Comparison of Motor Seizure Duration of Ketofol and Propofol for Electroconvulsive Therapy
Objectives: Propofol and ketamine have become progressively popular in electroconvulsive therapy (ECT) anesthesia. Ketofol is a combination of ketamine and Propofol, and the current study was designed to evaluate the effect of Ketofol and Propofol on motor seizure duration, hemodynamic profile and recovery times in patients undergoing ECT. Methods: Fifty-four ECT sessions were randomized into Ketofol and Propofol group. Motor seizure duration, hemodynamic profile and recovery times were recorded. Results: Motor seizure duration in Ketofol group (28.55 + 6.54 seconds) was longer than Propofol group (22.22 + 7.94 seconds) which was statistically significant (p =0.002). Both drugs had motor seizure duration within the therapeutic range. At 1 min after the end of seizure heart rate in Propofol group (97.40 + 18.18 bpm) was lower compared to Ketofol group (109.37 + 17.69 bpm) which was statistically significant (p= 0.017). Similarly at 5 min after the end of seizure the heart rate in Propofol group (95.25 + 10.38 bpm) was lower compared to Ketofol group (102.51 ± 13.65) which was statistically significant (p= 0.032). There was no statistically significant difference in recovery times between Ketofol and Propofol group. Conclusion: Although Ketofol 1:1 mixture is associated with a longer motor seizure duration than Propofol in ECT anesthesia, both drugs are equally effective in producing motor seizure duration within the therapeutic range.
Introduction
Electroconvulsive therapy (ECT) remains a widely used effective and safe treatment for a variety of complicated psychiatric conditions including severe and medication- resistant depression and mania, as well as in the treatment of schizophrenic patients with affective disorders, suicidal drive, delusional symptoms, vegetative dysregulation, inanition and catatonic symptoms [1]. Most ECT procedures are carried out with muscle paralysis under general anesthesia [2]. Therapeutic adequacy of ECT can be determined by monitoring the seizure duration which can be done by either with electroencephalogram or by observation of motor seizure. The motor seizure duration has been considered as a standard for determining the therapeutic adequacy [3]. A motor seizure lasting 20–25 seconds at minimum is considered adequate for ECT [4]. Seizures exceeding 120 seconds is considered as prolonged seizure and should be terminated with intravenous benzodiazepines [5].
Anesthetics that are used for general anesthesia during ECT should have a rapid onset, rapid emergence with no interference in seizure activity. Common drugs used for ECT anesthesia are Methohexital, Thiopental, Etomidate, and Propofol. In the early days of modified ECT, barbiturates were the only choice for induction. Later other anesthetic agents have been developed. Furthermore, there has been increasing literature regarding the influence of induction agents on the therapeutic efficacy of ECT, which led psychiatrists to coordinate with the anesthesiologist in choosing the induction agent. Methohexital exerts depressant action on seizure activity and is contraindicated in patients with acute intermittent porphyria. Etomidate causes an increased incidence of emesis [6]. Similarly, the incidence of sinus bradycardia and premature ventricular contraction increased with the use of thiopental during ECT procedure [7]. For these reasons methohexital, thiopental and Etomidate are not used in current anesthetic practice for electroconvulsive therapy. Propofol as an anesthetic in ECT has favorable characteristics such as rapid onset and emergence from anesthesia, minimal postoperative confusion. However, it causes hypotension and a dose- dependent decrease in seizure duration (at dose >1mg/kg) [8].
Ketamine is also used as an anesthetic agent in ECT because it has a favorable seizure-inducing effect and increased seizure duration [9]. But it is also not devoid of disadvantages. Its main disadvantages are that it produces hypertension, delayed recovery, and precipitates psychomimetic emergence phenomena [10].
So Ketofol (1:1combination of ketamine and Propofol) can be a good alternative to either Propofol or ketamine used alone for anesthetic management for ECT. Ketamine mitigates Propofol-induced hypotension, and Propofol mitigates ketamine-induced emergence agitation [11]. Ketofol can also have a better outcome on motor seizure duration than Propofol alone. Therefore, the present study is designed to test the hypothesis that Ketofol would be a good alternative anesthetic agent than Propofol for ECT.
