Enhanced Recovery after Cesarean Section (ERAC): Time to Consider
Cesarean section is one of the main operative procedures worldwide. Enhanced recovery after cesarean (ERAC) provides an evidenced-based system to reduce the risk of infection and improve maternal outcomes, functional recovery, maternal-infant bonding, and patient experience by decreasing pain and nausea. ERAC involves the multidisciplinary team efforts of the anesthesiologist, obstetrician, nursing, hospital staff, and patient. This study is an over view of the perioperative components of ERAC protocol and highlights the benefit of implementing them in our clinical practice.
Abbreviations
ASA: American Society of Anesthesiologists; CS: Caesarean Section; ERAC: Enhanced Recovery Caesarean Section; PONV: Postoperative Nausea and Vomiting.
Introduction
Enhanced recovery after cesarean (ERAC) is an evidence based approach aimed at decreasing infection risk and post- operative complications, speed up recovery, shorten stay in hospital, improve maternal infant closeness and patient satisfaction by reducing pain and nauseas after surgery [1]. The primary goal of an ERAC pathway is to reduce the response to surgical stress with regards to patient care. ERAC involves the multidisciplinary team efforts of the anesthesiologist, obstetrician, nursing, hospital staff, and the patient during perioperative period [1].
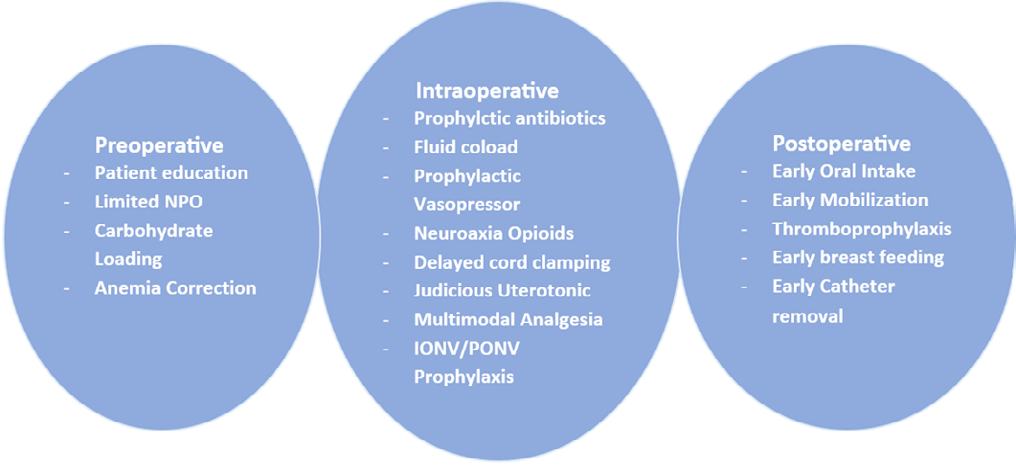
This protocol commences with education in the obstetric physician’s office prior to delivery and ends at the time of hospital discharge. The preoperative components of ERAC include the preoperative components of ERAC include limited fasting, carbohydrate supplementation, and prophylactic antibiotics/skin preparation [1].
Pre-Operative Components
Preoperative Counselling and Education
Patient education/counselling before the day of surgery administered by the obstetrician/ anaesthesiologist/nursing staff is crucial in order gain the patient’s cooperation, set realistic expectations for the patient and the healthcare team as well as increasing patient compliance with ERAC guidelines. It is expected to be made available in the form of videos and leaflets. One published study from the UK in 2015 showed that even just providing written information to patients on the benefits of early discharge increased acceptance of early discharge and the rate of earlier discharges prior to introduction of any other elements of the ERAC components [2]. One form of patient involvement and shared decision making can occur preoperatively and increase patient satisfaction and decrease opioid use [1, 3].
