Transformation of Agricultural Practices and Health Outcomes: An Empirical Investigation of Chronic Kidney Disease of unknown Etiology (CKDu) in Sri Lanka
The prevalence of chronic kidney disease of unknown etiology (CKDu) has significantly affected rural families, while creating many socio-economic problems in Sri Lanka. Extreme weather due to climatic change has produced many outcomes in dry zone in the country where more prevalence as well as incidents of CKDu are found. In this context, this study attempts to identify the farmers knowledge and attitudes towards the climate change induced transformation of agricultural practices and then estimate the value of loss in earnings due to being a CKDu patient using the Value of Statistical Life (VSL) approach. The study uses a combination of primary data and secondary data. Results show that farmers’ knowledge and awareness of the impacts of climate change on agricultural practices is satisfactorily high while their contribution to mitigate the impacts of it is not significant. The results of the VSL show that the estimated values of statistical life for the entire sample are approximately Rs. 2.50 million and Rs. 4.33 million under 60 and 70 years of retirement ages respectively. The estimated values of the loss earnings under 60 years of retirement age for 11 districts were Rs. 70.30 billion. The result further reveals that the prevailing situation of the CKDu in these districts has seriously affected the health and well-being of their family members, stress level, consumption as well as education of the kids of the affected families.
Introduction
Sri Lanka is already facing the adverse impacts of climate change in the form of droughts, unprecedented and rising temperature, floods, unseasonal rain, and coastal erosion. As a small island nation, Sri Lanka falls into the united nation framework of climate change under category of ‘vulnerable’ small island nations which are under serious threat from various climate change impacts, such as sea level rise, severe floods and droughts [1]. These threats are considered to have significant negative consequences on various sectors within Sri Lanka. Climate change puts extra burdens on the social and economic challenges that the poorest already face, emphasizing and increasing their vulnerabilities due to the dependence of their livelihoods on climate sensitive natural resources, livelihood and the weak social protection structures [2].
CKDu has now become one of the major health crises in Sri Lanka [3]. There has been an abnormal increase in the number of chronic kidney disease patients in the dry zone. According to the World Health Organization, it has been declared that 15% of the population aged 15-70 years, in the North Central and Uva Provinces are affected with CKDu [4]. Recent studies show that CKDu is now also prevalent in the North Western, Eastern, Southern, and Central Provinces. According to the Faculty of Agriculture and Plantation Management, Wayamba University, farming has been found to be strongly correlated with the prevalence of CDKu and those likely to be affected are young males, from low socio- economic, paddy farming communities. However, women and children too are suffering from CDKu. While over 1,100 CKDu patients are hospitalized every month in Sri Lanka, 300 annual deaths are recorded [5]. These Figures show an increasing trend in mortality and morbidity resulting from chronic kidney disease [6].
Studies suggest that high fluoride contents (presence of toxins produced by cyanobacteria in surface waters, particularly in freshwater reservoirs) include high concentrations of Cadmium and might be potential causes for CKDu [7]. Some studies have hypothesized that excessive use of agrochemicals, consumption of certain food such as lotus roots, smoking tobacco, excessive dehydration in the work environment of farmers and genetic predisposition as factors that contribute to the prevalence of Chronic Kidney Disease. Chronic arsenic exposure from drinking water obtained from tube wells has been reported as a cause for CKDu in regions of Bangladesh, Taiwan, and India. Exposure to Cadmium through food and to nephrotoxic pesticides may be considered to be underlying causes [8]. The etiology of CKDu is currently being investigated by several research groups that comprise scientists, biologists, geologists, chemists and medical experts. There have been numerous and continuous research studies that focus on explaining the causative agent or agents of CKDu. Evidence of some research in this area shows that environmental factors as the probable cause for the disease. Since reliable etiology has not been established, the Government of Sri Lanka has requested technical assistance from WHO headquarters in Geneva, to help diagnose the exact cause of the disease. The root cause of the disease although unknown is now under investigation.
Chronic kidney disease cannot be attributed to any known etiology and Sri Lanka is not alone in this mystery. In the past decade, countries such as El Salvador, Nicaragua, Egypt and India also have been affected [9]. While the underlying causes for Chronic Kidney Disease are unidentified, it is believed to be an environmentally induced disease. CKDu has affected people in 11 districts in Sri Lanka [10]. There is a significant increase in the number of patients reported from the Uva province, particularly in the Mahiyangana and Girandurukote districts. Therefore, regions with high densities of CKDu include North Central, Uva, North Western and Central provinces. The affected provinces are also heavily agriculture-based regions and therefore suggest a relationship between agricultural irrigation, water resources and CKDu [11]. Climate change, improper agricultural practices, disappearing the natural vegetation cover and deforestation coupled with soil degradation have led to the increase of water pollution in the dry zone of the country. While some of the geographical mapping studies indicate a relationship between CKDu and agricultural irrigation and water sources; health mapping and human biological studies have focused on likely causative factors related to agricultural practices in those areas. While some recent studies, in this area, show that the incidence of CKDu in Sri Lanka is doubling every four to five years, other studies show the estimates of more than 150,000 affected people of CKDu in the country.
Although a number of studies in the literature discussed various aspects of CKDu including multiple causative factors [12, 13], impacts on household’s livelihood [14], impacts of children’s education and risk factors [4], none of the studies uses VSL methodology to estimate the social burden of it. At the same time there are number of studies that use VSL focusing the valuation of mortality risk of job exposure in labor markets [15], evaluation of the costs of environmental health and safety risks [16] or estimating the trade-offs between money and fatality risks [17], none of the studies uses VSL to estimate the value of loss income of the affected families of CKDu in the literature. However, the use of VSL on the value of mortality in government policy evaluation in the area of CKDu has been a key benefit component of policy evaluations for a wide range of health, safety, and environmental policies. In the literature, the quality adjusted life years (QALY) approach has been used to estimates value of a life year saved (LY) in health sector using aggregate level data. The value of a life year takes on special significance in medicine because a life may be saved, but the person whose life is saved may have far less than a normal quality of life [18]. This has led to estimate the QALY which is a measure of disease burden in a country, including both the quality and the quantity of life lived.
