Anaesthetic Management of a Patient with Von-Hippel-Lindau Syndrome: A Conglomeration of Perplexities
Von-Hippel-Lindau (VHL) syndrome is an autosomal dominant disease with multisystem involvement. Tumours associated with VHL include, hemangioblastomas of the spine and brain, retinal capillary hemangioblastomas, renal cell carcinoma, pheochromocytoma, and neuroendocrine tumours of pancreas. We present a case of a 54 year old female second-degree uterovaginal prolapse scheduled for laparoscopic assisted vaginal hysterectomy. She was diagnosed with adult polycystic kidney disease, pheochromocytoma, parathyroid adenoma, vertebral hemangioma and multiple renal and hepatic cysts. Though genetic testing was not feasible, the co-existing systemic manifestations in this patient were strongly suggestive of Von Hippel Lindau syndrome. Owing to the multi-morbidities, central neuraxial block was deemed appropriate as opposed to general anaesthesia. In concert with the surgeons, it was decided to change the surgical plan to vaginal hysterectomy and avoid adrenaline infiltration at the surgical site, as it is known to precipitate arrythmias. We placed an intra-arterial catheter for continuous blood pressure monitoring before administration of the subarachnoid block and co-loaded the patient with fluids to avoid any drastic hypotension. The patient remained hemodynamically stable throughout the procedure, which could be attributed to extensive pre-operative work-up multi-disciplinary pre-operative optimization and synergistic management with surgical team. Providing anaesthesia to patients with multisystem involvement such as Von Hippel Lindau syndrome can be very challenging. Meticulous pre-anaesthetic evaluation and pre-operative optimization are often crucial. A multidisciplinary approach is often employed to achieve the best possible pre-operative functional status of these patients. Well-coordinated team with flexibility in management tailored to the patient helps achieve the best possible outcomes. Disclaimer: Informed consent was obtained from the patient prior to publication Main Points • Von-Hippel-Lindau (VHL) syndrome is an autosomal dominant disease with multisystem involvement; associated tumours include hemangioblastomas of the CNS, retinal capillary hemangioblastomas, renal cell carcinoma, pheochromocytoma, endolymphatic sac tumours of the middle ear, serous cystadenomas and neuroendocrine tumours of pancreas. • Providing anaesthesia to patients with multisystem involvement such as Von Hippel Lindau syndrome can be very challenging. Meticulous pre-anaesthetic evaluation and pre-operative optimization are often crucial. • A detailed anaesthetic plan, tailored to each patient, has to be formulated in elective cases, after an extensive work-up of the associated tumours. • Extensive pre-operative work-up, a multi-disciplinary approach towards pre-operative optimization and synergistic management with surgical team remains vital in minimizing peri-operative complications.• Anaesthetic implications are often at the nexus of surgical outcomes, hence, proper communication with the surgical team and arrival at a joint plan is crucial.
Introduction
Von-Hippel-Lindau (VHL) syndrome is an autosomal dominant disease with multisystem involvement; associated tumours include hemangioblastomas of the central nervous system, retinal capillary hemangioblastomas, clear cell renal cell carcinoma, pheochromocytoma, endolymphatic sac tumours of the middle ear, serous cystadenomas and neuroendocrine tumours of pancreas [1]. When VHL is associated with pheochromocytoma, clinical features related to abnormal catecholamine production such as tachycardia and labile blood pressure may be noted. These patients present with episodic/continuous hypertension based on the pattern of catecholamine secretion.
We present a case of a 54 year old female with adult polycystic kidney disease, pheochromocytoma, parathyroid adenoma, a D7 vertebral hemangioma and multiple renal and hepatic cysts. Though genetic testing was not feasible, the co-existing systemic manifestations in this patient were strongly suggestive of Von Hippel Lindau syndrome.