Limited Fasting and Oral Carbohydrate Loading
The American Society of Anaesthesiologists (ASA) guidelines recommend surgical fasting (NPO) of 8h for fatty food, 6hr for light meal, and 2 h for clear liquid before the induction of anaesthesia to reduce aspiration risk.4 Extended NPO periods are generally not warranted and can result in hypovolemia and patients’ dissatisfaction [1, 4]. Recent studies evaluating the effectiveness of enhanced recovery in patients who underwent colorectal surgery revealed that the preoperative consumption of a complex carbohydrate load in the form of maltodextrin dissolved in a non-particulate drink 2-3 h before surgery and in the evening before the operation reduces the metabolic stress response, including insulin resistance postoperatively and the rate of protein loss [5]. This may be omitted for diabetic mothers due to possible slow gastric emptying and high blood sugar levels [5].
Anaemia Correction
Iron in oral or IV form with vitamins is given to correct the iron deficiency anemia in the preoperative period. This will be useful in preventing or minimizing the wound infection and in the meantime promoting the recovery of the patient.
Intraoperative Components
Antibiotics Prophylaxis
As a preventative measure against surgical site infections, broad spectrum antibiotics are given 30 to 60 minutes before skin incision [1, 6].
Prevent or Treat Spinal Induced Hypotension
Hypotension can be prevented or treated by the use of Vasopressor, either bolus or infusion or through fluid coloading. The initial manifestation of spinal induced hypotension is vomiting and nausea. In order to maintain blood volume, maternal blood pressure is attempted to be kept at 90% of their baseline prior to the delivery of the baby and at around 80% post-delivery of the baby. Thus, it can be said that when the above target is maintained, the rate of nausea and vomiting is extremely low. The practices of prophylactic use of infusion or bolus of ephedrine, noradrenaline or phenylephrine effectively avoids hypotension induced nausea following spinal anaesthesia [7, 8].
Multimodal Analgesia
Elevated pain scores after birth has been linked to lower levels of breast feeding and increased rates of post- partum depression and chronic pain.6 Multimodal analgesia is defined as a basic standard for all enhanced recovery techniques that involve medications and intervention apart from general surgical anaesthesia. When the patient requires two or more drugs for achieving the goal of analgesia then, it is known as multimodal analgesia [6, 9]. Examples of such medications are the local anaesthetic agent, NSAIDs, paracetamol, opioids, and steroid. A lipophilic fast-onset short acting opioid, fentanyl or sufentanil are added for intraoperative effects while morphine, a hydrophilic opioid with longer duration is added for postoperative pain. The recommended dose of intrathecal neuraxial morphine for caesarean section is 50–150 mcg, to reduce opioid related adverse effects [1, 10, 11]. Details of any medication given for pain relief including the route of administration will be documented.
Prevention of Maternal Hypothermia
The regulation of body temperature so as to maintain euthermia is challenging. Hypothermia results in shivering and the issue will be to deal with the patient. The use of warmer is difficult to continue. The remedies that could be used are warming of the patients by pre-warming, heating the room and the use of warm intravenous fluids.
Delayed Umbilical Cord Clamping
Delay cord clamping is when the umbilical cord is clamped after 30-60 seconds. There’s evidence however to support delayed clamping in both preterm and term infants, with at least one minute of clamping for a term birth, and at least 30 seconds for a preterm one [1, 12]. Delayed cord clamping was associated with decrease rate of anemia within six months after childbirth [12].
Judicious Uterotonic Agent
There is various recommendation of uterotonic agent to ensure that the delivery process is effective and smooth. Optimal use of uterotonic agents refers to use of IV oxytocin as a bolus of 3 IU immediately after delivery followed by total minimum of 4 hours of infusion time. Further, a prophylactic low-dose oxytocin infusion of 15–18 U/hour should be initiated in the immediate postoperative period to prevent postpartum haemorrhage [13].
Intra and Postoperative Nausea and Vomiting Prophylaxis
An important goal of ERAS is early oral intake, which can be delayed by postoperative nausea and vomiting (PONV). It is recommended to use two different classes of prophylactic antiemetics which includes metoclopramide as D2 receptor antagonist, dexamethasone, and/or ondansetron as 5HT3 antagonist [1, 9].
Skin to Skin Contact
Skin-to-skin contact facilitates mother-child bonding [1, 6]. Early skin-to-skin contact has reduced maternal anxiety and lengthened the breastfeeding period between a mother and her child [13, 14].