Given this background, this study is attempting to identify the farmer’s knowledge and attitudes towards the climate change induced transformation of agricultural practices and then estimate the income loss of the CKDu patients using the value of the statistical life approach in Sri Lanka. In addition to that, the study will investigate the impacts of CKDu on the livelihood of the affected families. The study uses data gathered from a survey covering selected areas in Anuradhapura, Polonnaruwa and Kurunegala districts. In general, the findings of this research will draw much- needed attention to this issue (which has hidden costs), while achieving livelihood development in the affected areas of Sri Lanka. The remainder of the paper is set out as follows. Section 2 reviews the literature while Section 3 presents a theoretical model of estimating the value of statistical life and discusses the survey and data collection methods. Section 4 presents the results of the analyses of the survey data. In this section, we also report the results of the VSL analyses which examine the discounted flow of the loss of earnings due to CKDu. The final section summarizes and concludes.
Literature Review
Leiserowitz A, et al. [19] argue that about 40% of adults worldwide have never heard of climate change. This rises to more than 65% in some developing countries like Egypt, Bangladesh and India. Mcsweeney [19] states that adults in developed countries were more likely to say they are aware of climate change. Awareness rates in much of North America and Europe were over 90% of respondents. Japan comes top with 99% of the population aware of climate change, with the US 98% and Finland 98%. In contrast, awareness rates in developing countries were much lower, such as 47% of respondents in Philippines said they were aware of climate change, while this was 35% in India and 25% for Egypt. The lowest levels of awareness were recorded for Liberia at just 21%.
CKDu is reported in certain parts of the north central dry zone of Sri Lanka and is also found in Bangladesh, India, Nicaragua and El Salvador [7, 12, 14, 20]. Numerous studies [9, 16, 21, 22, 23, 24] have been conducted by a range of institutions and researchers concerning the problem and as a result, a body of research has been established well in this area. Anawar HM, et al. [25] investigate the sources of Arsenic mobilization in the groundwater in Bangladesh with the simultaneous mobilization of Arsenic and Ferrous sediments by the enhanced activities of indigenous bacteria. Bandara JMRS, et al. [7] identify the concentration of 9 heavy metals found in sediments of soil in five major reservoirs that supply irrigation to the north central province (NCP) in Sri Lanka. All of which carried high levels of cadmium, iron and lead.
They also observed high natural levels of fluoride in the groundwater (drinking water) in NCP and the neglecting of routine desalting of reservoirs for the past 20 years has resulted in the chronic consumption of heavy metals through food chains. Bandara JMRS, et al. [12] find an association between chronic cadmium consumption with Chronic Kidney failure. Chandrajith R, et al. [20] discuss fluoride with the effect of Calcium and Sodium ions as the third cause for renal tubular damage besides hypertension and diabetes.
Athuraliya NTC, et al. [14] observes the prevalence of proteinuric CKDu in northern, central and southern provinces of Sri Lanka and CKDu being endemic to north central province. CKDu not attributed to hypertension, diabetes and other known etiologies is studied by Jayatilake N, et al. [10] focusing on the north central province. Jayasekara JM, et al. [26] study the geographical distribution of CKDu using Geographic Information System (GIS) and Global Positioning System (GPS) mapping for community-based information collected from 11,630 patients. Chronic exposure to high levels of Cadmium through food chains and pesticides, and Cadmium, Selenium and genetic susceptibility being risk factors for CKDu are provided through this research. Dharma- wardana MWC, et al. [11] suggest exposure to high ionicity in water as a risk factor for CKDu. The study shows increased ionicity in drinking water due to, fertilizer sediments in the river systems and in the redox processes of soil in tanks and aquifers. Ramírez-Rubio O, et al. [27] study the possibility of kidney damage prior to occupational exposure after measuring biomarkers of kidney injuries among adolescents of Nicaragua. Gamage CD, et al. [9] found that fungal and bacterial nephrotoxins are possible factors for CKDu etiology. Particularly, infections such as Leptospirosis and Hantavirus, which are known to cause acute renal damage, are investigated in this study.
Sirisena D, et al. [4] discuss how high concentrations of heavy metals in phosphate fertilizer ultimately infiltrate the food chain. Heavy doses of organic and inorganic phosphate used in vegetable cultivation, to maximize productivity, surpass the relatively lower recommended dosage by the government. Therefore, the study emphasizes the government to have restrictions on the use of phosphate fertilizer as modes of tackling the issue of CKDu. Premarathne M, et al. [28] studies the relationship between CKDu and hardness in water in Bandagiriya. A social survey was conducted to determine families’ drinking water sources and, Phytoremediation is proposed as an economically greener method of removing the excess hardness in water. Senanayake SJ, et al. [13] discusses physical and psychological suffering, social suffering, the suffering of the family, economic suffering, hospital admissions costs, household costs of dialysis patients and perceptions regarding kidney transplant within the CKDu affected community in Sri
Lanka. Cooray T, et al. [8] investigate the water quality of groundwater and its suitability for drinking purposes in the dry zone of Sri Lanka. The study introduces the Water Quality Index (WQI) and reveals that only 3.8% in the wet season and 2.6% in the dry season are categorized as excellent WQI.
Although there is no application of VSL to analyses the health outcomes, there are a few applications of the quality-adjusted life-year (QALY) to measure the value of aggregate level health outcomes in the literature. Since health is a function of length of life and quality of life, the QALY was attempting to combine the value of these attributes into a single index number [29]. A few studies attempted to estimate the QALY which is a generic measure of disease burden in a country, including both the quality and the quantity of life lived. For example, Kerridge RK, et al. [30] examines the feasibility of using QALYs to assess patient outcome and the economic justification of treatment in an Intensive Care Unit in Australia. Zhang P, et al. [31] applied to method to analyses the economics of diabetes management with the efficient use of limited healthcare resources. Touray MML, et al. [32] investigated the impact of ‘time-effect’ on the estimation QALYs and found that it can have significant implications for resources allocations decisions. Moradi N, et al. [17] investigates the worth of QALYs from the perspectives of patients with diabetes using health and willingness-to-pay (WTP) measures.
Reviews of previous literature clearly show divergence of opinion as mentioned above. While some studies have shown that many socioeconomic factors have some impacts on CKDu, some other studies do not provide strong evidence related to those variables. Moreover, existing studies do not estimate the magnitudes of the incurred economic loss as a result of being a CKDu patient using the VSL approach. Therefore, there is still a debate about the level of the impact of CKDu on the household economy in rural areas of the country. Given this context, this study investigates the impacts of CKDu on the household economy by estimating the value of loss in earnings. We used the VSL approach which is a novel approach to this area. The information provided in this study will be helpful for policymakers to be aware of the magnitude of the economic loss due to chronic kidney disease in Sri Lanka. In addition to that, the government will be able to identify the true economic burden that is confronted by kidney patients or their families for making appropriate policies in the future.