Case Report
A 54 year old lady with 2nd degree uterovaginal prolapse was scheduled for a laparoscopy assisted vaginal hysterectomy. A pre-anaesthetic evaluation revealed that she was a diagnosed case of adult polycystic kidney disease, for which she had undergone a left-sided nephrectomy 12 years ago. She had presented with episodic headaches, palpitations and sudden bouts of profuse sweating 5 years ago; further evaluation confirmed diagnosis of pheochromocytoma by an MIBG scan. She was also diagnosed to have ischemic heart disease with a coronary angiogram suggestive of mild slow flow in the coronary vasculature 1 year ago. She was regularly followed up by the endocrinologist and was on multiple oral medications (cilnidipine, metoprolol, rosuvastatin, prazosin and losartan) for her co-morbidities. She gave history suggestive of moderate effort tolerance. On physical examination, she was hemodynamically stable with a heart rate of 105 beats/min, blood pressure of 130/90 mm Hg, room air saturation of 98% and an unremarkable cardiovascular examination.
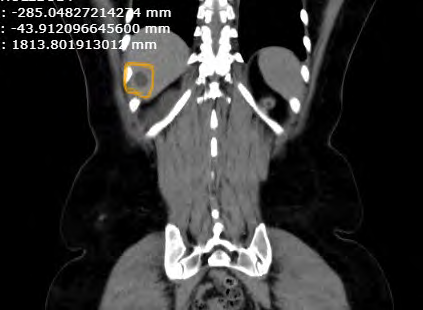
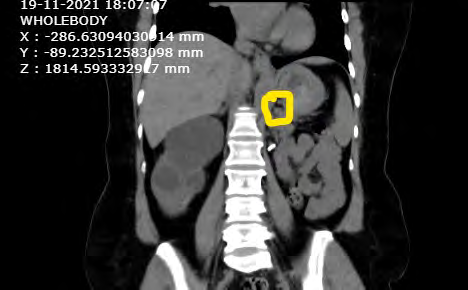
On routine evaluation, she was diagnosed to have hypercalcemia. Further evaluation revealed well- defined nodules in the ultrasound neck- suggestive of parathyroid adenomas. Imaging studies ruled out cerebellar hemangioblastomas; however spinal canal stenosis with a D7 vertebral hemangioma was noted. Computerized Tomography of Kidney, Ureters and Bladder was suggestive of multiple enlarged cortical and exophytic cysts, measuring around 7 x 6.5 x 7.5 cm which were replacing the renal parenchyma in the right kidney and an absent left kidney. A hypodense lesion measuring 7.3 x 6.4 mm was noted in the medial lobe of right adrenal gland. Multiple hepatic cysts were noted in V and VI segments of the liver.
After pre-anaesthetic evaluation, we had further advised: Holter monitoring for detection of arrhythmias and episodic hypertension, hormonal assay (24 hour urine VMA) to look for active tumour secretion and duplex screen of pelvic and lower limb veins to rule out DVT. We deduced that the patient would benefit from a central neuraxial block, as opposed to general anaesthesia; the surgical plan was changed to vaginal hysterectomy as opposed to laparoscopy assisted vaginal hysterectomy, in consultation with surgeon. It was also concurred upon to avoid adrenaline infiltration of vagina, as this is known to precipitate dysrhythmias.
Inside the operating room, standard ASA recommended monitors (pulse oximeter, non-invasive blood pressure and a 5- lead electrocardiogram) were attached. A bolus of crystalloid (Ringer’s lactate) of 10 ml/kg was initiated. Under sterile aseptic precautions, radial arterial cannulation was performed and transduced for continuous invasive blood pressure monitoring. The patient was positioned with a 10 degree reverse Trendelenburg position prior to the administration of central neuraxial blockade. Under sterile aseptic precautions, 14 mg of bupivacaine with 60 mcg of buprenorphine was administered intrathecally. A sensory blockade of up to T6 dermatome was achieved. A glucose random blood sugar (GRBS) assessment was done intra- operatively and was noted to be 165 mg/dl. Blood loss was estimated to be around 500 ml. A total of 3.5 litres of fluids was administered intra-operatively.
The patient remained hemodynamically stable throughout the procedure. Postoperatively, we encouraged the patient to ambulate as soon as possible. Postoperative analgesia was provided with 12th hourly intravenous paracetamol 1 g and nalbuphine 6 mg. The arterial cannula was removed 12 hours post-operatively since the patient was hemodynamically stable. She was discharged on the 4th postoperative day. On discharge, consultation with a geneticist was advised to confirm the diagnosis of VHL.

