Anaesthesia Management of a Parturient with Klippel Feil Syndrome Undergoing Emergency Cesarean Section
Klippel Feil syndrome (KFS) is a rare autosomal genetic disorder comprising of classical triad of short neck, low hairline, and limited neck mobility. Parturient with KFS syndrome presents with difficult airway and needs individualized consideration for Anaesthesia. Management with Regional Anaesthesia has its pros and cons and can be considered in parturient with KFS as General Anaesthesia in pregnancy poses increased risk of aspiration, difficult mask ventilation and endotracheal intubation. We present a case of a 25-yr old parturient G3A2 with 34+4 weeks of gestation with KFS syndrome posted for emergency caesarean section managed successfully under spinal anaesthesia.
Introduction
Maurice Klippel and Feil first described Klippel Feil syndrome (KFS) in 1912 as a congenital malformation causing fusion of cervical vertebrae which can involve either two vertebrae or entire cervical spine [1]. Klippel-Feil syndrome (KFS) is a congenital anomaly characterized by clinical triad consisting of short neck, low posterior hairline, and limited neck movement, although less than 50% of patients demonstrate all 3 clinical features [2]. Anaesthesia management of parturient with KFS syndrome is challenging considering difficult airway due to limited or no neck movement resulting from cervical fusion. Administration of both General and Regional Anaesthesia can be difficult due to cervical involvement and other associated anomalies like scoliosis.
Case Report
We present a case of a 25-year-old parturient, G3A2
with 34+4 weeks of gestation, with IUGR with mild oligohydramnios presented for emergency caesarean section in view of non-reassuring Non stress test and absent diastolic flow. She was a diagnosed case of Kippel Feil syndrome Type 2 with a Sprengel deformity of right shoulder since birth. She has h/o Hypothyroidism since second trimester of pregnancy and was on regular treatment with normal thyroid function test. She had a surgical history of modified Woodward procedure for Sprengel deformity correction in childhood. On examination parturient was averagely built, weighing 59kgs with BMI of 25.5kg/m2. She presented with classical triad of short neck, low posterior hairline, and limited range of neck movements (Figure 1). The abduction of her right hand was restricted up to an angle of 45 degree. She was unable to lift her right hand over the shoulder since birth. Spine examination showed a prominent S shaped Scoliotic deformity of the cervico- thoracic region with a scar mark of the previous surgery over the upper back with normal lumbar spaces on palpation. No neurological deficit detected.

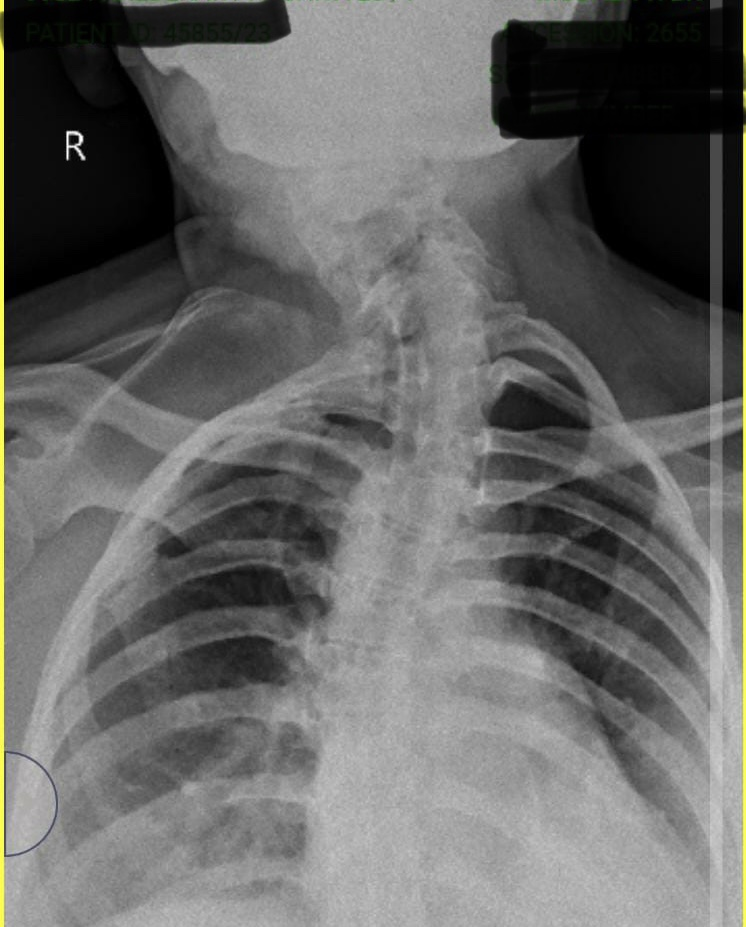
Airway assessment showed limited flexion and extension of the neck. Her mouth opening was adequate with Mallampati class II, no micrognathia noted. Systemic examination and blood investigations were normal. No other associated congenital disorder detected. Old investigations reports revealed deformed upper ribs with partial fusion at posterior aspects on right side associated with cervical vertebral anomalies seen. CT scan of lower cervical and upper thoracic region was suggestive of Congenital anomalies (Sprengel’s deformity) in the scapula and the cervico-thoracic spine. S shaped rotatory scoliosis with a convexity to right noted. Upper dorsal vertebrae from T1 to T4 vertebrae were deformed (hemivertebrae). C6-C7 vertebra appears fused with a rudimentary disc in between them. 1st rib on right side was not visualised. 3rd and 4th rib appear fused with wedging of the D3 and D4 hemi vertebral bodies on the right side. There was right sided elevated and rotated scapula. No spina bifida noted. The spinal canal dimensions were normal. No anomaly seen on Left side of thorax. ECG and 2D Echo done previously was normal. To determine the exact deformity of the spine and airway assessment, we did Xray neck AP and lateral post operatively which suggested tracheal deviation to left with no narrowing of airway (Figures 2 & 3).
