Use of Bedside Lung Ultrasound in Critically Ill Patients
The importance of ultrasound diagnostics in intensive care units is based on the fact that it is a radiological examination method that does not involve the use of ionizing radiation, can be repeated several times in a short period of time, minimally invasive, simple to carry out, does not involve transporting the patient to the radiology service and enables immediate decision-making on diagnosis and further treatment of the patient. Bedside lung US (bLUS) can reliably identify pneumothorax, consolidation, atelectasis, interstitial syndromes, pleural effusions with a high degree of sensitivity. Experts consider it a reliable tool on the basis of which a clinical decision can be made. Chest radiography is the most commonly used visualization method of examination in intensive care units and is certainly used for the diagnosis of ARDS. Radiography cannot monitor changes in the interstitium in a short period of time but ultrasound can detect more discrete changes in the interstitium, which is important for making the decision to extubate the patient. Bedside lung ultrasound is a simple visualization technique for the detection and characterization of conditions in the lung parenchyma. It can detect pleural effusion, interstitial syndrome, pneumothorax with considerable sensitivity and can be a good prognostic criterion for patient extubation.
Introduction
The importance of ultrasound diagnostics in intensive care units is based on the fact that it is a radiological examination method that does not involve the use of ionizing radiation, can be repeated several times in a short period of time, minimally invasive, simple to carry out, does not involve transporting the patient to the radiology service and enables immediate decision-making on diagnosis and further treatment of the patient. Morphological diagnosis of the chest in a patient in the intensive care unit is very important and computed tomography (CT) is certainly the method of choice. Unfortunately, sometimes it cannot be done in difficult patients, so bedside ultra sound (US) is the method of choice for examining these patients.
Ultrasound examination of the lungs is based on the presence of artifacts, which are most often the origin of the high acoustic impedance of the gas in the lungs, which makes it impossible to examine the lungs in a healthy person.
Bedside lung US (bLUS) can reliably identify pneumothorax, consolidation, atelectasis, interstitial syndromes, pleural effusions with a high degree of sensitivity [1, 2, 3]. Experts consider it a reliable tool on the basis of which a clinical decision can be made [4]. Chest radiography is the most commonly used visualization method of examination in intensive care units and is certainly used for the diagnosis of ARDS. Radiography cannot monitor changes in the interstitium in a short period of time but ultrasound can detect more discrete changes in the interstitium, which is important for making the decision to extubate the patient [5, 6, 7]. Also, ultrasound is very important in the detection of septations in the pleural effusion that CT cannot detect, in the detection of the dynamic “air” bronchogram, which is important in the differential diagnosis of atelectasis, as well as in the diagnosis of diaphragm dysfunction during respiratory insufficiency. Due to all these reasons, there are numerous papers and evidence on the necessity of daily and routine use of lung ultrasound in intensive care units in order to make timely and optimal therapeutic decisions [8].
Technique
Ultrasound examination of the lungs is most often performed in the supine position with a linear probe of 5-13 MHz frequency on B and M mode. The US probe is positioned vertically over the chest wall in the intercostal space.bLUS evaluation is performed in three different areas of the thorax, anterior, lateral and posterior regions, divided by anterior and posterior axillary lines. View should be obtained in between the ribs so that the pleural line is visible. On B mode the “pleural line” is hyperechoic linear structure which slides craniocaudally with each breath and is usually located 0.5 cm below the rib line. This sliding pattern is referred to as “lung sliding”. On the M-mode, this line and the aerated lung below create the “seashore sign”.
Diagnostic Methods
There are two basic types of artifacts during bLUS that allow determination of aeration and state of the pulmonary interstitium: A and B lines.
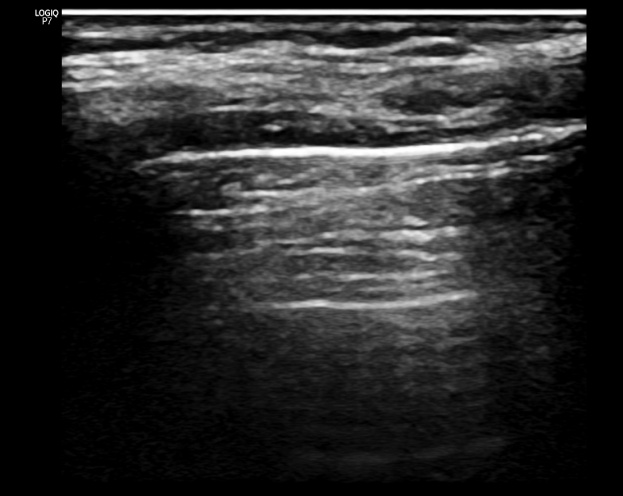
Alines are reverberation artefacts of a pleural line spreading through aerated lung parenchyma, they are parallel to the pleural line and always at the same distance from the pleural line. The presence of A lines is a sign of good lung aeration (Figure 1).
B lines are artefacts that starts from the pleural line, is perpendicular to the A line it interrupts, extends to the bottom of the ultrasound image, and has the morphology of a “comet tail” artifact (Figure 2).