**Theory and Methodology**
The value of statistical life is generally estimated using the human capital (HC) approach, which has a long history dating back to the works of the 1950s. However, later studies have significantly improved the theoretical and practical underpinnings of the approach. In the standard HC approach, it is assumed that the value to society by an individual’s life is measured by future production potential, usually calculated as the present discounted value of expected labour earnings [33, 34]. However, some studies in this area have used expected net earnings, which consider the future consumption flow as well. Accordingly, similar to physical capital, the net loss to society can be taken as the difference between earnings, and maintenance (consumption) expenditures. Whether the gross HC approach or the net HC approach (after adjusting for consumption) is employed, each is implicitly based on the maximization of society’s present and future production process or earnings by undertaking a productive economic activity [31, 35].
The lifetime income-based approach which is used in this study to measure human capital by summing the discounted values of all future income streams that an individual is expected to earn throughout his/her lifetime [36]. It measures the value of the total stock of human capital embodied in individuals as the sum of the discounted present value of all future income streams. A few applications of lifetime income-based approach can be seen in the field of road accidents [37], occupation or environment related risk [15] and health issues [38].
In general, the cost-based approach [32] focuses on the input side while the lifetime income-based approach measures the stock of human capital from the output side. The main assumption of the lifetime income-based approach is that labour is paid according to its present income flows [31, 39]. The corresponding equation for a human capital asset involves using earnings as given in Equation 1. The PV of a specific amount received in the future after n-year of time period and i- amount of the discount rate (which is closely related to the real interest rate) is given by the following formula Gunatilake HM, et al. [40]:
$$PV = \frac{Income / earnings}{[1 + i]^n}$$
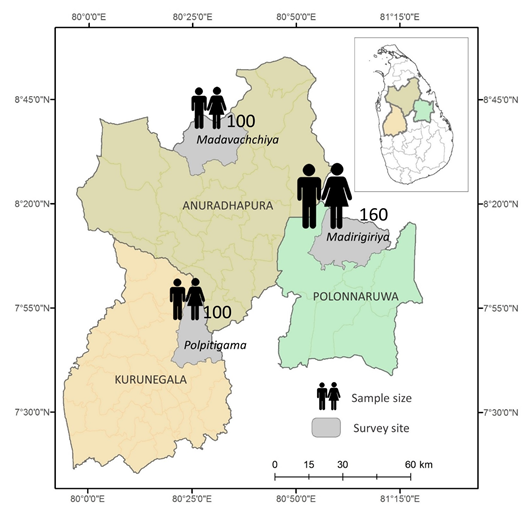
Where PV stands for present value and income/earnings consider the average yearly income of the respective CKDu patient who earned before being the disability. Discount rate is given by i who represents the market interest rate and n goes until the retirement age [40]. For example, if an individual became a CKDu patient by the age of 45, he/she would loss income until 60 years (retirement age) that is similar to the loss of annual income of 15 years. For the each CKDu patient we identified the annual income flow until the retirement age and then estimated the present value for obtaining the total loss earning for the sample due to being a patient. Then sample averages were used to estimate the loss earning for the three districts after combining with secondary data (total number of reported CKDu cases in each district). Then after using three district average loss earnings and total number of cases in 11 districts, each district total loss earning was estimated. This approach estimates an individual’s contribution to society by applying labour force earnings as a measure of productivity or economic contribution. It assumes continuous employment in the same job in the labour market or in one’s own business. In this case, if a person leaves the labour market, he or she will not be replaced and so an opportunity cost exists until the age of retirement. Based on this opportunity cost, the VSL is estimated. For this study, we have selected Anuradhapura, Polonnaruwa and Kurunagala districts purposely. Then while considering the divisional secretariat level data, one DS division was selected from each district based on the highest reported CKDu cases. These selected DS divisions include Madavachchiya, Madirigiriya and Polpitigama. Then the list of CKDu patients of each DS division is taken from the DS office. Approximately 160 CKDu patients from Madavachchiya and 100 from Madirigiriya and Polpitigama were selected from the list randomly for the survey (Figure 1).
Data for this study was collected from a survey conducted covering 360 CKDu patients in all three districts. The study is based on cross-sectional data, collected from 2019 May to August. A structured questionnaire was used to collect relevant information and finally, 342 CKDu patients’ information was used in the analysis. The survey was conducted by 12 well-trained undergraduates. A well- structured and field pretested comprehensive interviewing schedule is used for the collection of detailed information on various aspects of respondents in the area. Data about their socio-economic characteristics, income, and expenditure and health conditions are collected during the survey. The survey also covers information on food habits, economic activities involved, agrochemical usage, family history, changes in income sources and other socio-economic information. The survey was carried out at the household level including individual responses for health status, health expenditure, cultivation practices and education on CKDu illnesses in the area. In addition to that various socio-economic information and other details such as medical expenditure, averting activities, etc. were gathered at the same time. Village officers were discussed for the sake of validation of data acquired at the household and individual level. Data were collected through face-to-face interview of the CKDu patients of the house along with any helping hands. However, around 18 questionnaires had to be dropped out from the analysis as erroneous answers and some outliers were found. The questionnaire used in the survey was validated in a pilot survey and through focus group discussions. The final questionnaire was adjusted following the pilot survey and focus group discussions. The gathering of data was conducted by a trained group of researchers under the close supervision of the research team. The interviews took place in the interviewees’ home. The participants were informed about the purpose of the study and, provided verbal consent to take part in the study. A field supervisor reviewed the quality of the data gathered and entered it into a database for analysis.