The parturient was posted for Emergency LSCS, detailed clinical, physical examination with airway assessment was done in preoperative room. After detailed evaluation our Plan A of Anaesthesia was Spinal Anaesthesia. Plan B was Awake Fiberoptic intubation for providing General Anaesthesia. Operating Theatre preparation was done with all standard monitors, warming equipment, and emergency drugs. Difficult airway cart with Fiber-optic bronchoscope and emergency tracheostomy set was kept ready. Premedication in form of Inj Pantoprazole 1gm iv and Inj Metoclopramide 10 mg iv was given preoperatively as aspiration prophylaxis.

After informed written consent and adequate NBM status was confirmed, the parturient was shifted inside the OT in left lateral position. ASA standard monitors including ECG, NIBP, SpO2 Probe were attached. Her vitals were pulse rate - 82/ min, blood pressure - 130/70 mmHg and oxygen saturation on room air- 99%. IV access with 18 G intra catheter was taken and preloading with RL (15ml/kg) started.
Under all septic conditions, Subarachnoid block was performed by senior anaesthesiologist using 26 gauze Quincke’s spinal needle at L3-L4 space and Inj. Bupivacaine heavy 0.5% 1.8CC with Inj. Fentanyl 10mcg was given. Parturient was made supine and wedge given under right hip. The level of spinal anaesthesia was checked by pin prick sensation. T6 level was achieved. Surgery was started and baby was delivered with APGAR score 7. The surgery completed uneventfully under Spinal Anaesthesia. Parturient was vigilantly monitored postoperatively. After adequate recovery, parturient was shifted to the postnatal ward and discharged after 5 days uneventfully.
Discussion
Klippel–Feil syndrome is an inherited disorder with an estimated incidence of 1:40 000 births with female predominance (60% of cases). This congenital vertebral fusion of the cervical spine results from failure of segmentation of cervical somites during the organogenesis between first 3 to 8 weeks of gestation. Traditionally KFS has been classified into 3 types based on the degree of involvement as type I (massive fusion of cervical and upper thoracic vertebrae), type II (fusion of 2 or more vertebrae with associated atlanto-occipital assimilation, hemivertebrae, or any other anomaly of the cervical spine), and type III (fused cervical vertebrae with lower thoracic or lumbar vertebrae) [3]. Radiographically, Type I was defined as having a single congenitally fused cervical segment. Type II includes multiple non-contiguous, congenitally fused segments, and Type III includes multiple contiguous, congenitally fused cervical segments [4].
KFS may be associated with other congenital anomalies like scoliosis (60% of cases), spina bifida occulta (45%), renal abnormalities (35–55%), rib deformity (20–30%), deafness (30– 40%), synkinesia (20%), congenital heart disease (8–14%) and Sprengel anomaly, which occurs in 20–30% of the patients. Neck movements restrictions due to absent or fused cervical segments along with associated congenital anomalies like hypoplasia of the maxillary or mandibular region, torticollis, and cleft lip and/or palate makes management of airway difficult [5, 6]. These anomalies result in difficult mask ventilation and difficult intubation. Due to cervical instability, during mask ventilation and direct laryngoscopy inline cervical stabilization should be maintained and any cervical manipulation should be avoided to prevent any myelopathy or neurological sequel.
Awake Fiberoptic intubation is considered as the gold standard in managing difficult airway in KFS parturient undergoing caesarean section under General Anaesthesia [7]. However regional anaesthesia can be considered as an alternative as it avoids handling of airway in KFS where both mask ventilation and endotracheal intubation can be challenging due to cervical fusion and instability.
