Public Opinion on the Use of Psychedelics in the Treatment of Cluster Headache
Background: Anecdotal and survey evidence suggests that psychedelics such as psilocybin and LSD in low doses can improve cluster headaches. Up to 30% of people with cluster headaches cannot prevent headaches from occurring with conventional preventative treatments. Abortive and preventive medications have side effects which can be harmful, and there are reports that preventive medications can “wear out†over time. As a result, there is an urgent clinical need for alternative safe treatments that effectively abort and prevent the occurrence of cluster headache attacks. Current survey data suggests that psilocybin may be safer and more effective than current best medical therapy. Therefore, an online survey was conducted to assess the feasibility and acceptability of using these medications amongst the cluster headache community. Methods: The survey was conducted on social media platforms from 11th February-20th April 2020 and was funded with a National Institute for Health Research - Research Design Services Grant. The survey established if participants suffered from cluster headaches, the type, and their opinions on whether they considered psilocybin an acceptable drug to research and use as a medication. Results: In total 154 individuals with cluster headache took part. Findings revealed that 87% of respondents had little concern over the potential use of psilocybin as a treatment for cluster headaches. Although most concerns surrounded its legal status, dosage and side effect profile, 81% of respondents would consider using psilocybin if it was demonstrated to be beneficial. Of the 30 respondents who admitted to using psychedelics to treat cluster headaches, 80% rated it 8, 9 or 10 out of 10 for effectiveness. 78% of respondents would consider entering a study with this medication. Conclusions: Findings suggest there is considerable interest in psilocybin as a potential medication in individuals with cluster headache. The majority of respondents would consider entering a study investigating low dose psilocybin in cluster headache. Surveyed effectiveness of psychedelic use in reducing cluster headaches appears to be strong. Clinical research is needed to establish efficacy, safe dosing strategies and side effect profiles.
Introduction
Cluster headaches are the most intense primary headache with a lifetime prevalence of around 1 in 800 persons. It is a disabling primary headache disorder characterised by attacks of intense headache on one side of the head. Cluster headache has significant negative effects on quality of life, day-to-day functioning and ability to work [1] and is associated with high healthcare costs [2]. Due to the severity of cluster headache, it is associated Andersson with significant morbidity with nearly 80% of sufferers reporting restrictions on their daily activities during attacks (NICE, 2017). It can be described as the worst pain with suicide and suicidal ideation not uncommon during cluster headache periods [3]. There is a group of cluster headache sufferers who are unable to manage their symptoms with conventional medications and are using psychedelic drugs, such as psilocybin, in an unregulated and uncontrolled manner to ease symptoms [4]. This therefore suggests there is an urgent need to carefully research the safety and efficacy of these drugs. As there is limited research exploring the views towards psilocybin in the cluster headache community, we undertook an online survey exploring the perspectives of individuals with cluster headache surrounding potential research investigating psilocybin in this condition.
Presentation
Cluster headache can take different clinical courses. Episodic cluster headache is characterised by daily headache attacks that occur over periods of weeks or months with pain-free periods of remission. Chronic cluster headache is characterised by cluster headache attacks occurring for one year or longer without remission, or with remission periods lasting less than 3 months. Chronic cluster headache may arise de novo, or evolve from episodic cluster headache, and occurs in 10-15% of cases. Attacks can last 15 to 180 minutes when untreated and can occur once or several times per day [5]. The pain of cluster headache is maximal orbitally, supraorbitally, temporally or in any combination of these sites, and may spread to other regions. This intense pain can be accompanied with agitation and cranial autonomic symptoms, such as lacrimation, conjunctival injection, and nasal congestion [5]. During the worst attacks, the intensity of pain is excruciating. Patients are usually unable to lie down, and characteristically pace the floor. Pain usually recurs on the same side of the head during cluster periods. Structural differences in grey matter density in the inferior posterior hypothalamus are apparent between individuals with cluster headache and healthy controls [6], and brain activity in this area increases during acute attacks [6]. Evidence also seems to suggest there may be a genetic component to inheriting cluster headache [1]. However, findings are not conclusive: mode of inheritance has been shown to be autosomal recessive in some families [7] and autosomal dominant in others [8]. This in turn influences the prevalence rate between genders and age groups [1].
