Citation: Rakholiya S and Sonagara G. Feasibility of Modified Trouser/Pant for Improving Dressing Ability of Hemiplegic Patient. Int J Pharmacogn Chinese Med 2017, 1(4): 000120.
*Corresponding author: Rakholiya S, Assistant Professor, School of Physiotherapy, RK University, India, Email: shweta.rakholiya@rku.ac.in
Background: Stroke is one of the major non communicable diseases. The prevalence of stroke among populations ranges from 500 to 600 per 1, 00,000. Stroke is a major cause of long-term disability. About half of the patients surviving for three months after their stroke will be alive five years later, and one third will survive for 10 years. Approximately 60% of survivors are expected to recover independence with self-care, and 75% are expected to walk independently. It is estimated that 20% will require institutional care. The remainder will need assistance either by family, a close personal friend, or paid attendant.
Aim: To modify the trouser to make hemiplegic patient independent for their dressing
Method: The study will include 20 subjects with Hemiplegia who are volunteer to take part in the study and meet the inclusion criteria. The informed consent will be taken from the subjects, (Male) will receive specially designed specific outfit. Subjects will provide time for a trial of wearing modified outfits before they will include in the study. How much time they will take to wear routing clothing and specially design clothes should be measured with stop watch. The level of independence during dressing will be taken for each subject with regular clothing and modified clothing with dressing component of Functional Independent Measure (FIM).
Study Design: Experimental study
Results: Age mean was 43.3. Statically analysis shows that p value is 0.0004 so there is significance difference in wearing regular and modified trouser in time component. Statically analysis shows that p value is < 0.0001 so there is significance difference in wearing regular and modified trouser in dressing component of FIM. So this suggest that the modified clothes takes less time compared to regular clothing & FIM score has also been improved.
Conclusion: So this suggest that the modified clothes takes less time compared to regular clothing & Functional Independent Measure (FIM) score has also been improved.
Keywords: Hemiplegic; Modified outfits; Functional Independence Measure
Abbreviations: FIM: Functional Independent Measure; CVA: Cerebrovascular Accident; MRI: Magnetic Resonance Imaging; PMR: Physical Medicine and Rehabilitation; NMES: Neuromuscular Electrical Stimulation
IntroductionHemiplegia is a condition which affects one side of the body only-hemi comes from the Greek word meaning half [1].
The Prevalence of hemiplegia among populations ranges from 500 to 600 per 1, 00,000. Stroke is a major cause of long-term disability. Approximately 60% of survivors are expected to recover independence with self-care, and 75% are expected to walk independently. It is estimated that 20% will require institutional care. The remainder will need assistance either by family, a close personal friend, or paid attendant. The most common cause is stroke (CVA). Stroke can have different origins: the interruption of irrigation of part of the brain caused by a clot that blocks an artery or cerebral hemorrhage. They result in oxygen deprivation in a given area, in this case where the nerve cells die. Trauma can also cause hemiplegia brutal and immediate. Hemiplegia which occurs more gradually they are caused by brain tumors, infections (encephalitis and brain abscess) Figure 1 [2].
Hemiplegia caused by a lesion of the pyramidal tract. This is the main neural pathway that carries the motor orders. It is therefore a set of neurons involved in voluntary movement [3].
The pyramidal pathway begins in the brain at an area of nerve cells of pyramidal shape and joined with other nerve cells of the spinal cord. Pyramidal tract neurons then transmit their orders to LMN which carry them to the muscles. Before reaching the spinal cord, brain stem, the pyramidal tract changes sides. This explains that a lesion is localized on the side opposite the affected limb: left brain injury causes a right hemiplegia and vice versa.
Observed with Different Depending on the Location of the InjuryWhen the lesion in the brain cortex, this causes a disproportionate hemiplegia: the face and arms are predominantly affected. When the lesion is located in the white matter of the brain, this causes a proportional hemiplegia: arm and leg are affected similarly deficient. A brainstem lesion, it causes a paralysis of one side of the body and involvement of the face on the other side. In some cases the lesions, arm and leg are affected, in others only the arm or only the face.
