Citation: Rabhi I, et al. Carpo-Metacarpal Dorsal Dislocation of the Fourth and Fifth Fingers in a Skier (A Case Report). J Ortho Bone Disord 2017, 1(5): 000130.
*Corresponding author: Rabhi I, Department of Trauma and Orthopedics, CHU Hassan II, 30000 Fez, Morroco, Email: ilyastraumato@gmail.com
The carpometacarpal dislocations are rare injuries. The authors report two cases of dorsal carpometacarpal joint dislocations of the ulnar two fingers, treated by closed reduction and fixation with percutaneous Kirschner-wires. A plaster splint with the wrist in neutral position was applied for six weeks. Active physiotherapy of the fingers was started from four weeks after surgery, with a satisfactory result.
Keywords: Dislocation; Carpometacarpal joints; Fracture
Carpometacarpal dislocations of the fingers are rare lesions. The first case was described by Rivingtonin 1873 [1]. The diagnosis is suspected clinically and confirmed by radiology. The treatment consists of an emergency reduction, then stabilize by pins in case of unstable lesion followed by a plaster immobilization.
Clinical caseMr K.R, a 25-year-old amateur skier, is admitted to the emergency department following a closed trauma of the right hand (direct fall on the metacarpal-phalangeal) causing pain and functional impairment. Clinical examination showed a slightedema and deformity of the dorsal aspect of the right hand. The frontal and lateral radiographs of the right hand showed a dorsal, pure, complete and insulated dislocation of the last two fingers (figure 1). The patient was operated on an emergency basis, under loco regional anesthesia, a trophy at the root of the limb. The closed-end carpometa carpal reduction was found to be easy, followed by a synthesis by pinning (figure 2). The wrist was immobilized by an intrinsic splint which was worn for six weeks, then the pins were removed after 8 weeks (figure 3). Active finger rehabilitation was undertaken as early as the fourth postoperative week, keeping the splint between the rehabilitation sessions. At 2 years of retreat, the functional result is satisfactory with good muscular strength and complete recovery of wrist mobility in flexion-extension and fingers. The work was resumed after three and a half months.
DiscussionThe carpo-metacarpal articulation is a very stable articulation [2,3]. All the authors agree to emphasize the extreme violence necessary to disorganize joint articulation [4]. This makes the carpo-metacarpal dislocation of the fingers a rare lesion. It concerns the young adult. Very violent trauma such as traffic accidents are the main ones. However, traumas of lower intensity, such as falls in height and punches, may cause dislocation of the moving metacarpal muscles [5].
If the diagnosis of this type of lesionis made urgently on aradiograph of the hand and the wrist of strict profile (although their interpretation is sometimes difficult) the prognosis is better. It is essential to carry out a strict profile incidence showing the direction of displacement of the metacarpal bases, an oblique incidence givingrise to mobile or fixed metacarpals and a frontal incidence. Some authors recommend complementary to modensitometry [2]. Reduction by external maneuvers with percutaneous pinning is a good treatment in the absence of associated vasculonuclear compression.
Spindle stabilization of the carpometacarpal spacing may be oblique, intramedullary or cross-shaped [5]. The result of these carpometacarpal dislocations treated urgently is good and leaves few sequelae [6-8]. Several complications have been reported in the literature, such as residual hand pain, decreased gripping force, subluxations and secondary displacements [9]. Lawlis and Gunther [5] reported that patients with dislocation of the four carpometacarpal joints performed better than those with dislocation of the second and third rays [5,10]. The fourth and fifth carpometacarpal joints must be inserted in slight flexion to preserve the curvature of the metacarpal arch [11,12].

Figure 1: X-ray of the hand and wrist in profile; Frontal and oblique showing a carpo-metacarpal dislocation of the fourth and fifth fingers.
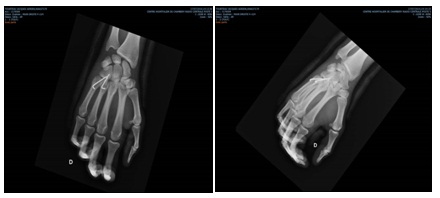
Figure 2: Postoperative control radiograph of the hand and wrist oblique and face incidence showing the reduction of the fourth and fifth finger carpal-metacarpal dislocation and stabilisation by two oblique pins.

Figure 3: X-ray of the hand face after removal of the two pins showing the integrity of the articular surfaces of the 4th and 5th radius.