Material and Methods
After obtaining approval from the Institutional Review Committee (IRC) of Institute of Medicine and Nepal health research council (NHRC) the process of enrolling the eligible patients into the study was started. The trial was registered in clinical trials.gov with ID no NCT05408000. Patients between 16 to 65 years of age with American Society of Anesthesiologists (ASA) physical status I and II were included. Patients with history of epilepsy, substance abuse or dependence, any adverse reaction to study drug and pregnant women were excluded from the study. Sample size calculation was done based on the study by Yalcin, et al. [11]
considering motor seizure duration in ketofol and propofol group. Considering 80 % power with 10 % drop out rate the sample size came out to be 27 in each group.
Patients meeting the inclusion criteria were enrolled in the study. Patients were randomized into two groups: Group P (Propofol group, n=27) and Group K (Ketofol group, n=27) using computer-generated random numbers. Blinding was done by the sealed envelope technique. A pre-anesthetic checkup was conducted and a detailed history and complete physical examination were done before the procedure. Written informed consent was taken from the legal guardian of the patient.
Patients were transferred to the pre-anesthetic room. Baseline hemodynamic parameters (SBP, DBP, MAP, SPO2, and HR) were taken and recorded. An 18 G IV cannula was secured in the appropriate hand of the patient. IV infusion set was connected and one unit of Ringer’s lactate solution (500ml) was started at the rate of 100ml/hour and titrated as per requirement. The patient was premeditated with Glycopyrolate 0.2 mg 30 minutes before the procedure. Patient was transferred to the operation theatre. ECG electrodes, SPO2 probe, and Non-invasive Blood Pressure (NIBP) cuff were attached. HR, SBP, DBP, MAP, and SPO2 were continually monitored.
Preoxygenation was done via facemask at the rate of 5liter/min for 5 minutes. Anesthesia assistant prepared drugs as per randomization for each patient. The study drug was prepared by anesthesia assistant as per the instructions in the envelope. Group K- in a 10 ml syringe 5ml of ketamine (10mg/ml) and 5ml of Propofol (10mg/ml) were mixed. The study drug thus contained 5mg /ml of Propofol and 5 mg/ ml of ketamine. Group P - Propofol (10mg/ml solution) was drawn in a 10ml syringe.
Patients in Group K were administered an initial dose of 0.5mg/kg Ketofol (0.25 mg/kg of Propofol + 0.25 mg/kg of ketamine). Patients in Group P were given an initial dose of 0.5mg/kg Propofol. In both, the groups this initial dose was given within 15 seconds. Fifteen seconds after administration of the drug, the patients were assessed for unresponsiveness to verbal commands (by calling the patient’s name) & loss of eyelash reflex. Then titrated dose of the drug was given at the rate of 1ml every 5 seconds until the patients no longer responded to verbal commands and there was loss of eyelash reflex. The required total dose of the study drug was recorded.
After the loss of consciousness, hemodynamic parameters (SBP, DBP, MAP, HR & SPO2) was taken and recorded. An isolated forearm technique was performed by inflating the tourniquet 20% above the SBP in the arm where the iv cannula was not placed. Then, succinylcholine, 1 mg/kg iv was administered. Ventilation was assisted with 100 % oxygen via a face mask. Bite block was used before the application of bifrontal electrodes. Then a psychiatrist blinded to the study groups administered electrical stimuli through bifrontal electrodes. The frequency was set at 90Hz and the current was set at 800 milliamperes.
The duration of the motor seizure was defined as the time from the ECT stimulus to the cessation of tonic-clonic motor activity in the isolated arm. After the end of the seizure, the bite block was removed and ventilation was continued with 100% oxygen via face mask. The duration of motor seizures was recorded. Hemodynamic parameters (SBP, DBP, MAP, and HR) were recorded 1mins and 5 mins Propofol and Ketofol anesthesia for ECT after the end of the seizure. Esmolol 5mg iv bolus was given if SBP ≥160 mmHg and HR ≥ 120 beats per minute. Mephenteramine 6mg iv bolus was given if SBP < 90 mmHg and Atropine 0.6 mg if HR< 50 beats per minute. Midazolam 2mg iv bolus was given if the seizure duration exceeded 120 seconds.
The time from the end of succinylcholine administration to spontaneous breathing, eye-opening, and obeying commands were recorded. Once the patients were awake, obeyed commands, and maintained oxygen saturation without supplemental oxygen, they were transferred to the recovery room. Patients were monitored with ECG, pulse oximeter, and noninvasive blood pressure for one hour in the recovery room and then transferred to the ward.
Data management and analysis
Statistical analysis was done after the completion of the study. All the data analysis was performed using SPSS (Statistical Package for the Social Sciences) version 17. Continuous data is expressed as mean ± standard deviation. Independent sample t test is used to analyze interval data. P value of < 0.05 is considered as statistically significant.