Results and Discussion
CKDu has severely affected people in 11 districts in Sri Lanka and data postulate a range of 0.05 % -2.20 % of residents being affected of those districts by 2018. Reports stated by the Ministry of Health show that in the year 2010 the CKDu patients totaled approximately 15,000, by the year 2015 the affected amount increased to 25,000 and a staggering 30,000 affected as of the year 2019 and since the early 2000’s the North Central Province has reported the highest number of CKDu cases. When compared to other districts, Anuradhapura, endemic to CKDu, has the highest mortality from the disease. There is a significant increase in the number of patients reported from the Uva province, particularly in the Mahiyangana and Girandurukote areas in recent years. At present, regions with high densities of CKDu include North Central, Uva, North Western and Central provinces. The affected provinces are also heavily agriculture-based regions; to hypothesize the relationship between agricultural irrigation and water resources and CKDu. The number of reported CKDu patients in selected high-risk districts by the end of 2016 and 2018 are given in Table 1.
| Districts | No. of Patients (2016) | Prevalence (%) (2016) | No. of Patients (2018) | Prevalence (%) (2018) | Change (%) |
|---|---|---|---|---|---|
| Anuradhapura | 9902 | 1.07 | 10,065 | 1.16 | 1.65 |
| Polonnaruwa | 5853 | 1.44 | 7201 | 1.6 | 23.03 |
| Badulla | 1621 | 1.29 | 1691 | 1.17 | 4.32 |
| Kurunegala | 1914 | 0.44 | 1904 | 0.44 | -0.52 |
| Matale | 1611 | 0.97 | 2159 | 1.75 | 34.02 |
| Moneragala | 394 | 0.18 | 1534 | 0.31 | 289.34 |
| Mullaithivu | 492 | 1.5 | 619 | 2.2 | 25.81 |
| Vavuniya | 1542 | 0.88 | 977 | 0.88 | -36.64 |
| Trincomalee | 700 | 0.49 | 702 | 0.49 | 0.29 |
| Ampara | 1057 | 1.2 | 1077 | 1.2 | 1.89 |
| Hambanthota | 183 | 0.05 | 185 | 0.05 | 1.09 |
| Total | 24,806 | 0.76 | 28,114 | 0.88 | 13.34 |
Table 1: Number of reported CKDu patients in selected high-risk districts. Note: The number of reported cases by the end of the y
Characteristics of individuals responding to surveys are explained below. The average age of the respondents is 61 years with a minimum of 34 and a maximum of 88 years. The study found that most of the affected are male which 62% of the total sample is. The majority of the affected are mature in age and approximately 58% of them are in their 50s. Approximately 72% of those affected were the head of the family and there were 4 households of which both parents had been affected.
Male respondents are 62% while females’ respondents are 38%. Most of the respondents were farmers (92%) and 8% employed either private or government sector permanent positions. Approximately 4% of the respondents were engaged in various businesses in the area in addition to the agricultural practices. The mean monthly income of the respondents is Rs. 25,601. Bad habits have a significant influence on the health of people. Our survey data reveals that approximately 89% of respondents were smoking (cigarette, beedy, etc.). However of those, only 54% were addicted to smoking. Around 56% were consuming alcohol everyday while another 34% was taking, at most, 2 days per month. Most respondents have obtained secondary level of education (57%) and 26 per cent of the respondents have completed up to GCE A/ L examination.
| Average | Maximum | Minimum | SD | |
|---|---|---|---|---|
| Age (number of years) | 61 | 88 | 34 | 11.86 |
| Education (number of years) | 7 | 14 | 0 | 3.76 |
| Weight (Kg) | 58 | 82 | 46 | 14.27 |
| Height (CM) | 154 | 192 | 141 | 24.98 |
| Gender (M / %) | 62 | |||
| Main occupation (agriculture / %) | 92 | |||
| Number of years resided in this village | 55 | 88 | 29 | 12.16 |
| Land ownership to family | 0.5 | 3.5 | 0.12 | 1.13 |
| Family size | 4 | 8 | 6 | 1.86 |
| Family income (Rs./ per month) | 25,601 | 64,540 | 8,220 | 17390.5 |
| No. of years spend with diseases (years) | ||||
| Less than 5 (%) | 42 | |||
| Between 5 and 10 (%) | 46 | |||
| More than 10 (%) | 12 | |||
| Total sample | 342 | |||
Table 2: Descriptive statistics. Note: Survey covers 360 respondents, however only 342 questionnaires of the respondents could be
Accordingly, in the Table 2, it is evident that approximately 88% of the CKDu patients suffer from the disease between 1 to 10 years with the disease while 12 % suffer for more than 10 years. During the survey, approximately 86% of respondents mentioned that the life span of the CKDu patients was less than 10 years after contracting the disease. This implies that the majority of CKDu patients survive less than 10 years after contracting the disease. During the survey, we collected information related to the respondents’ opinion about their own behavior before being a CKDu patient.
That information is summarized in Table 3. Accordingly, the number of respondents (out of male) who often consumed alcohol was only 69% of the sample. However, almost all male respondents mentioned that they consumed alcohol but not very often. We also collected information related to smoking which can be among the causative factors for chronic kidney diseases. According to the survey data, almost 88% of the CKDu male patients were smokers and of them, around 38% smoked only occasionally.
| Respondents (%) | |
|---|---|
| Involved regular exercise | 12.16 |
| Involved in sports activities during school | 16.41 |
| Maintained good food habits | 42.94 |
| Suffering from other health issues | 8.87 |
| Suffering from a high level of mental stress | 62.21 |
| Highly chemical usage in agriculture | 54.15 |
| Suffering from regular food shortage | 15.93 |
| Smoking (out of male) | 88.94 |
| Alcohol consumption (out of male) | 69.24 |
| Using domestic medicine for a long time | 6.21 |
Table 3: Respondent’s opinion about their own behavior before being a CKDu. Note: These percentages were calculated based on resp
After investigating the socio-economic background of the respondents, we started the estimation of VSL using each sample in each district, separately. When estimating the VSL, three main variables namely age of giving up the work or employment, retirement age, discount rate and average monthly earnings need to be identified. The average values of these variables for each sample are given in Table 4.
