Important Update on Reducing Risk for Alzheimer’s disease, A Charge for Public Health and Clinical Medicine. Incorporating Current Information into Public Awareness, Public Health and Healthcare Practice
The Lancet Commission on Dementia Prevention, Intervention, and Care provides us with another groundbreaking report. This adds additional risk factors to the list, discusses many related issues and includes estimates of the number of people who would be spared the burden of dementia and the potential cost savings to society.
Abbreviations
LDL: Low-Density Lipoprotein; HHS: Health and Human Services; CDC: Centers for Disease Control and Prevention.
Commentary
The Lancet Commission on Dementia Prevention, Intervention, and Care provides us with another groundbreaking report. This adds additional risk factors to the list, discusses many related issues and includes estimates of the number of people who would be spared the burden of dementia and the potential cost savings to society.
Just so we’re all on the same page, this is the third iteration of the work of teams of experts from around the world convened by the British Medical Journal, The Lancet. Each prior report has energized public policy, education and clinical changes based on new knowledge and projections. This report takes it a step further, adding two additional risk factors: vision loss and high levels of low-density lipoprotein (LDL) cholesterol. Both add to the list of risk factors that Commentary critically can be understood and impacted by practice and behavior [1].
What are we talking about here, allow me to set the stage with some background for reference. Dementia is changes in the brain that result in loss of cognitive function that interferes with life. While Alzheimer’s disease is the most common, there are several others (Vascular dementia, Frontotemporal dementia, Lewy Body dementia and others). For brevity I will refer to these conditions collectively as “Alzheimers”. We learn more about these conditions though valuable research every year, but it is clear that many cases have multiple causes. We have recently had additional confirmation that there are steps that can be taken to reduce our risk for these conditions, this changes the long-standing conventional wisdom that there is nothing we can do to impact dementia. I’ll discuss that more below [2].
The conventional view that Alzheimer’s disease is a condition of aging, and little can be done to impact it’s onset and progress has been turned aside by a number of studies recently - the landmark Lancet Commission Reports from 2017 and updated in 2020 lead the way and are reinforced and enhanced by the newest iteration [1]. It is essential we now recognize Alzheimers as the public health threat that it is, as Dr David Satcher (Former Surgeon General and CDC Director) said in 2014 “Alzheimer’s is the most under- recognized threat to public health in the 21st century”. The three conditions that make it so are the significant burden, significant impact, and opportunity for intervention. This latest update highlights several opportunities for intervention, it is now up to policymakers and professionals to achieve this new potential.
According to the Alzheimers Association Facts and Figures 2022 publication, currently 6.5 million Americans have Alzheimers. This is likely to increase to 14 million by 2060 without intervention. This translates to 1 in 9 adults age 65+ and 2/3 are women [2]. Prior to the Covid19 Pandemic Alzheimers was the 5th leading cause of death (behind four conditions that all contribute to Alzheimers risk) [3]. The seriousness is exacerbated by evidence of racial and ethnic disparities.
One study quantified the differences as follows based on 2014 Medicare Data. Percentage of Adults Aged 65 and Older with Alzheimers Disease: African American - 14%; Hispanic - 12%; Non-Hispanic White - 10%. This inequity alone calls out for change, but when we consider the modifiable risk factors described below, correcting this inequity and this part of the intervention is even more important [4].
Other key factors calling out for action include that a large percentage of people with dementias and their caregivers are unaware of the diagnosis; about 25% of hospitalizations in this population were preventable; almost half these people talked to a healthcare provider about memory concerns; having another chronic condition is a complication; and 1 in 3 caregivers report worsening health and mental health.
For many years I had the professional good fortune to work at the New York State Department of Health with a team of dedicated professionals and talented partner organizations. New York is home to the oldest and most robust state public health program to address Alzheimers disease in the US [4]. This program took a two-pronged approach of funding Centers of Excellence to improve quality of professional care, early diagnosis and access to services and Caregiver Support Initiatives which recognized the reality that this is most often a condition shared with a family member (or others) who provide needed care in the home and benefit from supportive services (like those provided by the Alzheimer’s Association) [5].
This experience led to my participation in national efforts through the National Alzheimers Project Act (at HHS) and CDC’s Healthy Brain Initiative. These, along with national partners including the Alzheimers Association, National Association of Chronic Disease Directors, US against Alzheimers; and many more have expanded the knowledge of both the public and professionals over the past few years. Often this has taken the form of implementing the National Alzheimers Project Act Goals. This is especially seen in Goal #6: Accelerate Action to Promote Healthy Aging and Reduce Risk Factors for Alzheimers Disease and Related Dementias. Details of strategies can be found at [6]. The presence of this national goal offers us encouragement, a focal point and a target for action.