Current Treatment Options
Abortive treatments: Abortive treatments for cluster headache aim to stop attacks as quickly as possible after onset. In the UK, NICE currently recommends two types of abortive treatments. The first is short burst oxygen therapy: delivering 100% oxygen at a flow rate of 12-15 litres per minute via a non-rebreather facemask for 15 to 20 minutes. Home oxygen is provided through a home oxygen order system and is effective in two thirds of cluster headache attacks [9]. The second are Triptans which are effective at treating approximately 45-75% of acute cluster headache attacks [10]. Triptans, such as sumatriptan and zolmitriptan, are selective agonists of serotonin (5-hydroxytryptamine [HT]) receptors that activate 5-HT1B and 5-HT1D (5-HT1B/1D) receptors. They are licenced for use in persons between the ages of 18 and 65 years (i.e. not for individuals over the age of 65 years of age), and can be administered intranasally or subcutaneously with the dose depending on the route and drug. A maximum of two doses are permitted per day, and only one dose is permitted per headache attack. If a patient has more than two cluster headaches per day, or has a cluster headache that does not respond to one dose, they are left only with high flow oxygen as a treatment option. Mild to moderately severe side effects are associated with triptans, including burning around the injection site (nose or skin), nausea or vomiting, dizziness and drowsiness [10]. Triptans are known to narrow human coronary arteries in vivo by 20% during angiography [11, 12] and whilst uncommon they have been associated with an increased risk in cardiac events and cerebrovascular accidents [12]. There therefore exists a large group of patients for whom triptans can potentially be dangerous, including those with high blood pressure and pre-existing cardiac problems [13] they can also lead to chronic headache [14]. A retrospective study of cluster headache sufferers who used triptans on a regular basis felt the attacks occurred more frequently, were more intense and the medication was becoming less effective [15].
Preventative Treatments
Although preventative treatments aim to reduce the frequency of cluster headache attacks the most recent open-label trial showed 45% of chronic cluster headache patients cannot prevent headaches from occurring with the first choice treatment verapamil [16]. Verapamil has a 69% response rate when used as a preventive medication in cluster headache [17]. However, verapamil is licensed as a cardiac drug used to treat arrhythmias, and has been associated with side effects such as cardiac conduction blocks, bradycardia, and constipation when used to treat cluster headaches [17, 18]. It therefore requires the patient to have an electrocardiogram (ECG) before any dose changes [18]. Another preventative treatment for cluster headache is lithium, which is most commonly used in bipolar disorder. Unfortunately, there is only limited evidence supporting its use as a preventative treatment in cluster headache [19, 20] and has been associated with side effects [21]. As 10-20% of patients with cluster headache develop resistance to conventional treatments [22, 15], and the severity of attacks has also led to the use of surgical treatments (e.g. deep- brain stimulation [23], trigeminal nerve-root section [24], and occipital-nerve stimulation [25]) which are not without serious risks, there is an urgent need to establish safer and more effective treatments for cluster headache [26].
History of Serotonergic Agonist Use in the Treatment of Headaches
Dr. Sicuteri introduced the concept that migraine may be caused by vasoneuroactive substances in 1959, with serotonin being the most important chemical due to its ability to provoke pain, sensitise pain receptors and produce vasoconstriction [27, 28, 29]. Following this theory, the effectiveness of methysergide was revealed, subsequently forming the basis for all subsequent experiments with 5HT receptor agonists, including LSD and the most recent development of sumatriptan (Imitrex™). Methysergide’s chemical structure is very similar to LSD and it is also psychotropic in supratherapeutic doses [4]. Unfortunately, the compound (Sansert™) is no longer available due to reports of retroperitoneal fibrosis following long-term use. However, a survey among members of the International Headache Society showed that a vast majority would prescribe the drug to a specific group of patients if it were available due its effectiveness [30]. An open label non- randomised case series using another ergot-based drug, the non-hallucinogen 2-bromo-LSD, for the treatment of episodic and chronic cluster headache demonstrated all 5 participants experiencing complete or near complete remission of all headache symptoms for at least 3 months [31].
Psilocybin in cluster headache
In 1998, a cluster headache sufferer posted online about his treatment of cluster headaches with psilocybin. Word spread of this treatment option amongst the cluster headache community and others tried it, achieving promising results. A core group of advisors emerged, to champion the use case of psilocybin and LSD in the treatment of cluster headaches. In 2001, the website www.clusterbusters.com was created which provides suggested psilocybin regimes to break cluster cycles and treat acute attacks.
Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine) is a 5HT2a receptor agonist and a substituted indolealkylamine, belonging to the group of hallucinogenic tryptamines. Psilocybin was isolated from Central American mushrooms (Psilocybe Mexicana) by the renowned Swiss chemist Albert Hofmann in 1957, and in 1958 was produced synthetically for the first time. It has been found in many species of mushrooms worldwide [32]. In a medium dosage (12–20 mg p.o.), psilocybin was found to produce a well- controllable altered state of consciousness [32]. This state is marked by stimulation of affect, enhanced ability for introspection and altered psychological functioning in the direction of Freudian primary processes, known otherwise as hypnagogic experience and dreams. Especially noteworthy are perceptual changes such as illusions, synesthesia’s, affective activation, and alterations of thought and time sense. The effects last from 3 to 6 hours [32].
Psilocybin is currently a schedule one drug (https:// www.gov.uk/government/publications/controlled- drugs-list--2/list-of-most-commonly-encountered-drugs- currently-controlled-under-the-misuse-of drugs-legislation). However, its safety and efficacy has been demonstrated in multiple recent pilot studies including; anxiety in patients with advanced stage cancer, treatment resistant depression, treatment of OCD, alcohol dependence and smoking cessation [33, 34, 35, 36, 37, 38]. Internationally, there are currently 45 studies exploring the efficacy of psilocybin in multiple psychiatric and neurological pathologies including addiction, treatment resistant depression, anxiety associated with terminal illness, episodic cluster headache, post-traumatic headache, migraine and short-term memory loss (https:// clinicaltrials.gov/ct2/results?cond=&term=psilocybin). Recent safety data of a double-blind randomised control study of psilocybin use in 89 healthy volunteers randomised to either high dose (25mg), low dose (10mg) of psilocybin or placebo in the presence of a psychological therapy support demonstrated no serious adverse effects, with no negative effects on emotional and cognitive functioning [39]. Additionally, in 2006, an internet survey of 53 individuals with cluster headache reported that psilocybin was better at aborting acute attacks than either oxygen or sumatriptan [4]. Furthermore, findings showed that LSD and psilocybin were both better at triggering and extending remission than standard drugs [4]. This preliminary evidence therefore suggests that psilocybin may be a more effective preventive and/or abortive treatment and have fewer side effects than existing therapies for the treatment of cluster headache.
Study Aim
Despite the preliminary evidence suggesting that psilocybin may be safer and more effective to treat cluster headaches than conventional strategies, it is unclear how psilocybin is perceived in the cluster headache community. We therefore undertook an online survey to ascertain perspectives surrounding psilocybin in a sample of individuals with cluster headache. It was hoped that the data generated from this work would contribute to designing a clinical research study investigating the safety and effectiveness of psilocybin in individuals with this condition.
Methods
Participants
The aim was to principally target male and female individuals who experienced cluster headache. To ensure a representative sample was obtained, a sample size of 100 was envisaged. There were no inclusion or exclusion criteria for the survey as the purpose was to gauge the community response to the use of psilocybin as a treatment for cluster headaches.
The survey
Following the securing of an NIHR research design services public and patient involvement grant, we developed a survey to assess the feasibility and acceptability of low dose psilocybin use for the treatment of cluster headaches. The anonymous survey introduced the rationale behind the questionnaire and information regarding psilocybin. A combination of single answer and free text questions asked respondents about their experiences and concerns surrounding the use of psychedelics to treat cluster headaches. We were also interested in exploring the views of the cluster headache community towards future research examining the efficacy and safety of psilocybin in the treatment of this condition. The survey was posted on cluster headache social media groups over the period of February 2020 to April 2020. Please see the Supplementary section for a copy of the survey (including introduction and instructions) that was presented to respondents.
Analysis
Responses to single answer questions were counted and percentages generated. Themes from the free text answers were identified and used to provide additional information to the single answer responses. This resulted in the identification of three key areas:
- Previous experience with psychedelics
- Concerns about psilocybin.
- Future research exploring psilocybin use in the treatment of cluster headache.
Results
The sample
In total, 154 individuals completed the survey, with 152 confirming they suffered from cluster headaches. 30% of the sample (n = 48) reported they suffered from chronic cluster headaches.