| Districts | Sample Size | Average Age | Average Income (Monthly/ Rs.) | Discount rate (%) |
|---|---|---|---|---|
| Anuradhapura | 152 | 46 | 24,345 | 11 |
| Polonnaruwa | 94 | 44 | 25,431 | 11 |
| Kurunagala | 96 | 49 | 27,028 | 11 |
| Total | 342 |
Table 4: Details of the sample statistics used to estimate PV. Note: Average income was estimated using the last five-year income
When comparing the sample averages among three districts, it becomes clear that there is not a significant difference between the districts. There is no difference in the average lending rates among different districts in the country. Therefore, the discount rate, which is estimated using the average lending rates over the last 10 years, is 11% in the study. The average monthly income was relatively higher in the Kurunegala district, which is approximately Rs. 7000. Data shows that the average age of detecting a CKDu patient varies between 44 and 49. Using this information, we estimated the VSL for each sample after assuming two retirement ages, 60 and 70. The descriptive statistics given in Table 2 shows that the main means of living for most of the patients in the sample is farming. Almost 92 % had been working as farmers and not many were engaged in other activities as their livelihoods. In general, VSL studies use the age of 60 as the retirement age which is valid in the formal sector full employment. When considering agricultural workers in rural areas, most healthy or active people work until 70 or even late in their life. Therefore, we used 60 as well as 70 as the retirement ages in order to estimate VSL for the samples in each district. These estimates are given in Table 5.
| District | VSL (Rs./Per Year) | VSL: Retired 60 (Total Loss/ Rs.) | VSL: Retired 70 (Total Loss/ Rs.) |
|---|---|---|---|
| Anuradhapura | 190,452 | 2,666,328 | 4,570,848 |
| Polonnaruwa | 177,342 | 2,837,472 | 4,610,892 |
| Kurunagala | 181,628 | 1,997,908 | 3,814,188 |
| Total | 549,422 | 7,501,708 | 12,995,928 |
Table 5: Estimated PV of the loss earnings. Note: These estimations were carried out using the sample data It became clear from t
Table 5: Estimated PV of the loss earnings. Note: These estimations were carried out using the sample data It became clear from the survey that the patients of CKDu had been engaged in different types of livelihoods. This has resulted in the variation in their monthly or annual income significantly. In order to avoid the impacts of those temporary variations of income on VSL, we used the last 5 years of average annual income and divided it by 12 to estimate the monthly income for each individual. The second column of Table 5 reports the average VSL per year for each sample. When assuming retirement age as 60 and 70, the estimated VSL or accumulated loss earnings are given in column 3 and 4. The estimated PV of the loss earnings or VSL for the entire sample was Rs. 7.50 million and Rs. 12.99 million under 60 and 70 years of retirement respectively. The analysis further revealed that a 3% deviation (plus or minus) of the interest rate resulted in changing the VSL by 5% to 9%, which indicates that the results are less sensitive to the key interest variable used in this study. Using this information, we next estimated the VSL for 11 high-risk districts in Sri Lanka. These estimations are given in Table 6.
| VSL (Rs. Mn/ Per Year) | Retired 60 (Total Loss/ Rs.Mn) | Retired 70 (Total Loss/ Rs.Mn) | |
|---|---|---|---|
| Anuradhapura | 1843.31 | 25168.23 | 43601.34 |
| Polonnaruwa | 1318.8 | 18006.6 | 31194.56 |
| Badulla | 309.69 | 4228.46 | 7325.37 |
| Kurunegala | 348.7 | 4761.08 | 8248.08 |
| Matale | 395.4 | 5398.73 | 9352.74 |
| Moneragala | 280.94 | 3835.87 | 6645.25 |
| Mullaithivu | 113.36 | 1547.85 | 2681.49 |
| Vavuniya | 178.93 | 2443.06 | 4232.34 |
| Trincomalee | 128.56 | 1755.4 | 3041.05 |
| Ampara | 197.24 | 2693.11 | 4665.54 |
| Hambanthota | 33.88 | 462.61 | 801.42 |
| Total | 5148.82 | 70301.01 | 121789.17 |
Table 6: Estimated PV of the loss earnings or VSL for high-risk districts. Note: Sample average was used to estimate the loss ear
It is evident, from these estimates that most of the CKDu patients are still at working and economically productive ages. As a result, it has a considerable impact on the households’ income as well as the entire economy in those districts. According to the estimates given in Table 6, the total VSL or loss earnings per year as a result of being CKDu patients is Rs. 5.14 billion for all 11 districts in Sri Lanka. The estimated PV of the loss earnings or VSL for all 11 districts were Rs. 70.30 billion and Rs. 121.78 billion under
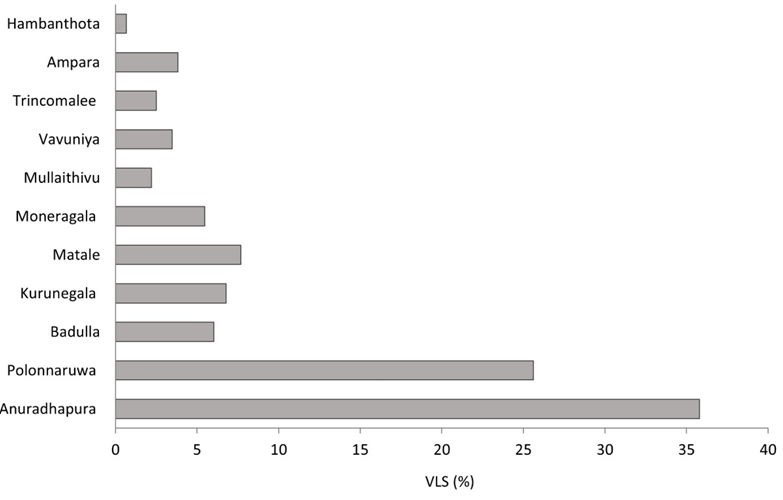
60 and 70 years of retirement respectively. These values could be higher if we incorporate the number of CKDu cases in other districts as well. We also analyzed the survey data qualitatively to understand the various issues that these patients faced in these areas. Accordingly, the majority of the affected households, which is 83% of the total sample claim that their family income, has dropped due to the disease. Further, in some households where there are female patients, the impact of the disease on the households’ income was found to be less because in those family’s males could run the agricultural activities without any interruption. To identify the distribution of loss earnings among the districts, a percentage contribution to the total was identified. Figure 2 gives these percentage values of loss earnings.