When hemiplegia is partial and that movements are still possible, there is a decrease in muscle strength and mobility impaired, as manifested by clumsiness, trouble walking accompanied by a great tiredness and falls of one side. When hemiplegia is total, even less reflexes are abolished. However, the Babinski sign is present: when you touch the outside of the foot, it causes an extension of the big toe. In a healthy person, this stimulation leads to a bending of the big toe.
Hemiplegia is accompanied by changes in muscle tone: the muscles are stiff and overly contracted any (spastic hemiplegia) or conversely soft and flabby (flaccid hemiplegia). On the face, the damage to the muscles can result in a drooping eyelid or an asymmetric smile.
In Addition to Motor Disturbances, Hemiplegia is Characterized by the Appearance of Other SymptomsPain: There is pain associated with brain injury and localized pain in the affected limbs. Aphasia. People, who suffer from hemiplegia, even though the process of thinking and developing ideas is held, are struggling to find words and articulate. In addition, they may have difficulty understanding the meaning of words they hear or read them.
Disorders of the sphincters: A quarter of people with hemiplegia have sphincter disturbances resulting in either urinary incontinence or urinary retention, fecal incontinence is still. Sexual dysfunction: erection, ejaculation is compromised in many men with hemiplegia. Moreover, a decreased libido, especially at the beginning of the disability, is often found.
The immobility of paralysis arising Member is responsible for complications that specialists in physical medicine and rehabilitation at trying to prevent the initial management. The main complication remains on the loss of autonomy: everything must be done to try to recover mobility as complete as possible.
Among the Complications that can Occur after HemiplegiaPain in joints of immobilized different: The shoulder is often affected with a stiffening of the muscles (spasticity) and local inflammation. Moreover, the bones of people with hemiplegia are weakened and lose bone density (osteopenia) as the brain give rise to abnormal vascularization of bone. Finally, sitting in a wheelchair or bedridden status may promote pressure sores (skin necrosis at the points of support) and problems such as venous disorders of venous circulation, the risk of phlebitis and edema. The sphincter disturbances can cause infectious complications.
There are situations where the diagnosis is not obvious because the hemiplegia may present with subtle signs such as clumsiness or fatigability of muscles on one side of the body. So the doctor performs a series of examinations, and in particular the operation of Barre highlighting deficits on one leg or one arm or both. In the case of an unconscious person, the hemiplegia was found from different specific maneuvers.
Imaging studies, CT or magnetic resonance imaging (MRI) can detect the causes (aneurysm, tumor embolism,) cause brain damage. An electro encephalogram may give information about brain injury and their importance. A neuropsychological examination can identify possible cognitive impairment such as aphasia, common in cases of hemiplegia.
The treatments are based upon that of the cause to prevent worsening of the hemiplegia, see the roll back. Depending on whether a thrombosis (a clot blocking an artery) or hemorrhage treatment will be suitable but the urgency is the same.
The initial management is performed in specialized, neurovascular emergencies. Hemiplegia can be immediately serious respiratory complications, or even respiratory arrest indicating a breakdown assisted. Then, the main treatment of hemiplegia is rehabilitation, as early as possible to allow the recovery of certain deficiencies and prevent the occurrence of complications. This will complete rehabilitation, physical and cognitive, sensory, but also if necessary.
Beyond physiotherapeutic care can involve a speech in the presence of speech, if there is an orthopedics oculars disorders can be reeducated, an occupational therapist to find all the aid which may facilitate the actions of everyday life and promote the maintenance home in case of loss of autonomy.
The management of hemiplegia is a service that specializes in physical medicine and rehabilitation (PMR) by a multidisciplinary team. His goal: to ensure greater independence and find walking possible with physical therapy and improve communication through speech therapy. Several rehabilitation methods (Bobath, Kabat, Schepherd and Carr) can be put to work.