Post-Operative Components
Early Oral Intake
Early oral intake is defined as consuming ice chips, water, or gum within 60 minutes of a cesarean section and returning to a regular diet as soon as tolerated within 4 hours. Early oral intake reduces the duration of vomiting, nausea, and infection while also speeding up the return of bowel function, improving mother satisfaction, and accelerating the time to ambulation and discharge. Finally, a Cochrane review discovered, albeit with low grade evidence, that chewing gum in the PACU sped up the return of bowel function and shortened length of stay [15].
Early Mobilization
After surgery, ambulation begins with eight hours of sitting on the edge, moving out from bed to a chair, and walking around. It is advised to walk once or twice in the next eight to twenty-four hours, or as tolerated. The aforementioned are regarded as early mobilization. Theoretically, early mobilization can enhance a number of immediate postoperative outcomes, such as a speedy recovery of bowel function, a lower risk of thrombosis, and a shorter hospital stay [16].
Early Urinary Catheter Removal
Early urinary catheter removal is defined as removing a catheter 6–12 hours following cesarean delivery. It is generally established procedure to insert a urinary catheter during cesarean section. Bladder drainage is often thought to have three benefits: it can evaluate urine production, lessen urinary system injuries, and reduce postoperative urinary retention.16 Nonetheless, one of the most frequent side effects following cesarean delivery is urinary tract infection. Urinary tract infections, urethral discomfort, and difficulty voiding can all be more common in people with indwelling urinary catheters. Delayed mobilization, longer hospital stays, and higher expenses are the outcomes of these problems [17, 18, 19, 20].
Thromboprophylaxis
Non pharmacological methods of thromboprophylaxis like pneumatic compression devices are recommended for all women undergoing caesarean sections. Pharmacological thromboprophylaxis is advised for women who have one or more additional risk factors.
Early Breast Feeding
It is recommended to begin breastfeeding as soon as possible after delivery; this is known as the “golden hour.” The nursing staff’s role should be to educate and support breastfeeding following birth. This will provide benefit to both mother and the baby (Figure 1).
Importance of ERAC protocol
There are multiple benefit of implementation of different components of ERAC protocol to the patient and hospitals. For patients, these benefits include better comfort, reduced anxiety, minimal wound infection, less perioperative pain, early mobilization and better recovery profile and improve bonding between mother and baby. For hospitals, the benefit include better patients outcome and improved turnover ratio, ultimately reducing overall costs [1, 2, 4] ERAC can be implemented for both scheduled and unscheduled cesarean deliveries. The rate of cesarean delivery is increasing worldwide, due to which the implementation of ERAC protocol in maternity care is urgently needed [6].
Therefore, it is crucial for obstetrician, anaesthesiologists, nursing and hospital administrative staff to work together for implementing the ERAC protocol as soon as possible for the benefit of the patients and hospitals [21, 22].
Conclusion
Enhanced recovery after cesarean (ERAC) is a protocolized approach that begins in the preoperative period and continues through the intraoperative and postoperative phases for patients undergoing cesarean section. The protocol includes steps to enhance maternal-infant bonding, accelerate recovery, and reduce postoperative complications such as infection, pain and postoperative nausea and vomiting (PONV). It includes limited fasting, antibiotic prophylaxis, multimodal analgesia and PONV prophylaxis. It
also emphasizes early mobilization and resumption of oral feeding. These measures improve overall patient satisfaction and shorten hospital stay and reduce the health care cost for both the hospital and the patient. It is high time we should implement this approach at our centre.
References
-
Bollag L, Lim G, Sultan P, Habib AS, Landau R, et al. (2021) Society for Obstetric Anesthesia and Perinatology: Consensus Statement and Recommendations for Enhanced Recovery After Cesarean. Anesth Analg 132(5): 1362-1377.
-
Wrench IJ, Allison A, Galimberti A, Radley S, Wilson MJ (2015) Introduction of enhanced recovery for elective caesarean section enabling next day discharge: a tertiary centre experience. Int J Obstet Anesth 24(2): 124-130.