The survey data revealed that the majority of the patients (96 %) receive treatment from government hospitals and approximately 12% use treatments from the Private Practice Places (PPP) as well as government hospitals. Further, it was found that approximately 14% use domestic medicine with western medicine. Also, the tendency of opting for domestic treatment differs in the districts. A relatively high percentage of the patients in the Polonnaruwa district were reported to have sought domestic treatment. We also estimated the average private costs of medicines, tests, meeting doctors, transportation…etc for each district using sample data. It was found that the average private monthly costs of medicine for households (except various tests) in the three sample districts are Rs.3, 250, Rs. 2,480 and Rs.3, 320, respectively, for Anuradhapura, Polonnaruwa and Kurunagala districts. The estimated average private monthly costs of other health-related items, including transports, special foods… etc, for households in the three sample districts are Rs.3, 720, Rs. 3,150 and Rs.2, 990 respectively for Anuradhapura, Polonnaruwa and Kurunagala districts. Meanwhile, it was revealed that CKDu patients have to undertake various tests and approximately Rs. 1,080 has to be spent for those.
It is obvious that the average private cost is approximately Rs. 6,630.00 per person per month. The government is giving Rs. 5000.00 for each patient as the monetary subsidy which could help them to cover approximately 75% of their health- related costs. The above costs do not include the direct costs that are borne by the government for medicine including even the charges of laboratory tests done. As such it is observed much of the burden of treatment for CKDu patients is borne by the government. Further, through the analysis of qualitative data, it was found that the disease had forced some of the households to borrow money from the informal sector. Several households had pawned their jewellery rather than borrowing from others to obtain the money they required for the treatment needs. It was also found that the disease has affected the education of children of some affected households (37%). More often at least one or more children had dropped out of school to take up agriculture- related activities in the family. According to the opinion taken from respondents, CKDu has seriously affected the health and wellbeing of their family members (73%), stress level (66%), expenditure pattern (71%) as well as the economic activities of the affected families.
As the last part of the study, we also analyse the knowledge, awareness and attitudes of farmers towards the climate changes, change of the agricultural practices and CKDu issue in the study area. Simple average calculation for the sample to each question is given in Tables 7 & 8. While Table 7 provide the details about farmers’ knowledge and awareness about the climate change, Table 8 helps to understand their attitudes towards climate changes and agricultural practices. In the questionnaire we include a set of questions related to peoples’ attitudes. Before asking these questions, enumerators explain the basic global environmental issues, changes of agricultural practices and use of chemical fertilizer and pesticides intensively for the modern agricultural practices to respondents. Then respondents were allowed to select one of the three options. Simple average calculation for both samples to each question is given in Table 8.
| Yes | |
|---|---|
| Have you heard about the climate change | 84.33 |
| Do you contribute to the climate change | 15.64 |
| Do you think that climate changes have some impacts on your livelihood | 72.87 |
| Do you think that climate changes will have more impacts on our future generation | 74.56 |
| Do you feel the pattern of weather is generally changing in this area | 82.46 |
| Do you think anything can be done to tackle climate change | 54.56 |
| Have you ever taken, or do you regularly take, any action out of concern for climate change? | 12.34 |
| Have you changed your agricultural practices for fitting the climate in this area | 81.46 |
| Do you think that climate change has some impacts on CKDu issue | 54.61 |
Table 7: Knowledge and awareness about the climate change Note: Percentage of others says “No” or don’t know
| Statement | Agree | Disagree | Not sure |
|---|---|---|---|
| I do not believe climate change is a real problem | 36.52 | 42.67 | 20.81 |
| Climate change is something that frightens me | 12.35 | 68.34 | 19.31 |
| The effects of climate change are likely to be catastrophic | 14.34 | 67.52 | 18.14 |
| The evidence for climate change is unreliable | 24.35 | 72.56 | 3.09 |
| I will be unable to contribute to reduce the climate change | 64.32 | 25.41 | 10.27 |
| I will be unable to contribute to protect my environment | 67.05 | 18.62 | 14.33 |
| We all have a huge responsibility to protect our environment | 81.42 | 17.32 | 1.26 |
| Education through media is an important component of education for sustainable development | 63.54 | 27.31 | 9.15 |
| Climate change is inevitable because of the way modern society works | 67.35 | 32.21 | 0.44 |
| Climate change is just a natural fluctuation in earth’s temperatures | 22.34 | 64.52 | 13.14 |
| It is already too late to do anything about climate change | 22.62 | 53.64 | 23.74 |
| Human activities have no significant impact on global temperatures | 5.36 | 86.25 | 8.39 |
| Climate change induced agricultural practices are obvious in this area | 88.94 | 8.23 | 2.83 |
| Climate change induced agricultural practices are the main reasons for various diseases | 58.32 | 28.31 | 13.37 |
| Climate change induced agricultural practices are the main reasons for water pollution | 78.52 | 6.35 | 15.13 |
| Climate change induced agricultural practices are the main reasons for CKDu | 54.23 | 28.23 | 17.54 |
| More chemical fertilizers and pesticides are used now than 20 years ago | 94.56 | 2.35 | 3.09 |
| Developed countries should take most of the blame for climate change | 74.56 | 18.26 | 7.18 |
| The government is not doing enough to tackle climate change | 78.65 | 16.28 | 5.07 |
| Lack of proper policy implementation is the main threat to climate change in Sri Lanka | 75.63 | 12.35 | 12.02 |
Table 8: Attitudes towards the climate change.
According to the results, it is clear that most farmers have heard about the climate changes (84%) and believe that climate changes have some impacts on your livelihood (73%) as well. Furthermore approximately 95% of the respondents believe that more chemical fertilizers and pesticides are used now than 20 years ago while 89% of the respondent mentioned that climate change induced agricultural practices are obvious in this area. Further 78% of the respondents say that climate change induced agricultural practices are the main reasons for water pollution. When inquiring whether climate change has some impacts on CKDu issue approximately 54% of the respondents says “Yes” while 27 % say “No”. However, their awareness as well as attitudes reveals that still those farmers have not given any priority for the issue. It is clear that lack of proper policies, lack of regulations and absence of good governance have resulted in unsustainable agricultural practices in the country. It is commonly accepted that education can be considered to be one powerful tool in making the people aware of the issue and sustainable agricultural practices. Therefore, it is important educating people regarding their individual contribution, social responsibilities of protecting environment as well as the speed of environmental degradation and how they can contribute to enhancing the environment’s present condition.