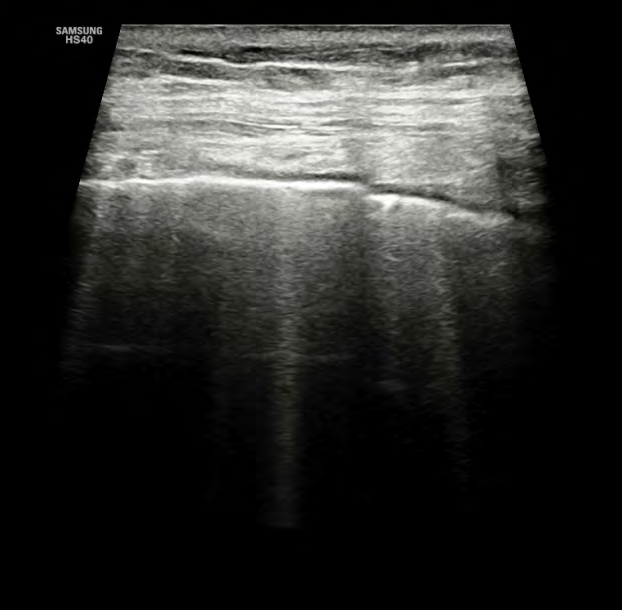
The presence of B lines indicates reduced aeration of the lung parenchyma and, in correlation with clinical findings, may correspond to an increased amount of extravascular fluid in the lungs leading to interstitial syndrome [9].
In intensive care units, bLUS usually involves calculating the LUS score. The LUS score is calculated on the basis of points assigned to each previously defined region of the lungs (6 per hemithorax)by existence of A and b lines as well as consolidation.Scoring is done as follows: 0 points - presence of A lines without B lines or few B lines, 1 point - predominance of B lines, 2 points - confluent B lines as evidence of the presence of fluid in the alveolar spaces and 3 points - consolidation with pulmonary hepatisation and dynamic “air” bronchogram, which suggests minimal lung aeration.
Main roles of bLUS are its ability to optimise ventilatory settings in adult respiratory distress syndrome (ARDS) patients, estimate the recruitable, poorly aerated pulmonary mass, monitor lung aeration during the weaning process, and give a reliable prognostic factor [10]. The LUS score is very helpful for monitoring lung aeration during intubation and is good prognostic parameter in evaluating the success of extubation. In fact, the number of B lines directly correlates with mortality while the LUS score correlates well with the amount of extravascular fluid in the lungs. In fact, LUS score is a good method in addition to radiological techniques (radiography, CT) for early diagnosis and monitoring of ARDS [10].
bLUS has entered routine clinical application in the detection of several pathological substrates in the chest: pleural effusion, pneumothorax, consolidation/atelectasis, interstitial syndrome and can be successfully used in the differential diagnosis of pulmonary edema, pneumonia and pulmonary thromboembolism.
Pleural effusion is very common in patients in intensive care units, and the role of ultrasound is in its detection, characterization and determination of quantity and monitoring over time. Detection of pleural effusion is most often done by placing a probe in the coronal plane of the middle axillary line for the evaluation of echogenicity above the diaphragm - if the zone is anechoic, it is most often a pleural effusion.
Pleural effusion is measured by placing the probe in the axial plane by determining the distance from the posterior paracostal pleura to the visceral pleura of the collapsed lung if it is typical posterior presentation, or if it is subpulmonary from the diaphragmatic pleura to the visceral pleura of the collapsed lung. If that diameter is over 50 millimeters, then it is considered to be more than 500 ml of effusion, and a possible thoracic paracentesis is decided on the basis of other clinical indicators. If the pleural effusion is completely anechoic, then it is most often a transudate, and if it contains septations, then it is most likely exudates (Figure 3).
Pneumothorax is the presence of air in the pleural space leads to separation of the visceral and parietal pleural interposition. This leads to a series of findings on lung US. There is absence of lung sliding and B-lines. Absence of lung- sliding has a sensitivity of 95% and 100% negative predictive value in diagnosing pneumothorax [11].