Observations and results
Demography
A total of 54 ECT sessions from 8 patients were analyzed. Four patients were male and four patients were female. Five patients were between age group (20-30 years), 2 patients were between (30-40 years) and 1 patient was between (16- 20 years). Mean weight of our patients was 54.57 kg.
Comparison of motor seizure duration and recovery times
| Propofol group Mean + SD (seconds) | Ketofol group Mean + SD (seconds) | p-value¹ | |
|---|---|---|---|
| Motor seizure duration | 22.22 + 7.94 | 28.55 ± 6.54 | 0.002* |
| Time of Spontaneous breathing | 342.22 + 118.62 | 304.44 ± 111.53 | 0.233 |
| Time of spontaneous eye-opening | 593 + 123.78 | 544.44 ± 215.64 | 0.311 |
| Time of obeying commands | 720.74 + 132.48 | 735.55 ± 224.24 | 0.768 |
Table 1: Seizure duration and recovery times of patients (n=54) Comparison of hemodynamic parameters between two groups Baseline
1denotes for independent sample t-test; *denotes for statistically significant at p<0.05 Table 1: Seizure duration and recovery times of patients (n=54) Comparison of hemodynamic parameters between two groups Baseline 1denotes for independent sample t-test After induction
- 1denotes for independent sample t-test
Table 2: Hemodynamic parameters between two groups (n=54)
1 minute after end of seizure
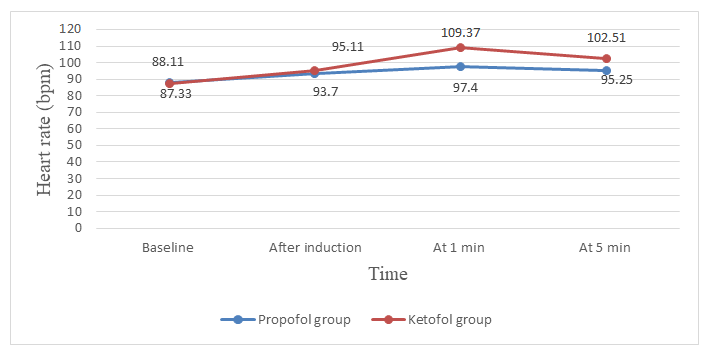
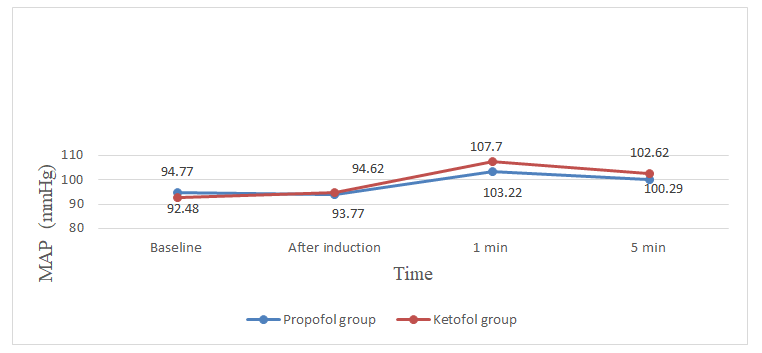
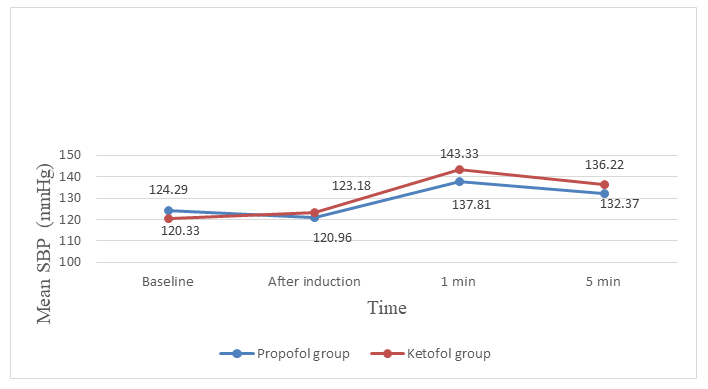
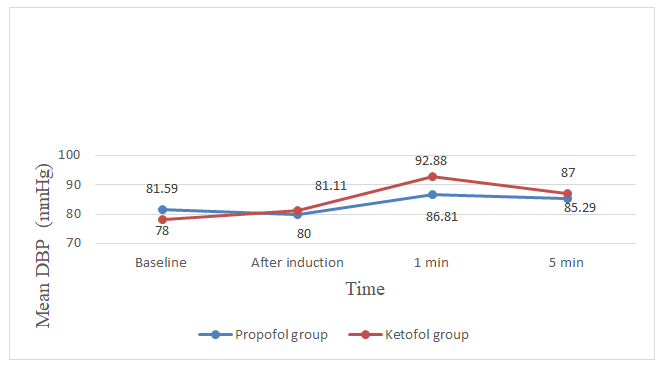
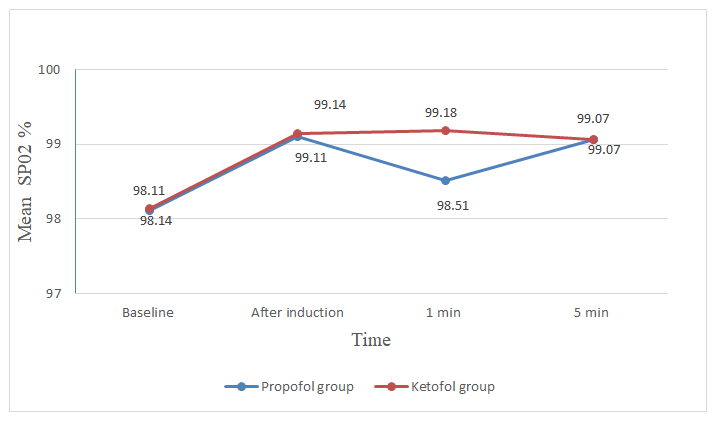
5 minutes after end of seizure Parameters Propofol group Mean + SD Ketofol group Mean + SD p-value1 Heart rate (bpm) 88.11 + 13.38 87.33 + 15.86 0.846 Systolic BP (mmHg) 124.29 + 14.83 120.33 + 15.76 0.345 Diastolic BP (mmHg) 81.59 + 14.12 78.00 + 10.31 0.291 MAP (mmHg) 94.77 + 12.98 92.48 + 11.82 0.500 SPO2 (%) 98.11 + 1.84 98.14 + 1.58 0.937 Parameters Propofol group Mean + SD Ketofol group Mean + SD p-value1 Heart rate (bpm) 93.70 + 21.83 95.11 + 17.83 0.796 Systolic BP (mmHg) 120.96 + 15.10 123.18 + 15.78 0.599 Diastolic BP (mmHg) 80.00 + 13.65 81.11 + 12.40 0.755 MAP (mmHg) 93.77 + 13.33 94.62 + 12.70 0.811 SPO2 (%) 99.11 + 1.08 99.14 + 0.95 0.894 Parameters Propofol group Mean + SD Ketofol group Mean + SD p-value1 Heart rate 97.40 + 18.18 109.37 + 17.69 0.017* Systolic BP 137.81 + 21.64 143.33 + 14.45 0.275 Diastolic BP 86.81 + 16.08 92.88 + 13.07 0.134 MAP 103.22 + 17.77 107.70 + 13.88 0.306 SPO2 98.51 + 1.52 99.18 + 0.92 0.057 Heart rate 95.25 + 10.38 102.51 + 13.65 0.032* Systolic BP 132.37 + 19.56 136.22 + 13.73 0.406 Diastolic BP 85.29 + 16.28 87.00 + 10.79 0.652 MAP 100.29 + 15.36 102.62 + 10.42 0.516 SPO2 99.07 + 0.95 99.07 + 1.07 0.500
- 1denotes for independent sample t-test; *denotes for statistically significant at p<0.05.
Table 3: Vital parameters after seizure between two groups (n=54)
Assessment of complications during the procedure
Tachycardia (HR≥ 120 bpm) was noted in 10 patients in Ketofol group out of which 5 patients were treated with injection esmolol 5mg, whereas in Propofol group 3 patients developed tachycardia (HR≥120 bpm) out of which single patient was treated with injection esmolol 5mg. A rise in systolic BP (SBP≥160 mmHg) was noted in 4 patients in the Propofol group and 1 patient in the Ketofol group. No treatment was required for rise in SBP. There was no incidence of hypotension and bradycardia in either group. There was no incidence of prolonged seizure (seizure≥ 120 seconds).
Total volume of drug required
Mean volume of Ketofol required was (9.51± 3.84 ml) and Propofol was (9.14±4.73 ml), which corresponds to the mean dose of Ketofol (95.1 ±3.84 mg) and Propofol (91.4±4.37mg).