Conclusion and Policy Recommendations
Extreme weather due to climatic change has produced many unfavorable outcomes in dry zone in the country where more prevalence as well as incidents of CKDu are found. In the literature, a number of different arguments and counterarguments have built up over probable causes of the disease based on different perceptions, attitudes and knowledge of the relevant groups or individuals. The common argument which was presented by using empirical evidence in Sri Lanka was the impact of agrochemicals in causing CKDu. According to those arguments, paddy, freshwater fish and water-based edible plants and roots in the affected areas were reported to contain agrochemicals such as cadmium, and arsenic, which damage the kidneys in the long run. In addition to this, the use of low-grade aluminum cooking utensils and several other unhealthy food habits were also found to be possible reasons for the disease. Even in the medical literature, considerable attention has been given to investigate the relationship between the quality of groundwater and CKDu. Accordingly, the government has taken necessary steps to discourage the use of the majority of the wells and deep wells of the households which had been used as sources of their drinking water because they contained elements that can damage the kidneys as reported in some of the affected areas. Furthermore, as shown in the results even in this study, most of the patients suffering from kidney disease are, relatively, of old age and have been engaged in agriculture for at least 20 to 30 years in their lifetime. Accordingly, it is also apparent that there is a possibility to show a relationship between a person’s involvement in agricultural activities and kidney disease.
In this paper, we have attempted to identify farmer’s knowledge, awareness and attitudes on climate changes induced agricultural practices while estimating monetary values of loss earnings of the CKDu patients using a standard methodology known as VSL approach. The study uses a combination of primary data along with secondary data. Primary data were collected covering 342 CKDu patients from Anuradhapura, Polonnaruwa and Kurunagala districts in 2019. Using the survey data, we estimated the PV of the loss earnings for the entire sample. Under 60 and 70 years of retirement, it was Rs. 7.50 million and Rs. 12.99 million, respectively. The analysis also found that a 3% fluctuation (plus or minus) in the interest rate caused the VSL to change by 5% to 9%, indicating that the results are less sensitive to the key interest variable employed in this study. Approximately 83 % of the overall sample claims that the condition has had a substantial impact on their family’s income. The average monthly private direct expenses of medicine for households in the three samples were Rs. 3,560 (including costs of various medical tests), while the average monthly indirect cost per patient was Rs. 3070. As a result, the average private cost per person per month is around Rs. 6,630, or roughly one-fourth of their monthly family income. It was also discovered that the sickness (CKDu) had a negative impact on the education of some of the children in the affected households (37 %). More frequently than not, at least one or more children had dropped out of school to help with the family’s agricultural pursuits. According to the responses, CKDu has had a significant impact on the health and well-being of their family members (73%), stress levels (66%), spending patterns (71%), and economic activities of the affected households.
Using average estimates derived from the survey data, average values of loss earnings for CKDu patients for 11 districts were estimated. Accordingly, the estimated values of the loss earnings under 60 years of retirement age for 11 districts were Rs. 70.30 billion. This represents the magnitudes of unaccounted economic burden due to the CKDu issues in the country. The result further reveals that the prevailing situation of the CKDu in these districts has seriously affected the health of their family members, stress level, consumption patterns as well as the education of the kids of the affected families. At present government does not consider this loss of income as well as its long-term impact on welfare of those families. Therefore, the government has to take necessary measures to improve the welfare of the affected families which will help them to maintain their children’s s’ education without disrupting their life. Improving health facilities while organizing psychological programs to reduce their stress level is needed to minimize the impacts of CKDu on the lifestyle of the affected families. In addition to this, the results of this study show the important of educating people regarding their individual contribution, social responsibilities of protecting environment as well as the speed of environmental degradation and how they can contribute to enhancing the environment’s in the long term. In this context, this research will help policymakers to understand the magnitudes of the loss due to climate change induced agricultural practices such as CKDu and farmers perceptions as well as knowledge on it.
References
-
(1992) United Nations Framework Convention 62220.
-
(2016) Ministry of Mahaweli Development and Environment Climate Change Secretariat.
-
Ranasinghe H (2017) Organic Agriculture as a Sustainable Solution to Chronic Kidney Disease Unidentified (CKDu). Int J Multidiscip Stud 3(2): 71-77.
-
Sirisena D, Suriyagoda LDB (2018) Toward sustainable phosphorus management in Sri Lankan rice and vegetable-based cropping systems: A review. Agric Nat Resour 52(1): 9-15.
-
Ministry of Heealth (2021) Annual Health Statistics 2019 Sri Lanka. Ecum Rev 1-80.
-
De Silva PMCS, Mohammed Abdul KS, Eakanayake EMDV, Jayasinghe SS, Jayasumana C, et al. (2016) Urinary Biomarkers KIM-1 and NGAL for Detection of Chronic Kidney Disease of Uncertain Etiology (CKDu) among Agricultural Communities in Sri Lanka. PLoS Negl Trop Dis 10(9): e0004979.
-
Bandara JMRS, Senevirathna DMAN, Dasanayake DMRSB, Herath V, Bandara JMRP, et al. (2008) Chronic renal failure among farm families in cascade irrigation systems in Sri Lanka associated with elevated dietary cadmium levels in rice and freshwater fish (Tilapia). Environ Geochem Health 30(5): 465-478.
-
Cooray T, Wei Y, Zhong H, Zheng L, Weragoda SK, et al. (2019) Assessment of groundwater quality in CKDu Affected areas of Sri Lanka: Implications for drinking water treatment. Int J Environ Res Public Health 16(10): 1-16.
-
Gamage CD, Sarathkumara YD (2016) Chronic kidney disease of uncertain etiology in Sri Lanka: Are leptospirosis and Hantaviral infection likely causes. Med Hypotheses 91(1): 16-19.
-
Jayatilake N, Mendis S, Maheepala P, Mehta FR (2013) Chronic kidney disease of uncertain aetiology: Prevalence and causative factors in a developing country. BMC Nephrol 14(1): 180.
-
Dharma-wardana MWC, Amarasiri SL, Dharmawardene N, Panabokke CR (2015) Chronic kidney disease of unknown aetiology and ground-water ionicity: study based on Sri Lanka. Environ Geochem Health 37(2): 221- 231.
-
Bandara JMRS, Wijewardena HVP, Bandara YMAY, Jayasooriya RGPT, Rajapaksha H, et al. (2011) Pollution of River Mahaweli and farmlands under irrigation by cadmium from agricultural inputs leading to a chronic renal failure epidemic among farmers in NCP, Sri Lanka. Environ Geochem Health 33(1): 439-453.
-
Senanayake SJ (2018) Chronic kidney disease in Sri Lanka: a glimpse into lives of the affected. J Coll Community Physicians Sri Lanka 24(2): 56-65.