Previous experience with psychedelics
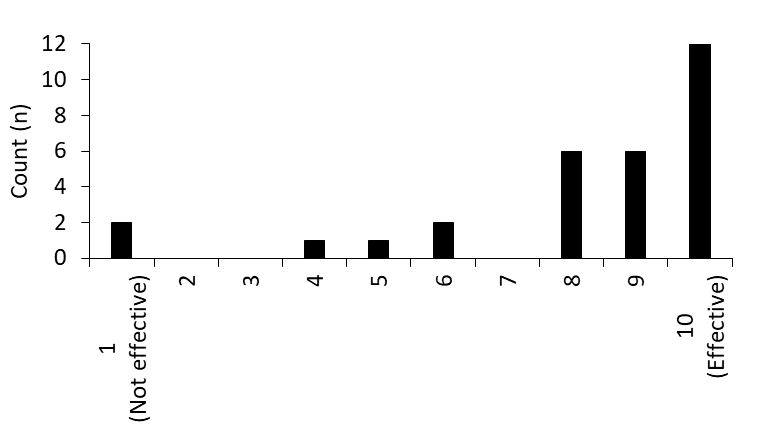
Thirty respondents had previously used psychedelic substances to try to ease their cluster headaches. Interestingly, 80% of these individuals experienced 80- 100% relief using these substances, and 93% rated it 40% or greater in effectiveness (Figure 1).
Free text responses revealed that some respondents had ’amazing results’, with psilocybin breaking cluster headache cycles: ’Have suffered with clusters for 9 years. Managed to bust my last cycle in 4 weeks using psilocybin they usually last 10-12 weeks’. Beneficial effects were experienced following one dose: ’I just tried a 0.15 dose once. It seems it worked for 3 weeks (impossible for me to find it, it was a coincidence thanks to a friend that gave me that)’. This has encouraged some to continue taking psilocybin, and other psychedelics, to experience longer-term pain relief: ’I’m chronic and consume mushrooms almost every single day. I’ve become entirely tolerant to the psychedelic effects, but it always eliminates or greatly reduces the pain. I’ve also had great success with LSD, DMT, and ketamine’. Although most responses are indicative of the positive effects of psilocybin, some encountered little benefit: ’It did not work for me after following all the suggested steps’. One possible reason for this could have been a lack of clarity about the correct dosing of psilocybin: ‘I tried it once to see but had very little and wasn’t sure if I dosed properly’. Of note there were no negative effects reported by these individuals.
Concerns about psilocybin
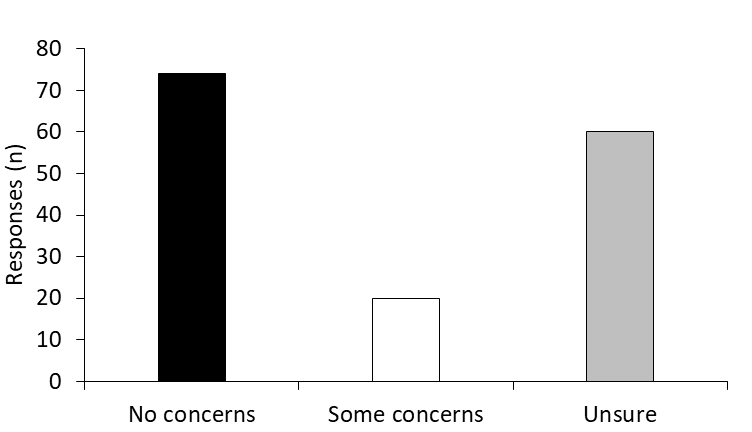
Around 48% of respondents reported having no concerns about psilocybin, with 39% saying they were unsure and the remaining 13% stating they had some concerns about the drug (Figure 2). When asked to freely state concerns around psilocybin, the legality of the drug was a worry: ‘The fact that it is illegal in some jurisdictions concerns me’. Furthermore, the issue of legality was compounded by a lack of standardisation around manufacturing and dosing: My concern is that whilst the risk is small, proponents of the use of psilocybin for any therapeutic use never discuss those risks. Also, as it is not legal on a national level, the production is unregulated, and dosages and potency are not standardized’.
‘Side effects’ also appeared to be an issue for some respondents, particularly those focused around mental health. Reports that ‘life / mind altering without control’ aspects of the drug were concerns: ’I don’t wanna lose myself, even if maybe it would be better’. There were also concerns there may be serious adverse events occurring with their recreational use ‘… I have seen too many people in the past who developed drug induced psychosis because of its use’. However, there was also a sense of acknowledgement that ‘… all meds (I’ve tried) have some negative effects’, suggesting that the benefit of alleviating cluster headaches with psilocybin may outweigh its side-effect profile, and those of current treatments: ‘We have read a lot about it and are not concerned as the reported effects are less than medications offered by allopathic medicine’. Some participants demonstrated they would want to see evidence of a long-term safety profile of psilocybin ‘...I’d prefer a study on mushrooms that looks into the long-term effect within the brain/memory’ and also an understanding about the mechanism of action of pain relief from these drugs. ‘I’ll do almost anything to stop them. My only concerns are the legality and if they actually treat it or mask the pain’. Due to the unregulated nature of psilocybin there were also concerns about obtaining it and drug preparation ‘Afraid when collecting, may collect wrong mushrooms. Once collected, concerned about correct preparation’. Dosage also emerged as a common worry: ‘My concern would be to get the dosing right, I wouldn’t know what correct dose would be but would be willing to try anything when in cycle’. Some advocates of psilocybin reported few concerns: ‘None, I actually recommend it’ because ‘… you don’t need to take enough to be tripping’. With others asking: ’My concern is why is it not available on the NHS?’ and ‘Where to get it’.