Discussion
With the present study, we have tested the hypothesis that Ketofol increases the motor seizure duration compared to Propofol in ECT anesthesia. Propofol was used routinely in our clinical practice during ECT. Our result showed motor seizure duration in Ketofol (28.55 + 6.54 seconds) was longer compared to Propofol (22.22 + 7.94 seconds) which was statistically significant. A motor seizure lasting 20–25 seconds at minimum has been typically recommended for the therapeutic efficacy of ECT. Both Ketofol and Propofol had adequate mean motor seizure duration. The longest seizure duration was 47 seconds in the Ketofol group. A minimum seizure duration of 14 seconds and 5 seconds were present in the Propofol group in two ECT sessions of the same patient. Our study showed both drugs are equally effective with regard to motor seizure duration. Yalcin, et al. also demonstrated similar result with motor seizure duration in Ketofol (34 ± 5.8 seconds), longer than Propofol (29.3 ± 5.1 seconds) group but the duration was within therapeutic range in both groups [11]. Erdogan, et al. demonstrated motor seizure duration in Ketofol was (29±17 seconds) and Propofol (28±13 seconds) with no statistical significance between two groups but motor seizure duration was adequate in either group. So both drugs seems to be equally effective with regard to motor seizure duration. We found no statistical significance in recovery parameters (time of spontaneous breathing, time of spontaneous eye opening, time of obeying commands) in either group. Regarding hemodynamic parameters although ketofol was found to have increased heart rate compared to propofol at 1 minute after seizure but heart rate was within acceptable range (< 120). Both drugs were found to produce stable hemodynamics throughout the procedure.
Limitations
- Clinical outcomes in patients following ECT is not assessed.
- Only 8 patients are enrolled, we could have taken 1 ECT session in each patient.
Conclusion
Both Ketofol and Propofol produced adequate motor seizure duration. There was no difference in recovery parameters. Although tachycardia was noted more in Ketofol, hemodynamic stability was comparable in both groups. So, both Ketofol and Propofol can be a good choice in ECT.
Conflict of Interest
There is no conflict of interest.
References
-
Feliu M, Edwards CL, Sudhakar S, McDougald C, Raynor R, et al. (2008) Neuropsychological effects and attitudes in patients following electroconvulsive therapy. Neuropsychiatric Disease and Treatment 4(3): 613-617.
-
Erdogan Kayhan G, Yucel A, Colak YZ, Ozgul U, Yologlu S, et al. (2012) Ketofol (mixture of ketamine and propofol) administration in electroconvulsive therapy. Anaesthesia and Intensive Care. 40(2): 305-310.
-
Joo SW, Joo YH, Kim CY, Lee JS (2017) Effects of stimulus parameters on motor seizure duration in electroconvulsive therapy. Neuropsychiatric Disease and Treatment 13: 1427-1434.
-
Sarkhel S (2009) Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry (10th edn), Indian Journal of Psychiatry 51(4): 331.
-
Sciences N (1997) Prolonged Seizures during Electroconvulsive Therapy. 68.
-
Chawla N (2020) Anesthesia for Electroconvulsive Therapy. Anesthesiology Clinics. Published online 2020.
-
Mokriski BK, Nagle SE, Papuchis GC, Cohen SM, Waxman GJ (1992) Electroconvulsive therapy-induced cardiac arrhythmias during anesthesia with methohexital, thiamylal, or thiopental sodium. J Clin Anesth 4(3): 208- 212.
-
Aytuluk HG, Simsek T, Yilmaz M, Turan AZ, Saracoglu KT (2019) Can propofol lead to an increase in seizure threshold over the course of electroconvulsive therapy? Clinical Psychopharmacology and Neuroscience. 17(4): 523-530.
-
Kurdi M, Theerth K, Deva R (2014) Ketamine: Current applications in anesthesia, pain, and critical care. Anesthesia: Essays and Researches 8(3): 283.
-
Gamble JJ, Bi H, Bowen R, Weisgerber G, Sanjanwala R, et al. (2018) Ketamine-based anesthesia improves electroconvulsive therapy outcomes: a randomized- controlled study. Canadian Journal of Anesthesia 65(6): 636-646.
-
Yalcin S, Aydogan H, Selek S, Kucuk A, Yuce HH, et al. (2012) Ketofol in electroconvulsive therapy anesthesia: Two stones for one bird. Journal of Anesthesia 26(4): 562-567.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index