Discussion
Von Hippel Lindau syndrome is a genetically predisposed disease, with a multitude of systemic manifestations. A study done on 271 patients with pheochromocytomas showed a germline VHL association in 11% of the patients [2]. Pheochromocytoma refers to catecholamine-secreting tumours that arise from chromaffin cells of the adrenal medulla. The classic triad of symptoms in patients with pheochromocytoma comprises episodic headaches, bouts of perspiration and tachycardia [3].
A 24-hour urine VMA analysis is mandated pre- operatively, to differentiate quiescent tumours from actively secreting pheochromocytomas. Since these tumours can have sporadic and episodic secretion of catecholamines, Holter monitoring is a better predictor of the cardiovascular fitness of the patient as opposed to a standard cross-sectional 12-lead electrocardiogram. Pancreatic abnormalities can also be anticipated in patients with VHL syndrome. Studies suggest that 70% of patients with VHL syndrome have co- existing pancreatic tumours which range from simple cysts to neuroendocrine neoplasms [4].
Hemangioblastomas are the most common lesions associated with VHL and typically involve the central nervous system, causing compression symptoms such as pain and paraesthesia [1]. Thus, a thorough central nervous system examination is warranted before the administration of central neuraxial blocks.
In our patient, the presence of pheochromocytoma was confirmed on an MIBG scan. Though she had hypertension at the time of diagnosis, she was well managed on multiple antihypertensive agents over the past 5 years. Hormonal assay was essentially normal which confirmed that the tumour was not an actively secreting lesion. Holter monitoring was further done to rule out arrhythmias. Though the patient had multiple renal and hepatic cysts, she had no features of hepatic/renal dysfunction. Owing to the multi-morbidities, central neuraxial block was deemed appropriate as opposed to general anaesthesia. In concert with the surgeons, it was decided to change the surgical plan to vaginal hysterectomy and avoid adrenaline infiltration at the surgical site, a commonly employed technique to reduce blood loss, as this is known to precipitate arrhythmias [5].
We placed an intra-arterial catheter for continuous blood pressure monitoring before administration of the subarachnoid block and co-loaded the patient with fluids during administration of subarachnoid block to avoid any drastic hypotension [6]. The patient remained hemodynamically stable throughout the procedure, which could be attributed to extensive pre-operative work-up, a multi-disciplinary approach towards pre-operative optimization and synergistic management with surgical team.
Conclusion
Providing anaesthesia to patients with multisystem involvement such as Von Hippel Lindau syndrome can be very challenging. Meticulous pre-anaesthetic evaluation and pre- operative optimization are often crucial. A multidisciplinary approach is often employed to achieve the best possible pre-operative functional status of these patients. Well- coordinated team with flexibility in interdisciplinary management tailored to the patient helps achieve the best possible outcomes.
- Conflict of Interest: No potential conflict of interest relevant to this article was reported
- Funding: Not applicable
- Acknowledgment: Not applicable
- Disclaimer: Informed consent was obtained from the patient prior to publication
References
-
Maher ER, Yates JR, Harries R, C Benjamin, R Harris, et al. (1990) Clinical features and natural history of von Hippel-Lindau disease. Q J Med 77(283): 1151-1163.
-
Neumann HP, Bausch B, McWhinney SR, Bernhard UB, Oliver G, et al. (2002) Germ-line mutations in nonsyndromic pheochromocytoma. N Engl J Med 346(19): 1459-1466.
-
Stein PP, Black HR (1991) A Simplified Diagnostic Approach to Pheochromocytoma A Review of the Literature and Report of One Institution’s Experience. J Med 70(1): 46-66.
-
Hammel PR, Vilgrain V, Terris B, Penfornis A, Sauvanet A, et al. (2000) Pancreatic involvement in von Hippel– Lindau disease. Gastroenterology 119(4): 1087-1095.
-
Schroeder HG, Evans JM (1969) Adrenaline Infiltration In Vaginal Surgery: A Statistical Analysis of the Effect on Operative Blood Loss during Methoxyflurane Anaesthesia. Br J Anaesth 41(7): 609-614.
-
Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R (1992) Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology 76(6): 906-916.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index