-
Prabhu M, Hanson E, Hopp S, Burns SM, Leffert LR, et al. (2017) A shared decision-making intervention to guide opioid prescribing after cesarean delivery. Obstet Gynecol 130(1): 42-46.
-
(2017) Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Task Force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology 126(3): 376-393.
-
Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, et al. (2019) Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations: 2018. World J Surg 43(3): 659-695.
-
Patel K, Zakowski M (2021) Enhanced Recovery after Cesarean: Current and Emerging Trends. Curr Anesthesiol Rep 11(2): 136-144.
-
Ngan WD, Lee SW, Ng FF, Tan PE, Khaw KS (2015) Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology 122(4): 736-745.
-
Onwochei DN, Ngan Kee WD, Fung L, Downey K, Ye XY, et al. (2017) Norepinephrine Intermittent Intravenous Boluses to Prevent Hypotension during Spinal Anesthesia for Cesarean Delivery: A Sequential Allocation Dose- Finding Study. Anesth Analg 125(1): 212-218.
-
Wu JI, Lo Y, Chia YY, Fong WP, Liu K, et al. (2007) Prevention of postoperative nausea and vomiting after intrathecal morphine for Cesarean section: a randomized comparison of dexamethasone, droperidol, and a combination. Int J Obstet Anesth 16(2): 122-127.
-
Dahl JB, Jeppesen IS, Jorgensen H, Wetterslev J, Moiniche S (1999) Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology 91(6): 1919-1927.
-
Sultan P, Halpern SH, Pushpanathan E, Patel S, Carvalho B (2016) The Effect of Intrathecal Morphine Dose on Outcomes After Elective Cesarean Delivery: A Meta- Analysis. Anesth Analg 123(1): 154-164.
-
McDonald SJ, Middleton P, Dowswell T, Morris PS (2014) Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Evid Based Child Health 9(2): 303-397.
-
Bigelow A, Power M, MacLellan J, Alex M, McDonald C (2012) Effect of mother/infant skin-to-skin contact on postpartum depressive symptoms and maternal physiological stress. J Obstet Gynecol Neonatal Nurs 41(3): 369-382.
-
Moore ER, Anderson GC, Bergman N, Medley N (2016) Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev 11(11): CD003519.
-
Morais E, Riera R, Porfirio GJ, Macedo CR, Sarmento V, et al. (2016) Chewing gum for enhancing early recovery of bowel function after caesarean section. Cochrane Database Syst Rev 10(10): CD011562.
-
Barnes JS (1998) Is it better to avoid urethral catheterization at hysterectomy and cesarean section? Aust NZ J Obstet Gynaecol 38(3): 315-316.
-
Bartzen PJ, Hafferty FW (1987) Pelvic laparotomy without an indwelling catheter. A retrospective review of 949 cases. Am J Obstet Gynecol 156: 1426-1432.
-
Schwartz MA, Wang CC, Eckert LO, Critchlow CW (1999) Risk factors for urinary tract infection in the postpartum period. Am J Obstet Gynecol 181: 547-553.
-
Leigh DA, Emmanuel FX, Segdwick J, Dean R (1989) Post- operative urinary tract infection and wound infection in women undergoing cesarean section: a comparison of two study periods in 1985 and 1987. J Hosp Infect 13: 349-354.
-
Aleem H. Aboelnasr MF, Jayousi TM, Habib FA (2014) Indwelling bladder catheterisation as part of intraoperative and postoperative care for caesarean section. Cochrane Database Syst Rev 4: CD010322.
-
Butwick AJ, Coleman L, Cohen SE, Riley ET, Carvalho B (2010) Minimum effective bolus dose of oxytocin during elective Caesarean delivery. British journal of anaesthesia 104(3): 338-343.
-
George R, McKeen D, Chaplin A, McLeod L (2010) Up- down determination of the ED90 of oxytocin infusions for the prevention of postpartum uterine atony in parturients undergoing Cesarean delivery. Canadian journal of anaesthesia 57: 578-582.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index