Future Research Exploring Psilocybin in Cluster Headache
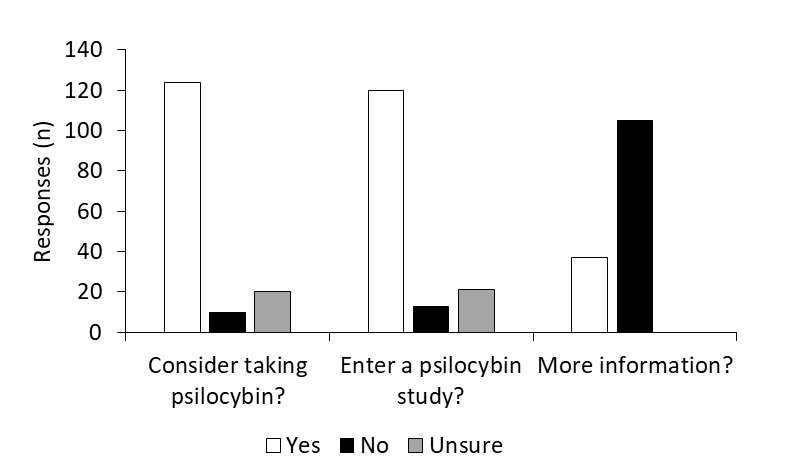
When asked about whether respondents would consider taking the medication, 81% said yes, 6% said no and 13% said they were unsure. Furthermore, the majority of respondents (78%) said they would consider entering a study investigating the effects of psilocybin in cluster headache, whilst 14% were unsure and 8% said it would not be considered. Respondents seemed to prefer the controlled nature of a clinical trial: ’If I was going to try it, it would have to be in a controlled setting…’. The advantages of trialling psilocybin seem to outweigh the associated risks: ‘I am the partner of a person living with CH. My partner has participated in clinical trials before, and I would definitely be good with them participating in one on psilocybin. From my perspective, the risk of (mainly psychological) harm is real, but small, and with psilocybin produced and administered in a controlled environment with the oversight of pharmaceutical and medical experts, that risk would be further reduced. The risk vs reward would lead me to advocate for participation’. In addition, most respondents (74%) felt they did not require any further information to make their decision about participating in a psilocybin trial in cluster headache.
Discussion
Findings from this online survey (n = 154 respondents) revealed that individuals with cluster headache are or have previously used psychedelics, including psilocybin in an unregulated and uncontrolled manner to ease their suffering (n = 30). Although most prior experience appears to be positive, some respondents reported limited efficacy. The majority of respondents reported no concerns about psilocybin (around 48%). But for those who had some concerns (13%), issues seemed to focus on legality, side effect/risk profile and dosing regimens. Findings also showed there was considerable interest from this sample in trying psilocybin as a potential medication for cluster headache. The proposal for a clinical trial investigating the efficacy and safety of psilocybin in cluster headache was well-received, with around 78% of respondents stating they would consider entering such a study. This therefore suggests that psilocybin appears acceptable as a medication amongst most of the cluster headache community and urgently warrants investigation in carefully monitored clinical trials.
Positive effects and perceptions of psychedelics in the cluster headache community
Current treatments for cluster headache, such as
short burst oxygen, triptans, lithium and verapamil, have limited effectiveness and are not risk-free [10, 19, 20, 21]. This has resulted in individuals with cluster headache feeling dissatisfied with conventional treatments [40], and as though they have not received adequate treatment with potential misdiagnoses [41]. These sentiments, compounded by stress, anxiety and suicidal ideation, have contributed to individuals with cluster headache seeking other forms of treatment, including illicit drugs [4, 40, 41]. Findings from the current online survey found that 30 out of 154 respondents were or had previously used psychedelic substances to treat their cluster headache. As psychedelics are illegal in most jurisdictions, this therefore suggests that despite the legal status of these substances, individuals with cluster headache are prepared to take them without regulation or the involvement of healthcare professionals [42].
