Comparison of Ultrasound Guided Interscalene Block vs Multimodal Analgesia in Shoulder Arthroscopic Surgeries- Prospective, Randomized Controlled Study
Introduction: Arthroscopic shoulder surgery is common and associated with severe postoperative pain. Interscalene block is recommended as a most effective method to relieve pain but it is also associated with some serious complications and expertise is required. This study assesses the efficacy, quality of analgesia postoperatively and overall satisfaction of patients undergoing shoulder arthroscopy by comparing ultrasound guided interscalene block with intraarticular morphine and local anaesthesia. Methods: This is prospective, single blind, randomized controlled study involving 46 patients randomized in ratio of 1:1 undergoing elective shoulder arthroscopy where GA was given in all patients out of which 23 received ISB before GA and 23 patients received intra articular injection of morphine and lignocaine at end of surgery. VAS score for postoperative pain, opioid consumption, PONV, patient satisfaction and readiness to discharge criteria was observed at 1, 4, 6, 12 and 24 hours post operatively in both groups. Results: In block group patient, VAS score was significantly low at 1 h and 6 h compared to non-block group. At 12 h both the group had a similar VAS score while at 24 h significantly high VAS score found in Block group patient. There was significant difference in opioid consumption in both groups. PONV, Complication rates, Satisfaction score and ready to discharge criteria were comparable in both groups. Conclusion: ISB provides effective analgesia in early postoperative period and it reduces the overall opioid requirement but the rebound pain which occurs after wearing off the block can reduce its overall benefit and satisfaction as compared to other modalities of multimodal analgesia. So, intra articular LA and opioid infiltration provides equivalent benefits in terms of post op analgesia and satisfaction.
Introduction
Shoulder arthroscopy has become common diagnostic and therapeutic procedure in recent times and also due to common sports injury [1, 2].
It is associated with severe post op pain due to soft tissue distension from saline irrigation, capsule tension, insertion of hardware, resection of bursal tissue etc [3].
Regional anesthesia is an attractive remedy to provide post op analgesia, early mobilization, decrease opioid consumption and physiotherapy [4]. ISB is commonly administered along with GA to provide postoperative analgesia and recent addition of USG machine provides real time image to make it a safe block. It may not be suitable to all patients, for example patients who did not give consent, history of drug allergy and difficult anatomy, respiratory insufficiency, existing vocal cord palsy.
It is also associated with few dreadful complications like total spinal, phrenic nerve block, BP and other nerve injury [2, 5]. Although rare, these complications can potentiate clinical and medico legal implications.
To give safe and effective block one need sophisticated machine, expert operator and it involves significant cost.
Peripheral opioid receptors have been identified which has led to use of intraarticular morphine as an analgesic. Local anaesthesia is also given as intraarticular for pain relief but chondrotoxicity can be there [6].
We compared 2 patient groups to evaluate effectiveness of ISB and multimodal analgesia including intraarticular morphine and local anesthesia. Our primary objective was to evaluate postoperative analgesia, vas scoring, opioid requirement, post op nausea vomiting and secondary objectives were any complications of interscalene block (like residual paralysis or motor deficits, pain, infection or swelling at block site) and patient satisfaction.
Materials and Methods
After approval from the Institutional Ethical Committee (IEC) [ref: IEC/2018/04/14 and Approval IEC date: 14th April 2018] and in accordance with Helsinki declaration, we conducted single blind, prospective, randomized controlled study involving 46 ASA 1 and 2 patients for shoulder arthroscopy.
Sample Size: The sample size was calculated based on the study done previously undergoing shoulder arthroscopic surgeries [7].
Assuming p value less than 0.05 to be significant and considering effect to be two sided we get $Z_{1-\beta} = 1.96$; and power of our study to be 90% we get $Z_{1-\beta} = 1.28$; considering an effect size(D) of 34 (from previous study), we get the sample size using formula:
$$n > 2 \cdot \frac{\left(Z_{\alpha} + Z_{1-\beta}\right)^2 \cdot SD^2}{D^2} > 9$$
where SD is the standard deviation.
