Citation: Jan E and Kadmon I. Women's Decision Styles Relating to Breast Cancer: The Israeli Jewish Perspective. Nurs Health Care Int J 2017, 1(5): 000126.
*Corresponding author: Elisheva Jan, Deputy head nurse, Radiation Neuro-oncology Coordinator, Oncological Radiation Dept, Sheba Medical Center, Israel, Email: elishevajan@gmail.com
Background and Aim: The beginning of the new millennium was characterized by a wealth of research in the field of decision making encompassing the medical health professions, and including the nursing occupation. The aim of this study was to research the decision styles of Jewish, Israeli women.
Method: This study focused on Jewish Israeli women, over 18 years old. Women diagnosed with a possible breast tumor and before they were about to undergo a breast biopsy to diagnose this finding were approached by the researcher. The sample was a convenient sample. Eighty participants were recruited.
The recruited women were asked three questions: 1. What are the decision styles of women who were about to have a breast biopsy in all three sectors of the Jewish, Israeli culture? 2. What is the difference between all three sectors concerning all four decision styles? 3. What is the correlation between each style within all three sectors? Results: Due to the small sample size, especially for religious women, the results were limited. The findings agree with the limited literature in this field showing that religious women tend to seek advice from a religious community leader prior to making a decision about their medical condition, especially for the Deferring, Avoidance and Information seeking styles.
Conclusion and Implications for Oncology Nursing: It can be established from this study that religious women are a special group, both concerning their participation in medical studies, and their decision making style behaviour. Nurses are probably intuitively involved with women's decision making and can know and estimate their decision style beforehand. In the future, there should be more research on this population, especially in Israel, where few studies have been completed.
Keywords: Jewish Women; Breast cancer; Breast biopsy; Decision styles
The beginning of the new millennium was characterized by a wealth of research in the field of decision making within the various medical health professions. Specifically researching the decision styles of patients [1-3]. A decision style is the behavior of a person within their decision making process [4]. Professor Penny Pierce first explored the field of decision styles in the early 1990's. She described three decision styles: Deferrers, Delayers and Deliberators [4]. She later on added a fourth style, Information Seekers.
For the past 15 years, there have been few studies of this subject mainly describing the decision styles of woman with early stage breast cancer in various cultures and ages concerning their treatments [1,2,5].
In 2013, we conducted a study in Israel on this subject. This was a descriptive correlative research study. It's main objective was to identify the decision styles of Jewish, Israeli woman who were about to undergo a breast biopsy due to a suspected breast tumor [6]. The research was unique because Jewish, Israeli women differ significantly from other cultures. The Jewish culture is divided into four groups 1. Secular 2. Traditional Jews 3. Religious Jews and 4. Ultra orthodox religious Jews. Special emphasis was placed on the fourth group the Ultraorthodox religious Jews who have a unique and different behavior while making decisions concerning health issues [7,8].
This study addresses three questions: 1. What are the decision styles of women who were about to have a breast biopsy in all three Jewish, Israeli cultural groups (secular, traditional, religious which included also ultraorthodox)? 2. What is the difference between all three groups concerning all four decision styles (as described by Pierce, 1993)? [4] 3. What is the correlation between each decision style within all three groups?
During the study, we encountered a problem with the religious group mainly the ultra-orthodox. They were reluctant to participate in our research for various reasons [6]. Therefore, we had to combine the two different religious groups into one namely the "religious" sector.
MethodThe population of this study was Jewish Israeli women, over 18 years old. The sample was a convenient sample. Women who were diagnosed with a finding in their breast and were about to undergo a breast biopsy to diagnose this finding were approached by the researcher. Due to difficulties recruiting participants especially with the religious sector, we had gathered only 80 participants. The small response rate was because of anxiety before the medical procedure they were about to have and the results of the biopsy. Moreover, the fact that, religious women, and mainly the ultraorthodox among them, were not used to participating in medical research.
The bases for this study were the four decision styles as described by Pierce (1993) [4]. Two questionnaires were used in the current study: 1. MADS - The Michigan Assessment of Decision Style translated to Hebrew which was approved by the author. This Pre-Decision Portfolio Questionnaire was developed by Pierce in 1996 following the analysis of a grounded theory study of 48 women diagnosed with early breast cancer [4]. This instrument consisted of items collecting information from the participants relating to their socio-demographic background decision-making process and decision style relating to early breast cancer treatment and, had established content and construct validity [9].
In the present study we only used the Decision-making style questionnaire. The Michigan Assessment of Decision Style (MADS) which is a 16-item instrument [9] on a 5- point Likert scale to measure four key predecision behaviors. For MADS the Likert scale ranged from “strongly disagree” to “strongly agree (score 1 to 5, respectively). Two factors, Avoidance (α = 0.63) consisted of four items (total possible score = 20) and Deferring Responsibility (α = 0.76) consisted of three items (total possible score = 15), indicate a tendency or preference to minimize personal involvement in the decision and defer the responsibility to another.
The two remaining factors, Information Seeking (α = 0.80) consisted of four items (total possible score = 20) and Deliberation (α = 0.85) consisted of five items (total possible score = 25), indicate an inclination of the participants for being involved in the decision-making process and seeking information and structuring a systematic plan for making a decision [9,1].
This tool was used in various studies.