Occupational therapy can learn to perform everyday activities. Finally, psychological treatment is recommended since depression is very common in people with hemiplegia [4].
Hemiplegia that results from lesions of the brain and spinal cord can be severe and permanent. The distribution of the paralysis due to these lesions varies with the location of the lesion and always affects a group of muscles, never individual muscles. The paralysis never involves all of the muscles on one side of the body, even in the most severe forms of hemiplegia.
Hemiplegia resulting from stroke is usually permanent. Roughly 70% of individuals are able to regain some function of the hand in physical therapy (Bruno). In cases of head injury, there may be partial or near complete recovery. In other causes less acute in onset, recovery may be possible if the condition is treated promptly (removal of a brain tumor or treatment of a viral infection). The degree of recovery depends on the extent of the damage to the brain or spinal cord. In all cases, there is the possibility of some degree of recovery with appropriate rehabilitation (physical therapy).
In addition to physical limitations, the mental status of the individual is an essential element of recovery. Brain damage can cause loss of normal thought processes (cognitive disorders), and balance may be impaired. Even if the individual can think and speak clearly, the devastating loss of normal control of the body affects each individual differently, and a reactive depression is not uncommon. Sometimes control of emotions and behavior are impaired. Speech and behavioral therapies can result in some degree of recovery [3].
Individuals who suffer from hemiplegia may require various rehabilitation services, including physical therapy, occupational therapy, speech therapy, and orthotic management. Rehabilitation services should occur at a frequency of 2 to 3 times a week for 8 weeks.
Occupational therapy focuses on regaining the ability to perform activities of daily living. Individuals learn to perform tasks while sitting down on a kitchen stool. By instructing individuals in tasks such as these, occupational therapists also engage in balance retraining. Individuals also learn dressing and bathing techniques. Occupational therapists may order equipment to assist individuals. Occupational therapists also promote the return of upper extremity and hand function through a variety of activities. Often the upper arm separates (subluxes) from the shoulder girdle because of a loss of muscle tone. Occupational therapy may use neuromuscular electrical stimulation (NMES), in which electrodes provide external stimulation to the muscles to counteract this symptom. More frequently, individuals wear a hemi-sling that helps support the arm to prevent subluxation. Occupational therapists may stretch the upper extremities and teach self-stretching techniques so that the arm can regain maximum potential. Individuals also learn strengthening exercises and practice tasks that require the affected hand to bear weight, thus sending nerve impulses to the brain so that damaged neural paths can begin to heal. Individuals engage in tasks that require both hands, such as holding a cup with the hemiplegic hand while pouring a drink using the good hand. As function returns, individuals may engage in fine motor tasks such as handwriting.
Occupational therapists also are instrumental in helping an individual perform activities of daily living, such as housecleaning, gardening, and practicing arts and crafts. They also help individuals learn how to adapt to driving and provide on-road training, which may be an important consideration in returning to work. Physical therapy focuses on stretching and strengthening the hemiplegic side. Therapists may passively stretch the affected side. Individuals and their family members learn to perform a stretching and strengthening program for the legs. Physical therapy also focuses on transfer training. The therapist teaches the individual to bear weight evenly when sitting and standing so that the individual is aware of the hemiplegic side. Individuals also learn mobility techniques such as walking and climbing stairs while using a pyramid cane or 4-pronged cane. For those individuals who cannot walk, the physical therapist may order a special wheelchair, called a hemi-chair, which can be propelled using only the good arm because a special axle connects the wheels. Orthotic management may also be required for individuals to regain function. Occupational therapists may make an individual a night splint, which positions the thumb and fingers so that the hand forms the letter "C." This position places the hand in a functional position, allowing for full use of the hand if strength returns. An orthotics, which custom-fits braces and splints, may make an individual a leg splint to promote better control of the ankle and knee during ambulation.