Thus, we have to take at least 10 sample in each group. We had taken total of 46 patients. Since the number of patients in each group will be in the ration 1:1, total sample size will be 2x23=46. This was a single center study. Patients were randomly allocated into 2 groups using computer generated list of random numbers. Sequentially numbered envelopes were used for assignment of the groups. Anaesthesiologist who performed the procedure opened the envelop just before the procedure and another anaesthesiologist was assigned to collect the data and analyze the outcome who was unaware of the group.
Patients who were ASA grade 1 and 2, aged between 18 to 60 years and normal BMI were included in the study and who refused for the block, had any history of drug allergy used in study, any cardio-respiratory disease, ASA 3 and more, coagulopathy and mental illness were excluded from the study.
On admission patients were assessed for inclusion and exclusion criteria, preoperative examination and patients are explained for study details and informed written consent was obtained from all patients who participated in the study.
GA was administered in both the groups. One group received USG guided ISB before GA while other group received intraarticular injection at the end of surgery. All patients were monitored with standard monitoring.
Patients received ISB after explaining block details in OT under standard monitoring using GE ultrasound machine. High frequency linear probe used. After pre block scan, under strict aseptic precautions, block was conducted under local anaesthesia.
50 mm sonoplex needle along with additional nerve stimulus guidance was used to prevent nerve injury.
After identifying proper anatomy, needle passed under USG guidance in interscalene groove to reach 3 interscalene roots. After seeking current 0.5 mA and threshold 0.3 mA with negative aspiration, small injections of 0.375% Ropivacaine made at each root outside fascia. Total volume of LA maintained at 8 ml in all patients. All patients received standard GA using propofol 2-2.5 mg/kg, fentanyl 1 mcg/kg, atracurium 0.5 mg/kg and sevoflurane and endotracheal intubation was done and ventilated. Maintenance was done with sevoflurane, oxygen and air (MAC= 0.7-0.8). Fentanyl bolus dose of 25 mcg given when required during the procedure. Patients in both groups received Ondansetron 4mg, IV Paracetamol 1gm, 30 mg ketorolac intraoperatively.
In no block group, they received intra articular 15mg Morphine and 10 ml of 2% lignocaine by surgeon at the end of surgery.
All patient were extubated and monitored in PACU for vital parameters and pain score.
All patients were monitored and compared after surgery for VAS score at 1, 6, 12 and 24 hours, total opioid used, total doses of rescue analgesics in first 24 hours, PONV, complications (Dyspnea, Hoarseness of voice, nerve injury),
Results
overall satisfaction score and ready to discharge criteria.
Pain at rest or at movement was assessed by VAS on a scale of 1-10 with 1= no pain to 10= maximum pain and VAS score of 0-3 was considered as mild, 4-7 as moderate and 8-10 as severe. Patient satisfaction scores were assessed and graded on a 5-point scale (5= very satisfied, 4= satisfied,3= average, 2= dissatisfied and 1= poor) [8, 9].
Ready to discharge was assessed via modified PADSS score with score 9 or >9 can be discharged [10].
All patients received iv Paracetamol 1 gm and iv Diclofenac 75mg as a part of multimodal analgesia intraoperatively. Any patient who complained pain with VAS >4 was given iv Tramadol 50 mg as a first rescue analgesic and iv Pethidine 50 mg IM as second line rescue analgesic.
Statistical analysis was done using SPSS version 20. Categorical variables were expressed as Number of patients and percentage of patients and compared across the groups using Pearson’s Chi Square test for Independence of Attributes/ Fisher’s Exact Test as appropriate. Continuous variables were expressed as Mean, Median and Standard Deviation and compared across the groups using and Mann- Whitney U test. An alpha level of 5% was taken i.e. if any p value is less than 0.05 it has been considered as significant.
