Multimodal Anesthesia for Open Total Hysterectomy; Adjuvants, a New Horizon
39-year-old female patient with no history of chronic degenerative diseases. His current condition began in June 2020 with pictures of recurrent constipation accompanied by diffuse colicky abdominal pain, tomographic study abdominal injury that keeps adequate interface with the rectum, displacing and compressing the bladder, with approximate diameters of 31x24x21 centimeters, mass which it was probably ovarian-dependent. Surgical plan total hysterectomy bilateral salipingoophorectomy with abdominal omentectomy. Anesthetic management, multimodal anesthesia with the use of adjunctive medications for pain control. Multimodal anesthesia represents a current trend with great advantages for onco-gynecological surgeries; with better pain control, reducing the consumption of opioid use.
Relevant points
The presented clinical case is relevant as it gives us new approaches to the importance and advantages of the use of multimodal anesthesia in cancer surgeries. Knowing different therapeutic options with adjuvant medications for the management of post-anesthetic pain will improve your in-hospital recovery as well as reduce the use of opioid rescue. Oncological surgeries are frequent at the Hospital Central Sur de Alta Especialidad (HCSAE), which is why knowledge of this technique is extremely important.
Introduction
Gynecological oncology surgical techniques continue to evolve, but this often leads to more invasive and prolonged procedures, the vast majority of patients with gynecological- oncological pathologies are patients with important pre- existing comorbidities that require a comprehensive pre- anesthetic assessment, an intravenous plan. and specific post-operative, likewise, ideal pain control in the recovery period [1].
Balanced general anesthesia, is the strategy most frequently used in anesthesiology during the last decades, involves administering a combination of different agents to create the ideal anesthetic state in order to reduce the consumption of each drug that is administered, therefore reducing the likelihood of its side effects. This practice leads to a high consumption of opioids, which has generated a trend in the use of adjuvant drugs with specific objectives at the central nervous system level, such as magnesium sulfate, ketamine or dexmedetomidine, which is called multimodal anesthesia [2, 3, 4].
Presentation of the Case
This is a 39-year-old female patient, weighing 106 kg and 1.72 meters tall with no history of chronic degenerative diseases, with previous surgeries for ankle fracture and instrumented curettage, both without anesthetic complications. Her current condition began in June 2020 with pictures of recurrent constipation accompanied by diffuse colicky abdominal pain, which is why he goes for evaluation by a gastroenterologist who refers to gynecology, documenting abdominal injury in a tomographic study with lobed but defined edges that keep an adequate interface with the rectum, displacing and compressing the bladder, with approximate diameters of 31x24x21 centimeters, mass which It was probably ovarian-dependent, which is why it is evaluated by the oncological surgery service, who decides on a surgical approach, projecting a total hysterectomy + bilateral salipingoophorectomy with abdominal omentectomy as a surgical plan. A pre-anesthetic assessment is performed in which the following airway predictors are documented: interincisor distance of 3 cm. Mallampati I, Patil Aldreti: II, Bell house Dore: I, sterno-chin distance: I, mandibular protrusion> 1 centimeter, cylindrical neck, short, thick, with central trachea, mobile, not painful, without limitation of movement.
Laboratories: hemoglobin 13.1 g / dl, hematocrit 42.6%, platelets 427,000 u / l, glucose 83 mg / dl, creatinine 0.75 mg / dl, granting ASA III. After verification of the proper functioning of the anesthesiology team, the patient is admitted to the operating room, non-invasive monitoring is performed with baseline vital signs; blood pressure: 115/60 mmHg, heart rate: 78 beats per minute, oxygen saturation: 94%, electrocardiogram with leads in DII and V5 without data suggestive of arrhythmia, infarction or ischemia, after which, intravenous anesthetic induction is performed with; midazolam (25 mcg / kg), fentanyl (4 mcg / kg), lidocaine (1.5 mg / kg), propofol (1.5 mg / kg) and neuromuscular blocker rocuronium (1 mg / kg), previous latency of anesthetic drugs and pre-oxygenation by 5 minutes endotracheal intubation is performed with Mac # 3 blade, At the first attempt, without incidents or anesthetic complications, a Cormack Lehan I was observed, placing an endotracheal cannula type Murphy # 7.5 with 5 cc of pneumoblocking, with the following ventilator parameters; tidal volume of 475 milliliters, respiratory rate of 12-15, FiO2 60%, fraction inspiration expiration 1: 2 and PEEP 5 cm H2O. It was decided to perform invasive monitoring by means of a line in the right radial artery, with a peripheral catheter # 20 gauce without complications, performing gasometric control (Table 1).