-
Athuraliya NTC, Abeysekera TDJ, Amerasinghe PH, Kumarasiri R, Bandara P, et al. (2011) Uncertain etiologies of proteinuric-chronic kidney disease in rural Sri Lanka. Kidney Int 80(11): 1212-1221.
-
Hein L, Roberts P, Gonzalez L (2016) Valuing a Statistical Life Year in Relation to Clean Air. J Environ Assess Policy Manag 18(4): 1650025.
-
Peraza S, Wesseling C, Aragon A, Leiva R, García- Trabanino RA, et al. (2012) Decreased kidney function among agricultural workers in El Salvador. Am J Kidney Dis 59(4): 531-540.
-
Moradi N, Rashidian A, Nosratnejad S, Olyaeemanesh A, Zanganeh M, et al. (2019) The Worth of a Quality- Adjusted Life-Year in Patients with Diabetes: An Investigation Study using a Willingness-to-Pay Method. PharmacoEconomics Open 3(3): 311-319.
-
Ashenfelter O (2006) Measuring the Value of a Statistical Life: Problems and Prospects, pp: 19116.
-
Leiserowitz A, Thaker J (2012) Climate change in the Indian mind. Yale Proj Clim Chang Commun 1-228.
-
Chandrajith R, Dissanayake CB, Ariyarathna T, Herath HMJMK, Padmasiri JP, et al. (2011) Dose-dependent Na and Ca in fluoride-rich drinking water -Another major cause of chronic renal failure in tropical arid regions. Sci Total Environ 409(4): 671-675.
-
Nelson RG, Pankratz VS, Ghahate DM, Bobelu J, Faber T, et al. (2018) Home-based kidney care, patient activation, and risk factors for CKD progression in zuni indians a randomized, controlled clinical trial. Clin J Am Soc Nephrol 13(12): 1801-1809.
-
Torres C, Aragon A, González M, López I, Jakobsson K, et al. (2010) Decreased Kidney Function of Unknown Cause in Nicaragua: A Community-Based Survey. Am J Kidney Dis 55(3): 485-496.
-
Weaver VM, Fadrowski JJ, Jaar BG (2015) Global dimensions of chronic kidney disease of unknown etiology (CKDu): A modern era environmental and/or occupational nephropathy?. BMC Nephrol 16: 145.
-
Fraser SD, Blakeman T (2016) Chronic kidney disease: identification and management in primary care. Pragmat Obs Res 7: 21-32.
-
Anawar HM, Akai J, Yoshioka T, Konohira E, Lee JY, et al. (2006) Mobilization of arsenic in groundwater of Bangladesh: Evidence from an incubation study. Environ Geochem Health 28(6): 553-565.
-
Jayasekara JM, Dissanayake DM, Adhikari SB, Bandara P (2013) Geographical distribution of chronic kidney disease of unknown origin in North Central Region of Sri Lanka. Ceylon Med J 58(1): 6-10.
-
Ramírez-Rubio O, Amador JJ, Kaufman JS, Weiner DE, Parikh CR, et al. (2016) Urine biomarkers of kidney injury among adolescents in Nicaragua, a region affected by an epidemic of chronic kidney disease of unknown aetiology. Nephrol Dial Transplant 31(3): 424-432.
-
Premarathne M, Asanthi H, Atapaththu K (2018) Phytoremediation for Excess Water Hardness in Drinking Water: A Causative Factor for CKDu in Bandagiriya, International Forestry and Environment Symposium 23.
-
Prieto L, Sacristán JA (2003) Problems and solutions in calculating quality-adjusted life years (QALYs). Health Qual Life Outcomes 1: 80.
-
Kerridge RK, Glasziou PP, Hillman KM (1995) The use of “Quality-Adjusted Life Years” (QALYs) to evaluate treatment in intensive care. Anaesth Intensive Care 23(3): 322-331.
-
Zhang P, Engelgau MM, Norris SL, Gregg EW, Narayan KM, et al. (2004) Application of economic analysis to diabetes and diabetes care. Ann Intern Med 140(11): 972-977.
-
Touray MML (2018) Estimation of Quality-adjusted Life Years alongside clinical trials: the impact of ‘time-effects’ on trial results. J Pharm Health Serv Res 9(2): 109-114.
-
Hensher DA, Rose JM, Ortúzar J de D, Rizzi LI (2009) Estimating the willingness to pay and value of risk reduction for car occupants in the road environment. Transp Res Part A Policy Pract 43: 692-707.
-
Experiments N (2008) Identification of Treatment Effects in Health Economics. Health Econ 16: 1127-1131.
-
Viscusi WK, Masterman C (2017) Anchoring biases in international estimates of the value of a statistical life. J Risk Uncertain 54(2): 103–128.
-
Jorgenson DW, Fraumeni BM (1989) Investment in Education. Educ Res 18: 35-44.
-
Dekker T, Brouwer R, Hofkes M, Moeltner K (2011) The Effect of Risk Context on the Value of a Statistical Life: A Bayesian Meta-model. Environ Resour Econ 49(4): 597- 624.
-
Lindhjem H, Navrud S, Braathen NA, Biausque V (2011) Valuing Mortality Risk Reductions from Environmental, Transport, and Health Policies: A Global Meta-Analysis of Stated Preference Studies. Risk Anal 31(9): 1381-1407.
-
Thaler RH, Rosen S (1976) The Value of Saving a Life: Evidence from the Labor Market, pp: 265-302.
-
Gunatilake HM (2003) Environmental Valuation: Theory and Applications.
- Are We Looking at an Overwhelming Crisis in Healthcare, or A Poorly Hidden Opportunity Calling on us to Improve our Systems? Perhaps Both?
- Sex, Metaphorical Drugs, and the Dissolution of Boundaries in the Perception of Time: Robert Muller’s Tropen: Der Mythos Der Reise (Tropics. The Myth of Travel) From 1915 Serves as an almost Forgotten Example
- Artificial Intelligence in Healthcare: Bioethical and Legal Challenges in the Brazilian Context
- Today Our Health and Our Principles are Challenged on Many Fronts Simultaneously, Where Can We Go from Here?
- The Value of Prevention, Avoid the Games and Focus on Real, Evidenced-Based Opportunities to Improve Health, Wellbeing and Longevity
- A Time of Opportunities to Improve our Health and Address Chronic Diseases