| GROUP | Age | Opioid Consumption Intraoperatively | Vas Score: 1 Hour | Vas Score: 6 Hours | Vas Score: 12 Hours | Vas Score: 24 Hours | Satisfaction | Ready to Discharge | |
|---|---|---|---|---|---|---|---|---|---|
| NO BLOCK | Mean | 49.52 | 90.22 | 6.52 | 3.3 | 2.74 | 3.26 | 4.04 | 8.96 |
| Median | 51 | 100 | 6 | 4 | 4 | 4 | 4 | 9 | |
| SD | 14.22 | 19.57 | 1.38 | 1.96 | 2.09 | 1.57 | 0.71 | 0.71 | |
| BLOCK | Mean | 49.48 | 61.96 | 0.26 | 1.52 | 3.96 | 4.61 | 4.26 | 8.87 |
| Median | 53 | 50 | 0 | 0 | 4 | 4 | 4 | 9 | |
| SD | 14.44 | 24.85 | 0.92 | 2.19 | 3.13 | 2.21 | 0.54 | 0.76 | |
| p value | 0.904 | <0.001 | <0.001 | 0.003 | 0.172 | 0.033 | 0.283 | 0.552 | |
| Significance | Not Significant | Significant | Significant | Significant | Not Significant | Significant | Not Significant | Not Significant |
Table 1: p value and significance of Age, intraoperative opioid consumption, VAS score at 1 hour, 6 hour, 12 hour and 24 hour, sa
| GROUP | Total | p Value | Significance | |||
|---|---|---|---|---|---|---|
| NO BLOCK | BLOCK | |||||
| Sex | M | 11(47.82) | 11(47.82) | 22(47.82) | 1 | Not Significant |
| F | 12(52.18) | 12(52.18) | 24(52.18) | |||
| ASA | I | 10(43.48) | 10(43.48) | 20(43.48) | 1 | Not Significant |
| II | 13(56.52) | 13(56.52) | 26(56.52) | |||
| RESCUE ANALGESIC (DOSES) | 0 | 3(13.04) | 12(52.17) | 15(32.61) | 0.008 | Significant |
| 1 | 18(78.26) | 9(39.13) | 27(58.7) | |||
| 2 | 2(8.7) | 2(8.7) | 4(8.7) | |||
| N/V (EPISODES) | 0 | 15(65.22) | 18(78.26) | 33(71.74) | 0.55 | Not Significant |
| 1 | 3(13.04) | 4(17.39) | 7(15.22) | |||
| 2 | 2(8.7) | 1(4.35) | 3(6.52) | |||
| 4 | 1(4.35) | 0(0) | 1(2.17) | |||
| 6 | 2(8.7) | 0(0) | 2(4.35) |
Table 2: p values and significance of Sex and ASA of patients in block and no block group, number of doses of rescue analgesics r
Tables 1 & 2 summarizes all the demographic and anaesthesia data. Data including age, sex and ASA were comparable in both groups. Mean age of patients was 49.52 in no block group while it was 49.48 in block group. 43.48% of patients were ASA1 in both groups while 56.52% was ASA2 in both the groups.
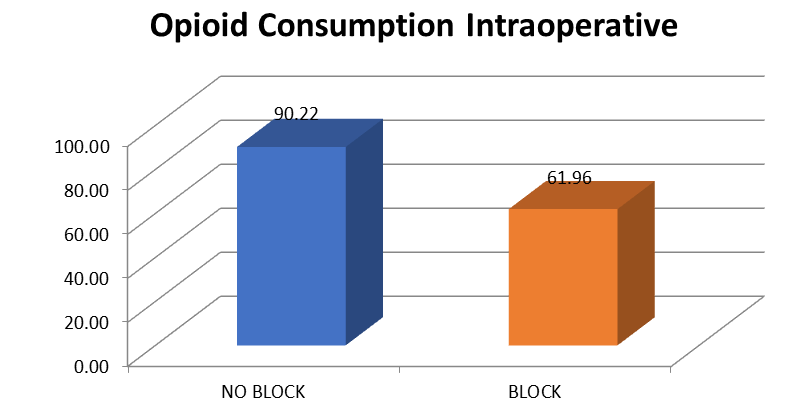
Mean intra operative opioid consumption was significant in No block group patients compare to block group. Mean opioid in block group was 61.6 µg compare to 90.22 µg in no block group which was statistically significant (p<0.001) (Figure 1).