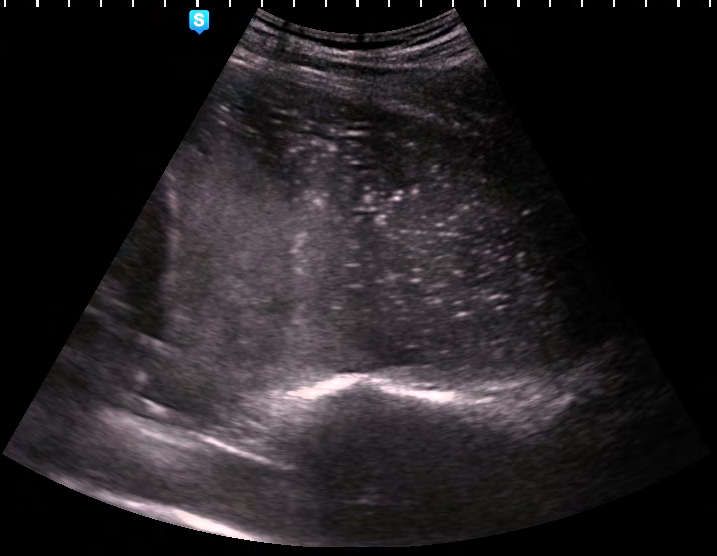
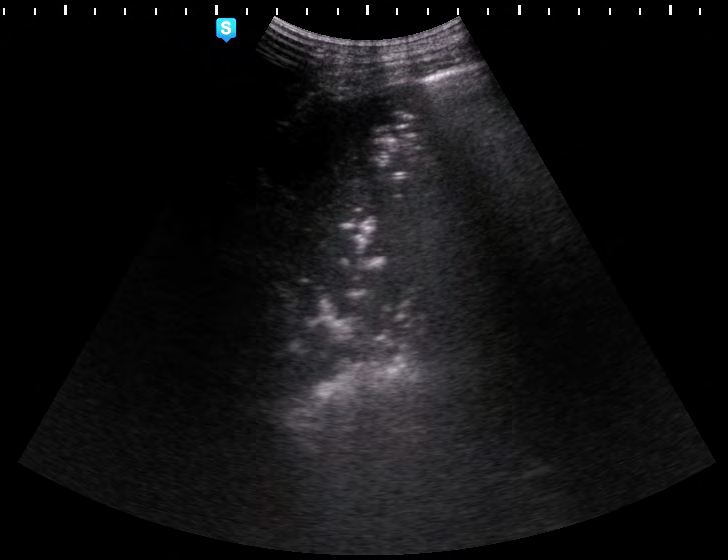
Atelectasis/pneumonia represents reduced lung aeration, which is hyperechoic in atelectasis and hypoechoic in pneumonia (Figure 4) with a dynamic “air” bronchogram sign that is not detected in atelectasis (Figure 5). Small areas of lung consolidations suggest pneumonia as a cause of hypoxic respiratory failure eighteen times more likely than a diagnosis of pulmonary embolism (PE).

Interstitial syndrome is the result of fluid accumulation in the pulmonary interstitium. On ultrasound examination, it is most often manifested as an increase in the number of B lines over 3 in one intercostal space. Detection of the number of B lines is important for monitoring the patient’s hydration status and may have significant therapeutic implications.
Conclusion
In conclusion, bLUS is a simple visualization technique for the detection and characterization of conditions in the lung parenchyma. It can detect pleural effusion, interstitial syndrome, pneumothorax with considerable sensitivity and can be a good prognostic criterion for patient extubation.
Conflict of Interest: Not applicable.
References
-
Lichtenstein D, Goldstein I, Mourgeon E, Philippe C, Philippe G, et al. (2004) Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 100(1): 9-15.
-
Volpicelli G, Mussa A, Garofalo G, Luciano C, Giovanna C, et al. (2006) Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am J Emerg Med 24(6): 689-696.
-
Bouhemad B, Liu ZH, Arbelot C, Mao Z, Fabio F, et al. (2010) Ultrasound assessment of antibiotic-induced pulmonary reaeration in ventilator-associated pneumonia. Crit Care Med 38(1): 84-92.
-
Xirouchaki N, Kondili E, Prinianakis G, Polychronis M, Georgopoulos D, et al. (2014) Impact of lung ultrasound on clinical decision making in critically ill patients. Intensive Care Med 40(1): 57-65.
-
Soummer A, Perbet S, Brisson H, Charlotte A, Jean Michel C, et al. (2012) Ultrasound assessment of lung aeration loss during a successful weaning trial predicts postextubation distress. Crit Care Med 40(7): 2064- 2072.
-
Bouhemad B, Brisson H, Le Guen M, Charlotte A, Qin L, et al. (2011) Bedside ultrasound assessment of positive end-expiratory pressure–induced lung recruitment. Am J Respir Crit Care Med 183(3): 341-347.
-
Caltabeloti F, Monsel A, Arbelot C, Hélène B, Wen Jie G, et al. (2014) Early fluid loading in acute respiratory distress syndrome with septic shock deteriorates lung aeration without impairing arterial oxygenation: a lung ultrasound observational study. Crit Care 18(3): R91.
-
Georgopoulos D, Xirouchaki N, Volpicelli G (2014) Lung ultrasound in the intensive care unit: let’s move forward. Intensive Care Med 40(10): 1592-1594.
-
Vetrugno L, Bove T, Guadagnin GM, Orso D, Alessandro B, et al. (2019) Advanced in lung ultrasound in critically ill patients. J Emerg Crit Care Med 3: 32.
-
Lichtenstein DA, Menu Y (1995) A bedside ultrasound sign ruling out pneumothorax in the critically III: lung sliding. Chest 108(5): 1345-1348.
-
Lichtenstein DA, Meziere GA (2008) Relevance of lung ultrasound in the diagnosis of acute respiratory failure. Chest 134(1): 117-125.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index