Even though psychedelic drugs are typically viewed as harmful or ‘drugs of abuse’ by the general public [43], evidence suggests they are perceived more positively in the cluster headache community. Indeed, the majority of respondents (around 48%) reported having no concerns about psilocybin. Comparatively, in an Italian online survey, 48 participants (85.7%) stated that they did not perceive psychedelics as less safe than conventional treatments [40]. Furthermore, 30 participants (55.6%) even considered their use of illicit drugs to be safer than conventional therapies with some saying they would consider recommending such illicit drugs as treatments to other sufferers [40]. Interestingly, only four patients (7.4%) reported that legality prompted some concerns [40]. Although it is unclear how many respondents in the current study were concerned about the legal implications of psilocybin, free text answers revealed it was concern for some. For the first time, this survey showed that respondents had some concerns surrounding how to correctly dose the drug and its potential side-effects, particularly with its long- term use. We therefore feel that education surrounding the drug and its effects would address a large number of these types of concerns. Current education practices seem to be informal, via online forums specifically for the cluster headache community. For instance, in a qualitative study exploring discussions on online cluster headache forums, Andersson, et al. [41] revealed that dosage and regimens were key discussion points. Members were found to provide ways to bust cluster headache cycles (i.e. how to administer psychedelics in moderate to medium doses that are strategically timed with cluster headache episodes). Micro- dosing techniques (taking a sub-perceptual dose) and full doses (starting with a tiny dose and gradually increasing the dosage until beneficial effects are achieved) were also focal points. In terms of severe adverse effects, none were reported. Also, although there were some accounts of discomfort, temporarily increased symptoms, residual anxiety and unexpected emotional experiences, most self- reported outcomes were positive.
Perhaps the positive perceptions of psychedelics in the cluster headache community are due to users experiencing improvements in their symptoms. For instance, to explore the use, efficacy and safety of psychedelics in cluster headache, Sewell, et al. [4] interviewed 53 individuals with cluster headache who had used psilocybin or LSD as a treatment. Out of 26 participants who had used psilocybin, 22 reported that the drug aborted attacks (i.e. ended an attack within 20 minutes). Furthermore, 25 out of 48 psilocybin users reported cluster period termination (i.e. total cessation of attacks) with 18 out of 19 participants reporting a lengthening to the remission period. More recently, the Cluster busters medication use survey found that psilocybin was reported by respondents to be more effective than other preventative and abortive medications whilst also having few side effects [44]. Consistent with these findings, we found that 80% of respondents encountered 80-100% relief after using psychedelics with 93% rating it 40% or greater in effectiveness.
Future Research
Findings from the current online survey are important and timely, suggesting that individuals with cluster headache do turn to psilocybin to self-treat with positive effects. However, it should be acknowledged that the sensitive and self-selecting nature of the survey may have biased responses. This therefore reinforces the importance of undertaking clinical trials that can quantify the magnitude of improvements in symptoms as well as any associated side effects. Due to the rich information that can be gathered via qualitative methods, future research could adopt a multi-method approach where quantitative outcomes can be substantiated by more personal accounts. Clinical trials investigating the efficacy and safety of low dose psilocybin in cluster headache seems feasible given the large number of respondents who would consider entering a study of this kind.
Conclusion
Findings showed that there is a cohort of individuals with cluster headache who have previously used psychedelics to alleviate their symptoms. The majority of respondents reported no concerns about the use of psilocybin as a medication for cluster headache (around 48%) and those who have previously used it reported positive effects (80% with 80 - 100% relief) and no personal experiences of negative side effects were reported. For those who did have concerns (13%), issues seemed to focus on legality, dosing regimens, and side effects, particularly with long-term use.
Findings also clearly showed there was considerable interest from this sample of cluster headache sufferers in trying psilocybin as a potential treatment, and around 78% of respondents said they would consider entering a clinical trial investigating the efficacy and safety of low dose psilocybin in cluster headache. Psilocybin appears to be viewed positively and as a potential acceptable treatment amongst most of the cluster headache community. The impact this condition has on the quality of life of the sufferers and their families warrants urgent carefully monitored clinical trials to explore the effectiveness and safety profile of low dose psilocybin in the treatment of cluster headache. The results of this survey suggest it is feasible and acceptable to perform this study.