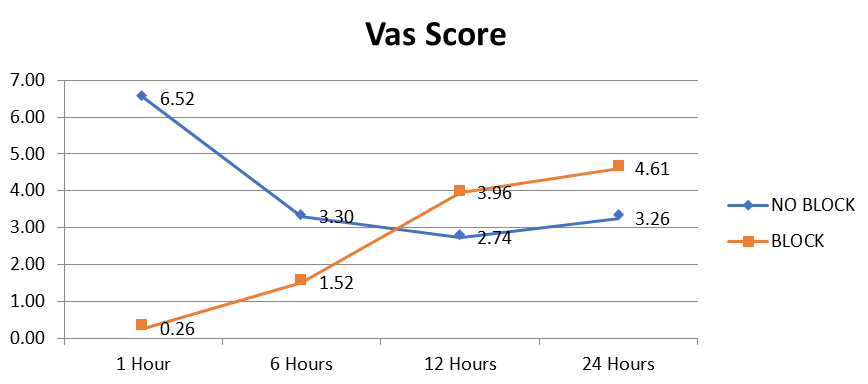
Mean VAS score at 1 h after surgery was 6.52 in no block group (with severe pain in 9 patient) compared to 0.26 in block group. It was statistically significant with p<0.001.
At 6 h mean VAS score was 3.3 in no block group compared to 1.52 in block group (with no patient complained of severe pain) as compared to 1 in block group which was statistically significant with p<0.003. 13 patients had moderate pain in no block as compared to 3 patients in block group. Severe pain occurred in one patient of block group.
At 12 h, there was increasing trend in VAS score among block group patients compared to non-block group. Mean VAS in block group was 3.96 as compared with 2.94 in non-block group patients although it was statistically not significant. 8 patients had moderate pain in block group compared to 12 patients in non-block group. Interestingly 5 patients had severe pain in block group compared to none in No block group.
At 24 h, VAS score was 4.61 in block group of patients compared to 3.26 in non-block group of patients which was statistically significant (p value <0.033). 14 patients complained moderate pain in each group and 4 patient complained severe pain in block group compared to none in No block group (Figure 2).
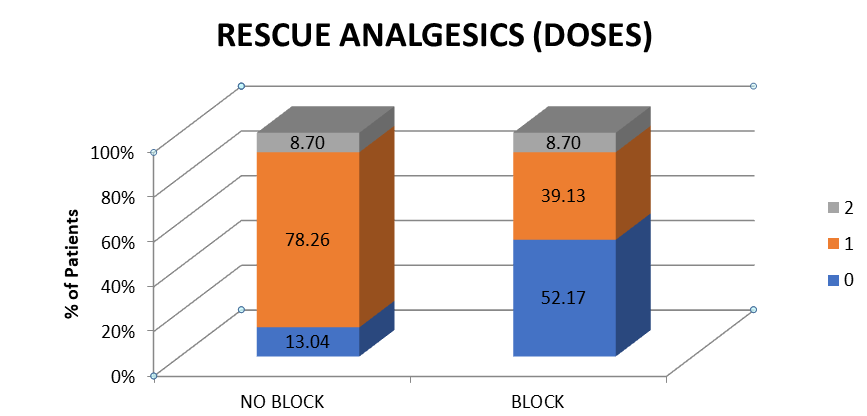
As shown in Table 2, significant patients required one rescue dose of analgesics. In Non block group, 18 patients required additional one dose of rescue analgesics compared to 9 patients requiring one dose in block group which was statistically significant (p value<0.008). Only 2 patients in both the groups required 2nd dose of rescue analgesics (Figure 3).
Postoperative nausea and vomiting were comparable in both the groups. Only one patient reported minor complication related to block.