Many of the strategies needed to accomplish this are outlined in the national plan. These include continuing research to home in on the 55% of risk not currently clear. Facilitating the translation of risk reduction findings into clinical practice, to make the changes necessary to maximize the individual benefit and collective benefit. Acceleration of public health action to address risk factors - recognizing the commonality of risk with other conditions and maximizing impact by assuring the public understand these key aspects of Alzheimers risk. This includes prevention and management of chronic conditions with related risk factors and utilizing related systems (like the aging network). Recognizing and addressing the inequities I mentioned above and addressing these to mitigate the additional risk now present. The last strategy may be the most important, engage the public to reduce risk. By engaging the public we increase the likelihood of hitting more subtle risk factors. Remembering the value of more education throughout life beginning in early life (and quality education while we’re at it); avoiding hearing and vision loss and injury by using readily available safety devices (ear protection, bike helmets, etc.); recognizing and correcting the inequities between physical and mental health [6]; focusing on environmental risks where we can make a difference such as air quality; focusing more diligently on behaviorally related risk factors such as not smoking, keeping alcohol use in moderation, actively treating chronic conditions like high cholesterol, diabetes, depression, hypertension, obesity, and engaging in healthy eating and safe regular physical activity.
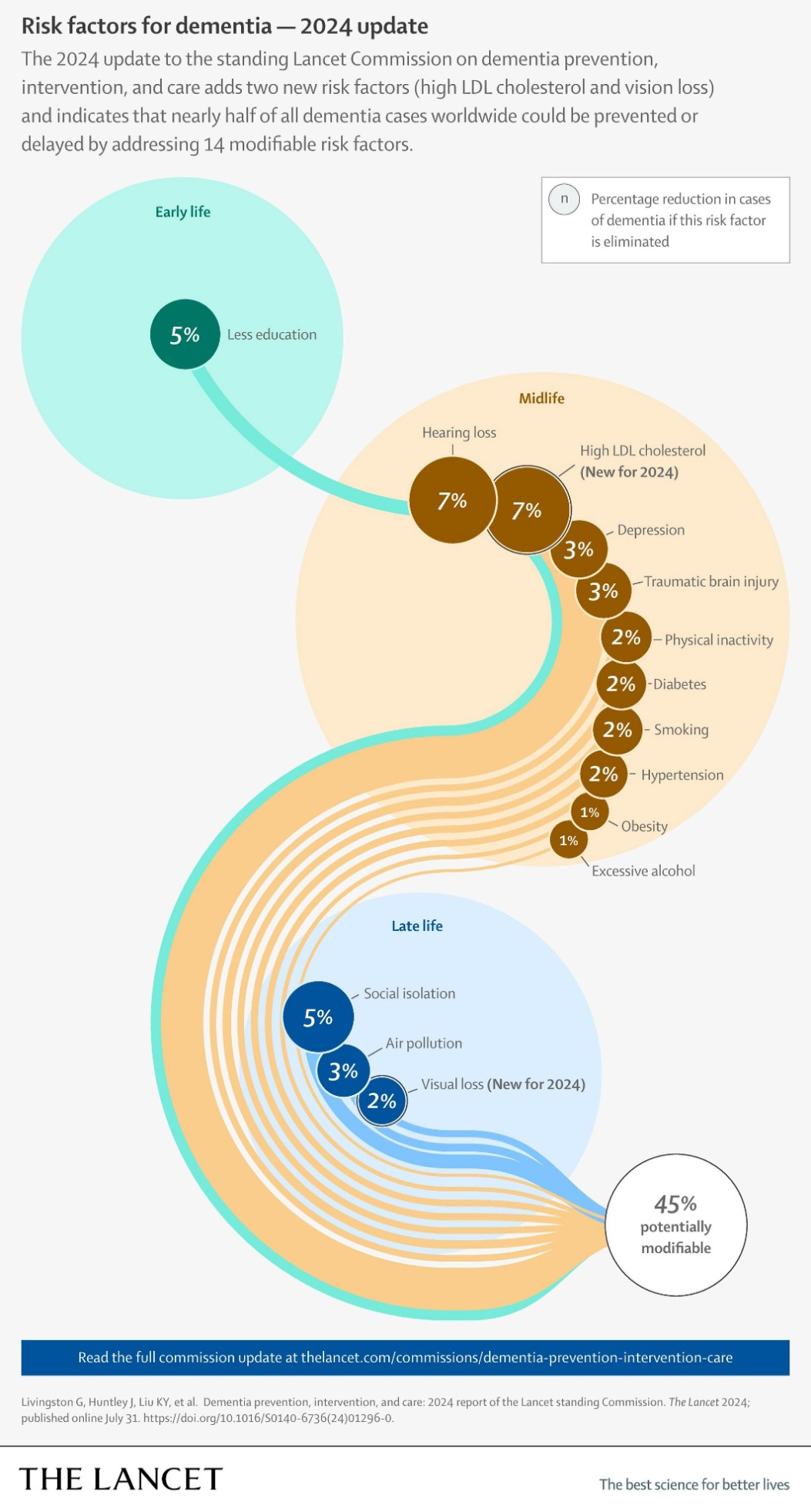
The time is right because we now have science demonstrating how we can intervene and reduce risk by as much as 45%. So what does this mean? What can we really do? The Lancet Commission highlighted in the following graphic risk factors where intervention could reduce risk, at what time in life this could have most impact and to what percent of the total of 45% each factor relates (Figure 1) [1].