References
-
Hoffmann J, May A (2018) Diagnosis, pathophysiology, and management of cluster headache. Lancet Neurol 17(1): 75-83.
-
Gaul C, Finken J, Biermann J, Mostardt S, Hans Christoph D, et al. (2011) Treatment costs and indirect costs of cluster headache: A health economics analysis. Cephalalgia 31(16): 1664-1672.
-
Rozen TD, Fishman RS (2012) Cluster Headache in the United States of America: Demographics, Clinical Characteristics, Triggers, Suicidality, and Personal Burden*. Headache: The Journal of Head and Face Pain 52(1): 99-113.
-
Sewell RA, Halpern JH, Pope HG (2006) Response of cluster headache to psilocybin and LSD. Neurology 66(12): 1920-1922.
-
Olesen J (2013) The International Classification of Headache Disorders 3rd (Edn.), (Beta Version). Cephalalgia 33(9): 629-808.
-
May A, Ashburner J, Buchel C, McGonigle DJ, Friston KJ, et al. (1999) Correlation between structural and functional changes in brain in an idiopathic headache syndrome. Nat Med 5(7): 836-838.
-
De Simone R, Fiorillo C, Bonuso S, Castaldo G (2003) A Cluster headache family with possible autosomal recessive inheritance. Neurology 61(4): 578-579.
-
Russell MB, Andersson PG, Thomsen LL, Iselius L (1995) Cluster headache is an autosomal dominantly inherited disorder in some families: a complex segregation analysis. J Med Genet 32(12): 954-956.
-
Cohen AS, Burns B, Goadsby PJ (2009) High-Flow Oxygen for Treatment of Cluster Headache. JAMA 302(22): 2451- 2457.
-
Law S, Derry S, Moore RA (2013) Triptans for acute cluster headache. Cochrane Database Syst Rev 4: CD008042.
-
Welch KM, Mathew NT, Stone P, Rosamund W, Saiers J, et al. (2000) Tolerability and appropriate use of sumatriptan: clinical trials and post-marketing experience. Cephalalgia 20(8): 687-669.
-
MacIntyre PD, Bhargava B, Gemmill JD, Hillis WS (1993) Effect of subcutaneous sumatriptan, a selective 5HT1 agonist, on the systemic, pulmonary, and coronary circulation. Circulation 87(2): 401-405.
-
Tepper SJ, Millson D (2003) Safety profile of the Triptans. Expert Opin Drug Saf 2(2): 123-132.
-
Kristoffersen ES, Lundqvist C (2014) Medication-overuse headache: Epidemiology, diagnosis and treatment. Ther Adv Drug Saf 5(2): 87-99.
-
Dousset V, Chrysostome V, Ruiz B, Irachabal S, Lafittau M, et al. (2004) Does repeated subcutaneous administration of sumatriptan produce an unfavorable evolution in cluster headache?. The Journal of Headache and Pain 5(2): 110-114.
-
Blau JN, Engel HO (2004) Individualizing Treatment with Verapamil for Cluster Headache Patients. Headache: The Journal of Head and Face Pain 44(10): 1013-1018.
-
Leone M, Amico DD, Frediani F, Moschiano F, Grazzi L, et al. (2000) Verapamil in the prophylaxis of episodic cluster headache: A double-blind study versus placebo. Neurology 54(6): 1382-1385.
-
Cohen AS, Matharu MS, Goadsby PJ (2007) Electrocardiographic abnormalities in patients with cluster headache on verapamil therapy. Neurology 69(7): 668-675.
-
Bussone G, Leone M, Peccarisi C, Micieli G, Granella F, et al. (1990) Double Blind Comparison of Lithium and Verapamil in Cluster Headache Prophylaxis. Headache 30(7): 411-417.
-
Steiner TJ, Hering R (1997) Double-Blind Placebo- Controlled Trial of Lithium in Episodic Cluster Headache. Cephalalgia 17(6): 673-675.
-
De Coo IF, Haan J (2016) Long Lasting Impairment of Taste and Smell as Side Effect of Lithium Carbonate in a Cluster Headache Patient. Headache: The Journal of Head and Face Pain 56(7): 1201-1203.
-
Gooriah R, Buture A, Ahmed F (2015) Evidence-based treatments for cluster headache. Ther Clin Risk Manag 11: 1687-1696.
-
Leone M, Franzini A, Broggi G, May A, Bussone G (2004) Long-term follow-up of bilateral hypothalamic stimulation for intractable cluster headache. Brain 127(10): 2259-2264.