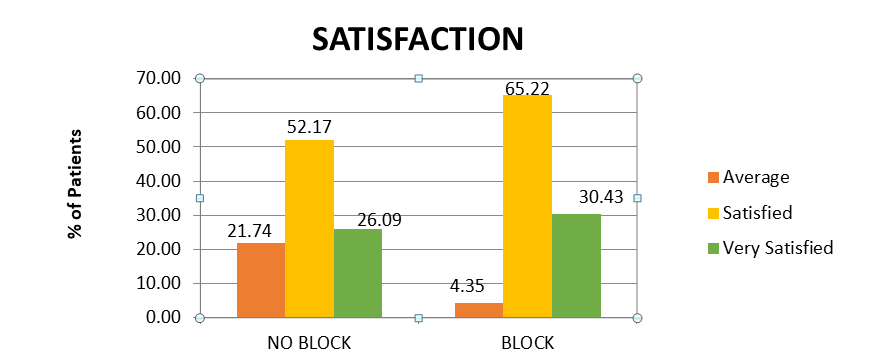
Satisfaction score were statistically comparable in both the groups with mean 4.04 score in No block group compared to 4.26 score in block group. In No block group, out of 23 patients, 6 patients were very satisfied, 12 were adequately satisfied and 5 average satisfied. In Block group, 7 patients were very satisfied, 15 adequately satisfied and
1 patient average satisfied. These results were statistically insignificant (Figure 4).
Among 23 patients in each group, 19 patients in No block group fulfilled ready to discharge criteria after 24 hours compared to 15 patients in block group which was statistically not significant.
Discussion
Shoulder arthroscopy is associated with moderate to severe post-operative pain. Around 30-70% has been associated with severe pain [11]. ISB for shoulder surgery is commonly administered in conjunction with GA, with the block performed primarily for postoperative analgesia. It is one of the most efficient technique to reduce the postoperative pain [12, 13, 14, 15].
Although interscalene block is one of most effective and recommended technique to provide postoperative analgesia, it has a potential for some rare but serious complications. It can be associated with various complications like Horner’s syndrome, subarachnoid/ epidural injection, pneumothorax, phrenic nerve palsy, injection into vertebral artery [2].
But ultrasound guidance has reduced the number of complications and improves the success rates.
ISB also involves expensive machine, nerve stimulator, special needles, skilled person and additional cost.
We found VAS score was low in block group only till 6 hours while at 12 h VAS score was comparable in both groups. Importantly at 24 h, situation is reversed with high pain score in patients who received ISB. More patients complained of severe rebound pain in block group despite giving multimodal analgesia. This was mainly between 12 h -24 h of the surgery. That’s why we found that vas score was higher at 24 h in block group.
Dada O, et al. [16] concluded that rebound pain characterized by hyperalgesia after block wears off negates the benefits of regional anaesthesia for orthopaedic surgeries. In other studies it has been found that Rebound pain may occur after 8 – 24 h which is irrespective of type of local anaesthetic, concentration and volume [17, 18, 19, 20]. This was concurrent with our study.
We found that significant patients required rescue opioid analgesic in no block group. The requirement of opioids was reduced in block group intraoperatively and early postoperative period but needed more after block wears off. Findings were similar to various studies which shows that upper extremity block provides effective intraoperative and early postoperative analgesia, therefore reducing the amount of rescue opioids analgesics [21, 22].
Incidence of PONV was low in our study. This may be due to small sample size but it was consistent with previous studies of Hazdic, et al. and Shah, et al. who also reported low PONV scores [23, 24].
Ultrasound guided nerve blocks requires shorter onset with more effective blockade as compared to blind or nerve stimulation techniques [25]. Direct visualization of the nerve roots helps in reducing the dose of local anaesthesia therefore decreasing the complications due to larger amount of drug like phrenic nerve palsy, possible intravascular injection and damage to surrounding tissue [25, 26]. So in our study also ultrasound has improved the efficacy with no major complications. We found one complication in block group patient. One patient had persistent hiccups postoperatively for 1 week and got relieved by the treatment with chlorpromazine. We did not find any complication in No block group related to anaesthesia.
We found higher satisfaction score in no block group. This is contrary to normal belief that patients are more satisfied if they receive nerve block. This could be due to lack of breakthrough pain, continuous analgesia, and better quality of sleep. Previous studies claimed that patients were more satisfied in block group could be because of low incidence of complications along with patient’s interest of getting home early [24, 27]. We found overall satisfying score statistically insignificant.
We also found that more patients in No block group achieved discharge readiness as compared to patients who received ISB. This is contradictory to belief that patients are ready to discharge early when they receive nerve block. Zoremba, et al. [28] also found that addition of interscalene block to GA for shoulder arthroscopy did not enhance fast track capability.