Speech therapy may be required to strengthen the muscles of the face for improved speech and swallowing. Individuals learn to move the facial muscles in a balanced manner, both by manual assistance and visual cueing through the use of a mirror. Individuals perform tongue exercises to allow for better speech and eating. Activities such as sustained vocal expressions help individuals learn to speak with greater clarity. Individuals begin eating semi-moist, pureed food, which is easier to swallow, and progress to eating food rich in taste, smell, and texture to assist in the swallowing reflex. Individuals also learn to achieve sucking control and saliva production. Vocational therapists may help an individual with hemiplegia identify vocational strengths and develop resumes that highlight those strengths. Stroke vocational rehabilitation agencies may help an individual find a job that is tailored to his or her specific needs and appropriate for the degree of disability.
Individuals may need counseling by a psychologist or psychiatrist to help them adjust to their altered functional abilities and body image [3].
Work restrictions and accommodations will depend on job requirements and the level of activity involved. Wheelchair accessibility in and out of buildings and handicapped facilities may be needed. Although only one side of the body is affected in hemiplegia, activities that require coordination and balance are affected and may limit the individual's ability to perform physical work [3].
Dressing Difficulties after StrokeOccupational therapists traditionally give dressing practice to stroke patients during their stay in hospital, but despite this many are still unable to dress several weeks after admission to hospital. Edmans and Lincoln (1987) found that in a group of 150 stroke patients admitted consecutively to hospital and assessed at one month and two years after stroke, 41% and 36% respectively still required assistance to dress. Ebrahim and Nouri (1987) studied 120 patients at six months after the onset of stroke, to establish the extent and type of help provided by relatives and friends. Help was most often given for bathing (65%), dressing (54%), in the toilet (38%) and with feeding (21%).
In further analysis, Ebrahim and Nouri document that of those patients given help in dressing, 35% of wives were given help by their husbands and 61% of husbands were given help by their wives. This difference may have arisen because the husbands were more disabled than the wives but it is more likely to confirm the statement made by Kinsella and Ford (1985) reporting their study of hemi-mattention after stroke, that 'it can be easily seen that in dressing it is quicker and easier for the wife to dress the patient completely rather than leave him to struggle as far as he can before coming to his assistance. Further statistics on the prevalence of dressing difficulties following stroke include those based on the Frenchay Community Study by Wade, Langton-Hewer et al (1985): at one week after stroke 21% were independent, at three weeks 49% and at six months 69%. Different studies produce a varying frequency of difficulties, but they all confirm 4 the basic premise that dressing difficulties after stroke are common [5].
Tips for DressingFastenings: Ideally, choose clothes without fastenings, such as t-shirts, polo shirts, casual tops, and trousers or skirts with elasticized waste bands. Zips are extremely difficult to manage with one hand and are best avoided. When dressing, it is much easier to dress the affected side first, and undress last.
Buttons: It is possible to do up a button one-handed, but it takes practice. A latch hook maybe useful: insert the hook through the buttonhole, latch it into the shank of the button, and pull the button back through the hole. For buttoned shirt cuffs, stitch elastic hoops next to the button hole, and fasten the button through the elastic rather than the hole. This allows for the hand to pass through the cuff without needing to unfasten the buttons. You could also replace buttons with Velcro. Remove the buttons and stitch then back on over the buttonholes. Stitch Velcro circles behind the button holes and onto the material where the buttons used to be [6].
Need of the studyTo modify the trouser to make hemiplegic patient independent for their dressing
ObjectiveTo find out the effectiveness of specially designed outfits in hemiplegic patients in terms of change in level of independency in wearing & quickness in wearing.
MethodologyAnalysis was done graph pad prism 5.0 version for the analysis of time component paired t test was done and for dressing component of FIM was analyzed by mannwhitney u test Table 1, Graph 1.
Statically analysis shows that p value is 0.0004 so there is significance difference in wearing regular and modified trouser in time component Table 2, Graph 2.
Statically analysis shows that p value is < 0.0001 so there is significance difference in wearing regular and modified trouser in dressing component of FIM Table 3.
So this suggests that the modified clothes FIM score has also been improved compared to regular clothing Graph 3.