2. A demographic questionnaire developed by the researcher.
This study took place in a Women’s Health Care Center in a medical institution in the center of Israel. The study received approval from the ethical committee of the medical center where the study took place. The questionnaires were filled anonymously and no other identification was included.
ResultsOur findings are presented in relation to the 3 questions that were asked:
What are the decision styles of women who were about to have a breast biopsy in all three sectors of the Jewish Israeli culture (secular, traditional, religious)?We used a chi square test to find out if there is a difference in the distribution of the answers between the three sectors but only two questions from the MADS were statistically significant and there for we could not determine any conclusions of these differences. We also found that the reliability of each decision style was different for each of the three sectors thus making it impossible to determine the decision style of each sector (Table 1).
What is the difference between all three sectors concerning all four decision styles?Our hypothesis was that the women from the 3 sectors differ from each other in all 4 decision styles. To determine this hypothesis, we calculated the average of each decision style for each sector and compared between them using the ANOVA tests. Our conclusions were based on a significance of p = 0.05. We found no statistically significant difference between the 3 sectors in the avoidance style (p= 0.06) and the deferring style (p= 0.08). We do see that the avoidance style was close to the cut off line and if there had been more participants maybe it would have been statistically significant and maybe concerning this decision style there is a difference between the 3 sectors.
What is the correlation between each decision style within all 3 sectors?Our hypothesis was that among the women in the 3 sectors there is a correlation to all 4 decision styles. This was calculated by the Spearman correlation test (Table 2).
The results of this question show a significant statistical correlation between the secular sector and delaying, deliberation and Information seeking styles. It also shows a similar result with the Traditional sector. No significant statistical correlation was found with the religious group.
Summary and ConclusionsIt can be said, that the present study, in relation to the literature that exists, concerning health care decision making in Israel, the described style of decision making leans towards deliberating, delaying and information seeking among the secular and traditional sectors. However, in this study it was found that the Israeli religious Jews do not have a significant difference in the four decision styles that were described. It cannot be known if these women are not influenced by other factors which are common in this country with in this sector such as consulting rabbi’s or a spiritual and religious community leader. As described by Coleman (2009) [7] religious orthodox women mostly gave all the delegation of authority when having to make a decision concerning health issues to the religious leaders. In relation to the present research, if the number of religious women was greater, it may have shown a statistically significant difference between the styles of deferrers (women who prefer to make decisions with their doctors or other professionals) and deliberators (women who prefer to collect information before a decision is made). Therefore, it can be said that religious Jewish Israeli women would generally wish to collect more information regarding their breast cancer from a respected authority before making their own decision. However, in a difference from Jewish secular women, the authority they consult with may not be only a medical authority but a religious leader or someone respected by the religious community, and base their decision on both consultations, leaning more towards the religious leader’s advice.
LimitationsThe limitations of the present study are:
1. A small sample size
2. Recruiting women in only one institution
3. Poor participation of religious women
4. Limited literature in this area
5. Women, at this point of time, when the study was done, were undergoing a stressful situation.
Relevance to Oncology NursingIn the area of decision making, the whole psychosocial team should be involved. This includes nurses, psychologists, doctors and social workers. However, nurses are probably mostly involved with decision making of women and may know and estimate their decision style beforehand [10]. This study showed that also religious leaders such as a community rabbi may assist the Jewish religious woman in their decision making over their care.
Future ResearchFuture studies should be further done in the Israeli culture of religious Jewish women and should perhaps also examine what they think about their decision making style retrospectively [11]. Moreover, more qualitative studies should be done on this community to further investigate the themes and concepts underlying their decision-making style.
AcknowledgmentsAbove all, sincerely we would like to thank all the women who participated in this study. Our thanks are also to Prof. Penny Pierce, who kindly allowed us to use her questionnaire and to translate it to Hebrew. Also, we would like to thank Dr. Sarit Shimoni Kant for her kind help in reviewing the manuscript and Dr. Elite Levin, the professional statistician, who helped us with the statistical analysis and Dr. Ayala Hubert who advised during this study.
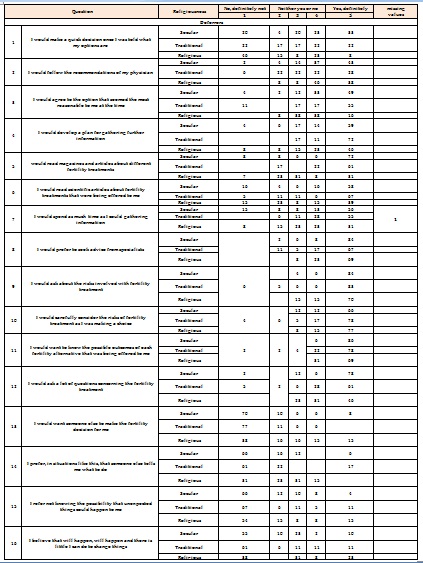
Table 1: Division of the women's decision styles by religiousness (%).
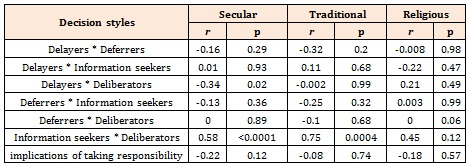
Table 2: Correlation scores between decision styles and women's religiousness.