Thus, in our study we found that initial low VAS score till 6 hours post operatively in block group, but due to breakthrough pain, the VAS score escalates after 12 hours in block group and at 24 hours patient experience more pain in block group.
Although ISB will still hold a place for shoulder surgeries in specific subset of patients since all proximal plexus blocks like ISB has the potential to block neighbouring sympathetic ganglion via stellate ganglion. Sympathetic nervous system has good role in acute postoperative pain but multimodal approach nonetheless provided adequate overall clinical results with high degree of patient satisfaction. With less complications, low episodes of PONV and utilization of multimodal analgesia patients were comparable in both the groups for discharge readiness.
Our study has certain limitations. Primarily, it is possible that we were unable to assess fluctuating pain levels in between the study time intervals. Also, this study was done on a relatively lesser number of patients, further studies warranted with larger sample size to strengthen the results.
Conclusion
Although ISB is very effective, relatively safe at expert hand in providing postoperative analgesia in shoulder arthroscopy patients, we found it is only effective in initial few hours. Rebound pain actually diminished most benefits of ISB and it affects quality of sleep and reduces overall satisfaction in patients who received ISB. Although we did not find any major complication in block group, it is complex, costly, time consuming and potential for serious complication at times.
So, simple measure like standard multimodal analgesia along with intra articular morphine injection with local anesthesia provides equivalent benefits in terms of post op analgesia in patient undergoing shoulder arthroscopy without PONV, similar overall satisfaction score and discharge criteria.
- Acknowledgements: None
- Financial Support and Sponsorship: Nil.
- Conflicts of Interest: Nil.
References
-
Farmer KW, Wright TW (2015) Shoulder Arthroscopy: The Basics. J Hand Surg Am 40(4): 817-821.
-
Beecroft CL, Conventry DM (2008) Anesthesia for shoulder surgery. Contin Educ Anaesth Crit Care Pain 8(6): 193-198.
-
Kim CW, Kim JH, Kim DG (2014) Factors affecting pain pattern after Arthroscopic Rotator Cuff Repair. Clin Orthop Surg 6(4): 392-400.
-
Hewson DW, Oldman M, Bedforth NM (2019) Regional anaesthesia for shoulder surgery. BJA Educ 19(4): 98- 104.
-
Pani N, Routray SS, Pani S, Mallik S, Pattnaik S, et al. (2019) Post-operative analgesia for shoulder arthroscopic surgeries: A comparison between inter-scalene block and shoulder block. Indian J Anaesth 63(5): 382-387.
-
Dragoo JL, Braun HJ, Kim HJ, Phan HD, Golish SR, et al. (2012) The In Vitro Chondrotoxicity of Single-Dose Local Anesthetics. Am J Sports Med 40(4): 794-799.
-
Singelyn FJ, Lhotel L, Fabre B (2004) Pain relief after arthroscopic shoulder surgery: a comparison of intraarticular analgesia, suprascapular nerve block, and interscalene brachial plexus block. Anaesth Analg 99(2): 589-592.
-
Klein SM, Nielsen KC, Greengrass RA, Warner DS, Martin A, et al. (2002) Ambulatory discharge after long- acting peripheral nerve blockade: 2382 blocks with ropivacaine. Anaesth Analg 94(1): 65-70.
-
Nielsen KC, Guller U, Steele SM, Klein SM, Greengrass RA, et al. (2005) Influence of obesity on surgical regional anaesthesia in the ambulatory setting: An analysis of 9,038 blocks. Anaesthesiology 102(1): 181-187.
-
Chung F (1995) Discharge criteria-a new trend. Can J Anesth 42(11): 1056-1058.
-
Moote CA (1994) The prevention of postoperative pain. Can J Anaesth 41(6): 527-533.
-
Brown AR, Weiss R, Greenberg C, Flatow EL, Bigliani LU, et al. (1993) Interscalene block for shoulder arthroscopy: comparison with general anesthesia. Arthroscopy 9(3): 295-300.
-
Alessio D JG, Rosenblum M, Shea KP, Freitas DG (1995) A retrospective comparison of interscalene block and general anesthesia for ambulatory surgery shoulder arthroscopy. Reg Anesth 20(1): 62-68.