DiscussionThe Result of the present study indicates that modified trouser (dressing) is easier and comfortable for the patient to wear, there by rejecting the null hypothesis.
The analysis of time component for wearing modified trouser showed significant feasibility to wear in comparison with wearing regular trouser. This result support with those of Joanna Fletcher-Smith as lower body dressing performance correlated with physical impairment that has been overcome by modifying the regular trouser for the purpose of reducing patients’ effort in wearing lower body dressing. It also suggests that lower body dressing difficulties are likely to be influenced by physical disability. Therefore unsuccessful lower body dressing could be due to an inability to manage independent standing and dynamic standing balance, rather than being a result of cognitive impairment.
Here in this study, though patients are having physical disability, the modified trouser takes less time to wear than regular trouser and also indicates that modified trouser requires less assistance while wearing it, which has been concluded through dressing component of functional independent Scale.
Same study must be conducted with larger size.
Limitation of the StudySo this suggest that the modified clothes takes less time compared to regular clothing & FIM score has also been improved. There was significance feasibility of modified trouser/pant for improving dressing ability of hemiplegic patient.
SummaryStroke is one of the major non communicable diseases. To make the hemiplegic patient independent for the dressing, trouser modification is been done. The Experimental study includes 20 male subjects with Hemiplegia. Subjects were providing time for a trial of wearing modified outfits before they included in the study. Duration taken by the patient to wear the modify trouser and normal was measured with stop watch. The level of independence during dressing was taken for each subject with regular clothing and modified clothing with dressing component of FIM. Age mean was 43.3. Statically analysis shows that p value is 0.0004 so there is significance difference in wearing regular and modified trouser in time component. Statically analysis shows that p value is < 0.0001 so there is significance difference in wearing regular and modified trouser in dressing component of FIM. So this suggest that the modified clothes takes less time compared to regular clothing & FIM score has also been improved.
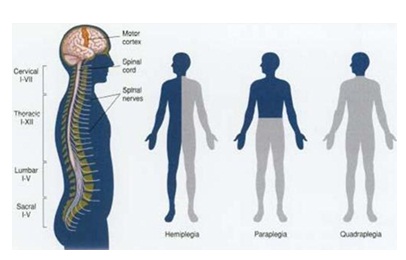
Figure 1: Hemiplegia.
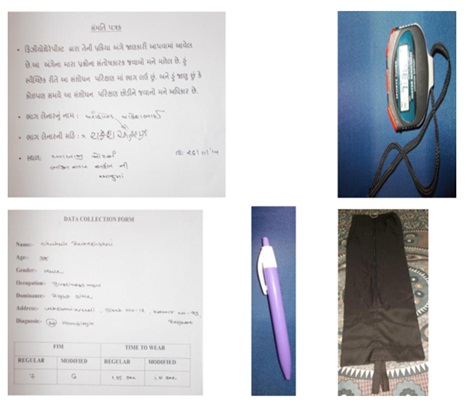
Figure 2: Materials.

Figure 3: Modified trouser with Patient.
Graph 1: Age Mean.
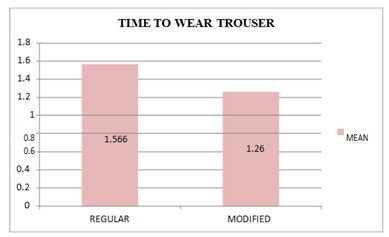
Graph 2: Analysis of Time to Wear Trouser.
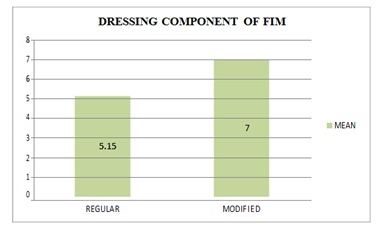
Graph 3: Analysis Dressing Component of FIM.
Table 1: Age Mean.

Table 2: Analysis of Time to Wear Trouser.

Table 3: Analysis Dressing Component of FIM.