Lidocaine-based infusions are established at 50 mcg / kg / min during the first hour, to later administer 30-15-12 mcg / kg / min respectively the following hours of the procedure, as well as magnesium sulfate at 15 mg / kg / min. hr, fentanyl at 0.039 mcg / kg / min and dexmedetomidine at 0. 8 mcg / kg / hr all drugs previously described by continuous infusion. Anesthetic maintenance with Sevoflurane at 0.8-0.6 MAC. Complementary medication is administered; ceftriaxone 1 gram, calcium gluconate 1 gram, ketorolac 60 milligrams, dexamethasone 8 milligrams, ondansetron 8 milligrams, paracetamol 1 gram. Fluid control, with a positive balance at a final 100 ml, (6200 ml admissions, 6100 ml discharges, with the need for two globular packs to exceed the permissible bleeding volume, with a final uresis of 1.42 ml / kg / hr ), and total bleeding of 1800 ml. paracetamol 1 gram. Fluid control, with a positive balance at a final 100 ml, (6200 ml admissions, 6100 ml discharges, with the need for two globular packs to exceed the permissible bleeding volume, with a final uresis of 1.42 ml / kg / hr ), and total bleeding of 1800 ml. paracetamol 1 gram. Fluid control, with a positive balance at a final 100 ml, (6200 ml admissions, 6100 ml discharges, with the need for two globular packs to exceed the permissible bleeding volume, with a final uresis of 1.42 ml / kg / hr ), and total bleeding of 1800 ml.
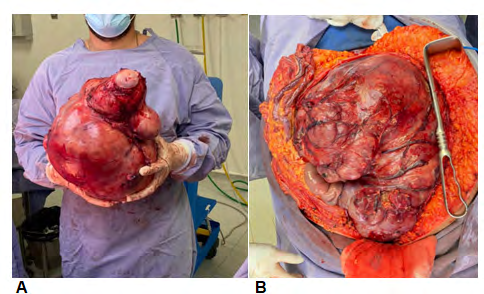
Prior to surgical wound closure, it was decided to infiltrate 135 milligrams of ropivacaine plus 100 milligrams of ketamine into the subcutaneous cellular tissue. Total surgical time: 390 minutes and 420 anesthetic minutes. A 10,250 kg tumor was obtained (Figure 1), which reported high-grade sarcoma in a trans-surgical pathology study. At the end of the surgical procedure, the patient was extubated after aspiration of secretions without complications, with the following final signs: blood pressure: 134/81, heart rate: 71, oxygen saturation: 96%, referring to 0/10 on the analogous pain scale (EAD).), Ramsay II. After 90 minutes in the post- anesthetic care unit, discharge to the treating service floor was decided with 1/10 EAD, without referring nausea or vomiting with physiological parameters of vital signs.
Follow-up is performed at 12, 24 and 48 hours after discharge for pain management, reporting a maximum ENA of 3/10 during the first 24 hours, decreasing to 0/10 in the 48 hours after surgery.
| HOUR | PH | PCO2 | PO2 | HCO3 | BE | HB | SO2 | LAC |
|---|---|---|---|---|---|---|---|---|
| 9:30 | 7.2 | 29.2 | 138.4 | 11.2 | -15.5 | 8.7 | 98.2 | 0.77 |
| 10:26 | 7.28 | 42.3 | 151.5 | 19.6 | -6.7 | 11.7 | 97.8 | 1.49 |
| 11:46 | 7.3 | 33.3 | 190.8 | 16.2 | -9.2 | 11.4 | 98.5 | 1.24 |
| 12:50 | 7.36 | 33.7 | 197.5 | 18.7 | -5.9 | 11.9 | 99.2 | 1.24 |
| 14:07 | 7.36 | 32.2 | 180.8 | 18.2 | -6.2 | 12 | 98.5 | 1.3 |
| 15:36 | 7.36 | 30.3 | 143.7 | 16.9 | -7.3 | 12.8 | 98.7 | 1.46 |
Table 1: Gasometric Control.