-
Feigl GC, Anderhuber F, Dorn C, Pipam W, Rosmarin W, et al. (2007) Modified lateral block of the suprascapular nerve: a safe approach and how much to inject? A morphological study. Reg Anesth Pain Med 32(6): 488- 494.
-
Kempen PM, O’Donnell J, Lawler R, Mantha V (2000) Acute respiratory insufficiency during interscalene plexus block. Anesth Analg 90(6): 1415-1416.
-
Dada O, Gonzalez Zacarias A, Ongaigui C, Echeverria- Villalobos M, Kushelev M, et al. (2019) Does Rebound Pain after Peripheral Nerve Block for Orthopedic Surgery Impact Postoperative Analgesia and Opioid Consumption? A Narrative Review. Int J Environ Res Public Health 16(18): 3257.
-
Namdari S, Nicholson T, Abboud J, Lazarus M, Steinberg D, et al. (2018) Interscalene block with and without intraoperative local infiltration with liposomal bupivacaine in shoulder arthroplasty: A randomized controlled trial. J Bone Joint Surg Am 100(16): 1373- 1378.
-
Taeha R, Tae KB, Hae KJ (2015) Comparison between ultrasound-guided supraclavicular and interscalene brachial plexus blocks in patients undergoing arthroscopic shoulder surgery - a prospective, randomized, parallel study. Medicine 94(40): e1726.
-
Abdallah FW, Halpern SH, Aoyama K, Brull R (2015) Will the Real Benefits of Single-Shot Interscalene Block Please Stand Up? A Systematic Review and Meta-Analysis. Anesth Analg 120(5): 1114-1129.
-
Lee SM, Park SE, Nam YS, Han SH, Lee KJ, et al. (2012) Analgesic effectiveness of nerve block in shoulder arthroscopy: comparison between interscalene, suprascapular and axillary nerve blocks. Knee Surgery, Sports Traumatology Arthroscopy 20(12): 2573-2578.
-
Candido KD, Knezevic NN (2011) All adjuvants to local anesthetics were not created equal: animal data evaluating neurotoxicity, thermal hyperalgesia, and relevance to human application. Reg Anesth Pain Med 36(3): 211-212.
-
Sunderland S, Yarnold CH, Head SJ, Osborn JA, Purssell A, et al. (2016) Schwarz SK. Regional Versus General Anesthesia and the Incidence of Unplanned Health Care Resource Utilization for Postoperative Pain After Wrist Fracture Surgery: Results From a Retrospective Quality Improvement Project. Reg Anaesth Pain Med 41(1): 22- 27.
-
Hadzic A, Williams BA, Karaca PE, Hobeika P, Unis G, et al. (2005) For outpatient rotator cuff surgery, nerve block anesthesia provides superior same-day recovery over general anesthesia. Anesthesiology 102(5): 1001-1007.
-
Shah A, Nielsen KC, Braga L, Pietrobon R, Klein SM, et al. (2007) Interscalene brachial plexus block for outpatient shoulder arthroplasty: Postoperative analgesia, patient satisfaction and complications. Indian J Orthop 41(3): 230-236.
-
Gorlin A, Warren L (2012) Ultrasound-Guided Interscalene Blocks. J Ultrasound Med 31(7): 979-983.
-
Brattwall M, Jildenstål P, Warrén Stomberg M, Jakobsson JG (2016) Upper extremity nerve block: how can benefit, duration, and safety be improved? An update. F1000Res 5: F1000.
-
Fontanaa C, Donatoa AD, Giacomoc GD, Costantinic A, Vitac AD, et al. (2009) Postoperative analgesia for arthroscopic shoulder surgery: a prospective randomized controlled study of intraarticular, subacromial injection, interscalenic brachial plexus block and intraarticular plus subacromial injection efficacy. Eur J Anaesthesiol 26(8): 689-693.
-
Zoremba M, Kratz T, Dette F, Wulf H, Steinfeldt T, et al. (2015) Supplemental Interscalene Blockade to General Anesthesia for Shoulder Arthroscopy: Effects on Fast Track Capability, Analgesic Quality, and Lung Function. BioMed Res Int 2015: 325012.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index