-
Jarrar RG, Black DF, Dodick DW, Davis DH (2003) Outcome of trigeminal nerve section in the treatment of chronic cluster headache. Neurology 60(8): 1360-1362.
-
Mueller OM, Gaul C, Katsarava Z, Diener HC, Sure U, et al. (2011) Occipital Nerve Stimulation for the Treatment of Chronic Cluster Headache-Lessons Learned from 18 Months Experience. Cen Eur Neurosurg 72(2): 84-89.
-
Davenport WJ (2016) Psychedelic and nonpsychedelic LSD and psilocybin for cluster headache. Canadi Medic Associ J 188(3): 217.
-
Sicuteri F (1959) Prophylactic and Therapeutic Properties of 1-Methyl-Lysergic Acid Butanolamide in Migraine. Int Arch Allergy Immunol 15(4-5): 300-307.
-
Sicuteri F, Franchi G, Del Bianco P L (1967) An Antaminic Drug, BC 105, in the Prophylaxis of Migraine. Int Arch Allergy Immunol 31(1): 78-93.
-
Sicuteri F (1976) Migraine, A Central Biochemical Dysnociception. Headache: J Head Face Pain 16(4): 145- 159.
-
MacGregor E A, Evers S (2017) The role of methysergide in migraine and cluster headache treatment worldwide-A survey in members of the International Headache Society. Cephalalgia 37(11): 1106-1108.
-
Karst M, Halpern JH, Bernateck M, Passie T (2010) The non-hallucinogen 2-bromo-lysergic acid diethylamide as preventative treatment for cluster headache: An open, non-randomized case series. Cephalalgia 30(9): 1140- 1144.
-
Passie T, Seifert J, Schneider V, Emrich HM (2002) The pharmacology of psilocybin. Addiction Biology 7(4): 357-364.
-
Harris C, Bolstridge M, Rucker J, Camilla MJ Day, Erritzoe D, et al. (2016) Psilocybin with psychological support for treatment-resistant depression: an open-label feasibility study. The Lancet Psychiatry 3(7): 619-627.
-
Grob CS, Danforth AL, Chopra GS, Hagerty M, McKay CR, et al. (2011) Pilot Study of Psilocybin Treatment for Anxiety in Patients With Advanced-Stage Cancer. Arch Gen Psychiatry 68(1): 71-78.
-
Moreno FA, Wiegand CB, Taitano EK, Delgado PL (2006) Safety, Tolerability, and Efficacy of Psilocybin in 9 Patients with Obsessive-Compulsive Disorder. J Clin Psychiatry 67(11): 1735-1740.
-
Bogenschutz MP, Forcehimes AA, Pommy JA, Wilcox CE, Barbosa PCR, et al. (2015) Psilocybin-assisted treatment for alcohol dependence: A proof-of-concept study. J Psychopharmacol 29(3): 289-299.
-
Johnson MW, Garcia Romeu A, Cosimano MP, Griffiths RR (2014) Pilot study of the 5-HT 2A R agonist psilocybin in the treatment of tobacco addiction. J Psychopharmacol 28(11): 983-992.
-
Johnson MW, Garcia Romeu A, Griffiths RR (2017) Long-term follow-up of psilocybin-facilitated smoking cessation. Am J Drug Alcohol Abuse 43(1): 55-60.
-
Rucker J, Young A, Williams S, Stansfield S, Eriksson H, et al. (2019) Psilocybin Administration to Healthy Participants: Safety and Feasibility in a Placebo- Controlled Study. Neuropsychopharmacology 44 (1): 443-444.
-
Di Lorenzo C, Coppola G, Lorenzo GD, Bracaglia M, Rossi P, et al. (2016) The use of illicit drugs as self-medication in the treatment of cluster headache: Results from an Italian online survey. Cephalalgia 36(2): 194-198.
-
Andersson M, Persson M, Kjellgren A (2017) Psychoactive substances as a last resort-a qualitative study of self- treatment of migraine and cluster headaches. Harm Reduction J 14(1): 60.
-
Govare A, Leroux E (2014) Licit and Illicit Drug Use in Cluster Headache. Curr Pain Headache Rep 18(5): 413.
-
Tupper KW, Wood E, Yensen R, Johnson MW (2015) Psychedelic medicine: a re-emerging therapeutic paradigm. Canad Medic Assoc J 187(14): 1054-1059.
-
Schindler EAD (2015) Indoleamine Hallucinogens in Cluster Headache: Results of the Clusterbusters Medication Use Survey. J Psychoactive Drugs 47(5): 372- 381.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index