This effort requires a robust population-wide intervention that includes public awareness, public health education, pre-service and in-service professional education, changes in clinical practice, and changes in public policy. The dual approach of pre-service and in-service professional education recognizes that collectively these reports change the former conventional wisdom that there was little that could be done, to the reality that there is much we can do. The relationship with risk factors for and other chronic conditions, modifiable risk factors that benefit quality of life (individual and family), health and longevity, also would result in the likelihood of significantly reduced system costs in health and related systems, and significant reductions in family expenses for care and services. Everything I’ve learned about ethics and health policy tells me this effort is essential and because the science and evidence is available and clearer than ever, this is an urgent matter. The fact that this confirms and expands on new knowledge raises the priority to clear up any misinformation that exists regarding dementias and their impact [7, 8].
Note that these opportunities span our lives, from assuring quality early education to an array of actions in mid- life with multiple positive benefits, to late life interventions that have now been shown to reduce risk or at least postpone onset of additional symptoms [1].
The principles of bioethics call on us to move with vigor and organize our efforts soon, educate policymakers so that policy change can drive progress and resources can be invested in appropriate ways to assure that progress occurs. The Lancet evidence makes clear that in doing so we will also reduce costs for care, both medical and social, far more than the costs of addressing this new knowledge [1]. The good news is that progress has begun with small steps. A new national plan with focus on risk reduction is now available, and DHHS, CDC and partners like the Alzheimer’s Association, National Association of Chronic Disease Directors have some tools available now [6, 9, 10, 11] that can make a difference and support a variety of professionals. The key will be to have sufficient resources to accomplish the mammoth task before us. We must collectively acknowledge the conventional wisdom is now different, and education and professional practice must reflect the opportunity to reduce risk and improve health associated with dementia, and happily also reduce risk and impact for many other chronic conditions at the same time.
References
-
Livingston G, Huntley J, Liu KY, Costafreda SG, Selbæk G, et al. (2024) Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet 404(10452): 572-628.
-
Hoffman DP (2022) Risk Reduction for Alzheimers Disease, Setting a Goal for All of Us: The Science and the Time are Right to Incorporate This into Public Awareness, Public Health and Healthcare Practice. Ann Bioethics Clin App 5(4): 000244.
-
Alzheimer’s Association (2024) Alzheimer’s disease Facts And Figures. Alzheimer’s Dement 20(5): 1-149.
-
CDC (2024) National Center for Health Statistics.
-
(2024) Alzheimer’s disease and Related Dementia. New York State.
-
(2021) National Plan to Address Alzheimer’s disease: 2021 Update. ASPE.
-
Hoffman DP (2023) When is it News? The Danger of Reporting Misinformation is that it Spreads, So Does the Damage. We Need to Prioritize a Principled Approach. Ann Bioethics Clin App 6(4): 000265.
-
Hoffman DP (2024) Why Disinformation Works. How Otherwise Reasonable People can Ignore Facts and Believe Purposeful Mistruths. What Next? Ann Bioethics Clin App 7(2): 000271.
-
Hoffman DP (2022) The Time has come to Apply Ethical Principles to Mental Health, Doing the Right Thing is Good for our Health. Ann Bioethics Clin App 5(3): 000239.
-
(2024) 10 Ways to Love Your Brain. Alzheimer’s Association.
-
(2024) Action on Healthy Aging and Brain Health. National Association of Chronic Disease Directors.
- Are We Looking at an Overwhelming Crisis in Healthcare, or A Poorly Hidden Opportunity Calling on us to Improve our Systems? Perhaps Both?
- Sex, Metaphorical Drugs, and the Dissolution of Boundaries in the Perception of Time: Robert Muller’s Tropen: Der Mythos Der Reise (Tropics. The Myth of Travel) From 1915 Serves as an almost Forgotten Example
- Artificial Intelligence in Healthcare: Bioethical and Legal Challenges in the Brazilian Context
- Today Our Health and Our Principles are Challenged on Many Fronts Simultaneously, Where Can We Go from Here?
- The Value of Prevention, Avoid the Games and Focus on Real, Evidenced-Based Opportunities to Improve Health, Wellbeing and Longevity
- A Time of Opportunities to Improve our Health and Address Chronic Diseases