In our case mouth opening was adequate with MPC 2 with limited neck movement. We made decision of proceeding with spinal anaesthesia with all preparation to handle difficult airway. In pregnancy regional Anaesthesia is preferred as it avoids general Anaesthesia which poses risk of aspiration, rapid desaturation, difficult mask ventilation and endotracheal intubation. At the same time when opting for regional Anaesthesia, chances of failure or inadequate Anaesthesia with less time to convert to General Anaesthesia, high spinal due to scoliosis should be kept in mind. We added fentanyl as an adjuvant to Bupivacaine to prolong the effect of spinal Anaesthesia in view of chances of prolongation of surgery.
Ahuja V, et al. [8] in an interesting case report managed the airway of KFS posted for corrective surgery for Sprengel’s shoulder under general anaesthesia with Glidescope. Authors have selected this technique as an alternative to Awake fiberoptic intubation as mouth opening was adequate and no neck mobility is required while using Glidescope. In our case we have kept fiberoptic bronchoscope with tracheostomy set stand by as a part of difficult airway cart. Sharma BL, et al. [9] presented a case of parturient with KFS and difficult airway posted for emergency Caesarean Section. They planned and successfully managed LSCS under regional anaesthesia.
Hsu G, et al. [10] presented a case report of 38-year-old primiparous woman with type III Klippel-Feil syndrome posted for elective caesarean delivery. They planned a combined spinal-epidural technique; however, spinal anaesthesia failed and only the epidural technique was obtained. LSCS was managed successfully under regional anaesthesia with favourable maternal and fetal outcomes.
Parturient with Klippel -Feil syndrome poses unique challenge to anaesthesiologist as it is rare entity which involve management of difficult airway along with other congenital disorder like scoliosis, Sprengel deformity etc. Decision making on proceeding with regional or general anaesthesia should be individualised based on investigations, airway assessment and availability of Airway gadgets along with expertise and skills of anaesthesiologist. We were able to successfully manage parturient with KFS under regional anaesthesia with good maternal and fetal outcome.
Conclusion
We recommend early involvement of an anesthesiologist during antenatal checkup and detailed investigations for assessment of airway and associated congenital disorder which will help in safe delivery in parturient with KFS during emergency surgery. We conclude that successful Anaesthesia management of syndromic patients with KFS needs detailed preoperative assessment for associated congenital disorder and planning with expertise for handling anticipated difficult airway.
Conflicts of Interest
None
Acknowledgements
None
Funding
None
References
-
Klippel M, Feil A (1975) The classic: A Case of Absence of Cervical Vertebrae with the Thoracic Cage Rising to the Base of the Cranium (Cervical Thoracic Cage). Clin Orthop Relat Res 109: 3-8.
-
Bejiqi R, Retkoceri R, Bejiqi H, Zeka N (2015) Klippel - Feil Syndrome Associated with Congential Heart Disease Presentaion of Cases and a Review of the Curent Literature. Open Access Maced J Med Sci 3(1): 129-134.
-
Klimo P Jr, Rao G, Brockmeyer D (2007) Congenital anomalies of the cervical spine. Neurosurg Clin N Am 18(3): 463-478.
-
Samartzis DD, Herman J, Lubicky JP, Shen FH (2006) Classification of congenitally fused cervical patterns in Klippel-Feil patients: epidemiology and role in the development of cervical spine-related symptoms. Spine (Phila Pa 1976) 31(21): E798-804.
-
Frikha R (2020) Klippel-Feil syndrome: a review of the literature. Clinical Dysmorphology 29(1): 35-37.
-
Hensinger RN, Lang JE, MacEwen GD (1974) Klippel-Feil syndrome; a constellation of associated anomalies. Journal of Bone and Joint Surgery, American Volume 56(6): 1246-1253.
-
Venkata MKK, Khan JA, Qureshi MT, Qureshi A, Kar I, et al. (2009) Anaesthetic management of a patient with Klippel-Feil syndrome for elective Caesarean section. British Journal Med Pract 2(3): 54-56.
-
Ahuja V, Kazal S, Gombar S, Thapa D, Bahadur R, et al. (2012) Glidescope (®) for predicted difficult airway in Klippel-Feil Syndrome. J Anaesthesiol Clin Pharmacol 28(4): 532-534.
-
Sharma BL, Sushil B, Chatterjee CS, Smridhi N (2016) Anaesthetic Management for Emergency Caesarean Section in a Parturient with Klippel Feil Syndrome. J Anesth Clin Res 7: 12.
-
Hsu G, Manabat E, Huffnagle S, Huffnagle HJ (2011) Anesthetic management of a parturient with type III Klippel-Feil syndrome. Int J Obstet Anesth 20(1): 82-85.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index