Discussion
This report describes a young patient undergoing a major onchosurgical procedure, who decides to decline regional anesthesia, limiting the benefit of analgesic control during and after surgery, despite this, the new trend of multimodal anesthesia is used. making use of adjuvant drugs, in this case; Magnesium sulfate, which acts mainly by blocking NMDA receptors, is used in infusion as a complement to reduce the dose of agents, as well as it manages to potentiate the effects of hypnotics on arousal and prolong neuromuscular blockers by blocking calcium channels [5, 6]. Dexmedetomidine improves the downward inhibition of nociceptive transmission by activating inhibitory interneurons that synapse with projection neurons in the dorsal horn of the spinal cord, as well as acting presynaptically to decrease the release of norepinephrine from neurons of the locus coeruleus [7]. In the case of lidocaine, the main objective is its action at the sodium channel level, it is believed that the mechanism by which perfusion lidocaine manages to act is its ability to block the release of neutrophils [8, 9]. Several studies have demonstrated the use of subcutaneous ketamine in the management of postsurgical pain [10, 11, 12], Sacevitch, et al. in a double-blind randomized clinical trial, at a dose of 1 mg / kg infiltrated into the surgical wound, pain was improved and its adverse effects decreased. Like its simultaneous use with dexmedetomidine at a dose of 1 mcg / kg, its subcutaneous application helps in the management of postsurgical pain [7]. In the case of dexmedetomidine, the main concern for its use as rescue and control of postoperative pain is the hemodynamic effect (bradycardia) that could limit its use in certain patients. However, Uusalo, et al. In a study published in 2018, they demonstrated a bioavailability after administration of 1 mcg / kg of dexmedetomidine of 81% with a plasma concentration of 0.1 ng / ml, establishing that the onset of the cardiovascular, sympatholytic and sedative effects of dexmedetomidine , were less abrupt after subcutaneous administration.
Conclusion
Multimodal anesthesia represents a current trend with great advantages for onco-gynecological surgeries; with better pain control, improving the consumption of the use of opioids, neuromuscular and halogenated blockers.
References
-
Munro A, Sjaus A, George RB (2018) Anesthesia and analgesia for gynecological surgery. Curr Opin Anesthesiol 31(3): 274-279.
-
Brown EN, Pavone KJ, Naranjo M (2018) Multimodal General Anesthesia: Theory and Practice. Anesth Analg 127(5): 1246-1258.
-
Do SH (2013) Magnesium: a versatile drug for anesthesiologists. Korean J Anesthesiol 65(1): 4-8.
-
Mulier J (2017) Opioid free general anesthesia: A paradigm shift? Rev Esp Anestesiol Reanim 64(8): 427- 430.
-
Beiranvand S, Karimi A, Haghighat Shoar M, Baghizadeh Baghdashti M (2020) The Effects of Magnesium Sulfate with Lidocaine for Infraclavicular Brachial Plexus Block for Upper Extremity Surgeries. J Brachial Plex Peripher Nerve Inj 15(1): 33-39.
-
Paula Garcia WN, OliveiraPaula GH, De Boer HD, Garcia LV (2021) Lidocaine combined with magnesium sulfate preserved hemodynamic stability during general anesthesia without prolonging neuromuscular blockade: a randomized, double-blind, controlled trial. BMC Anesthesiol 21(1): 91.
-
Afonso J, Reis F (2012) Dexmedetomidine: current role in anesthesia and intensive care. Rev Bras Anestesiol 62(1): 118-133.
-
Miralda I, Uriarte SM, McLeish KR (2017) Multiple Phenotypic Changes Define Neutrophil Priming. Front Cell Infect Microbiol 7: 217.
-
Nguyen GT, Green ER, Mecsas J (2017) Neutrophils to the ROScue: Mechanisms of NADPH Oxidase Activation and Bacterial Resistance. Front Cell Infect Microbiol 7: 373.
-
Tuchscherer J, McKay WP, Twagirumugabe T (2017) Low-dose subcutaneous ketamine for postoperative pain management in Rwanda: a dose-finding study. Can J Anaesth 64 (9): 928-934.
-
Kamali A, Zarepour Z, Shokrpour M, Pazuki S (2019) Comparison of intradermal Dexmedmotidine and subcutaneous Ketamine for post-surgical pain management in patients with abdominal hysterectomy. Eur J Transl Myol 29(1): 7873.
-
Schnaider TB, Vieira AM, Brandao AC, Lobo MV (2005) Intraoperative analgesic effect of epidural ketamine, clonidine or dexmedetomidine for upper abdominal surgery. Rev Bras Anestesiol 55 (5): 525-531.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index