Difficult Airway in the Periphery - An Onerous For the Anesthetist
A patient with slow-flow venous malformation of the head and neck region was managed with elective tracheostomy for the procedure of Sclerotherapy in the radiotherapy suite.
Introduction
International Society for the Study of Vascular Anomalies (ISSVA), in the year 1996, classified vascular anomalies based on their appearance, disease course, histopathologies and blood-flow characteristics. They divided them into two categories. First one being the proliferating vascular tumors called the heamangiomas and the second one being Vascular malformations. The latter are further divided into low-flow, high-flow or complex combined group based on their blood flow characteristics [1].
This classification has lead to the better understanding of the anomalies and advances in the field of radiology enable us to manage them in a better way by sclerotherapy and other percutaneous interventions [2].
Therefore patients with such anomalies visit the anesthesiologist very often in view of managing their complex airways in a peripheral setting, most likely a radiotherapy suite, where resources and man-power both are limited for an anesthetist and the complexity of the airway hardly gives time to shift between various plans of securing the airway.
Case Report
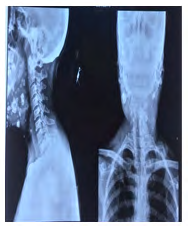
A 25 yr old, ASA physical status I patient reported to our institute with an indefinite generalized growth of soft tissue involving the oral cavity. On external appearance the growth was involving the lower lip and tongue, to the extent that in sitting position the patient had to support the tongue with her hand in order to keep it inside the oral cavity. On examination, she significantly commented that she could sleep only in the lateral position, though supine position could be tolerated for a few minutes. Deglutition and other daily chores were not an issue with her, only that in the upright position the tongue had to be supported all the time (Figure 1). Laboratory investigations showed all values within normal limits. Skiagram of chest and neck suggested normal lung fields and no compression or deviation of the airway. Though multiple phleboliths could be seen in the soft tissue around the naso and oro pharynx (Figure 2). Magnetic resonance imaging showed soft tissue swelling of 12*11*14 cm involving the masticator space, soft palate and nasopharynx superiorly. Inferior extent was upto the supraclavicular region bilaterally. Skin and subcutaneous tissue were invaded anteriorly and posteromedially the growth was abutting the sternocleidomastoid muscles bilaterally. Medially bilateral false vocal cords were involved and laryngeal compression was seen. Though trachea seemed to be normal but left vallecula and pyriform sinus were involved. Ultrasound was done and it was reported to be a slow flow venous malformation. Non-contrast Computerized Tomography was done, which reported tracheal airway column to be free of any external compression or invasion. On indirect laryngoscopy, the lesion was covering and compressing the epiglottis from the left side at such an angle that the true vocal cords and the chink of the glottic opening could not be seen. It was also commented that passage of tube under direct laryngoscopy was not possible. Considering the gravity of this airway, an elective preprocedure tracheostomy was planned. It was done after a through pre anesthetic check and in the operation theater. With all the preparation of difficult airway done, fiberoptic and videolaryngoscope kept ready, the procedure of tracheostomy was uneventful. We report this case to emphasize the fact that losing a patient to airway is very easy in a peripheral setup, so we should always be prepared to tackle such cases.

Discussion
As an anesthesiologist, securing an airway is our forte, and losing a patient due to airway will always leave a mark, irrespective of the number of years of experience that one has in the field. Therefore, it is always better to err on the side of caution. Anesthetic considerations of these patients are multi-factorial i.e type and extent of the lesion, clinical features, age and other comorbidities like coagulopathy and cardio-respiratory compromise. Pre-operatively, the airway should be thoroughly investigated using multiple modalities such as skiagram, MRI, NCCT and Ultrasonography of the lesion as well as the airway. Indirect laryngoscopy is a real- time tool for advice on airway and based on its report did we plan an elective pre-procedure tracheostomy.
The luxury of awakening the patient or regional anesthesia is not available in the peripheral settings [3]. Therefore, definitive airway management is the only answer to such airways where losing the airway can create a catastrophe.
Conclusion
Managing a difficult airway outside the operation theater is one of the biggest onerous of an anesthesiologist and one should always err on the side of caution.
References
-
Enjolras O (1997) Classification and management of the various superficial vascular anomalies: hemangiomas and vascular malformations. J Dermatol 24(11): 701- 710.
-
Lee BB, Bergan JJ (2002) Advanced management of congenital vascular malformations: a multidisciplinary approach. Cardiovasc Surg 10(6): 523-533.
-
Cook TM, MacDougall-Davis (2012) Complications and failure of airway management. Br J Anaesth 109: 168- 185.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index