Rapid Evaluation of Cardiovascular Phenotypes in Hemodynamic Instability Due to Septic Shock and its Association with Outcomes
Background and aim: Septic shock is characterized as a life-threatening organ failure resulting from an aberrant host response to infection. Sepsis continues to be the primary cause of mortality in severely ill patients. Sepsis mortality is associated with cardiac dysfunction. This study aims to assess cardiovascular phenotypes in hemodynamic instability resulting from septic shock and their correlation with outcomes. Methods: Analytic-observational cohort research was performed in the Intensive Care Units at Qasr El Eni Hospital and Maadi Hospitals involving 53 persons diagnosed with septic shock. The study lasted six months, from June 1, 2022, to January 30, 2023. Results: The three biomarkers (left ventricular ejection fraction, left ventricular fractional area change, and mitral E wave velocity in cm/s) were independent predictors for cluster 2. The area under the ROC curve for the combination of these three parameters was 0.983. The predictive capacity of combined indicators demonstrated superiority compared to the single measure (P < 0.001). Univariate analysis indicated that the three biomarkers (left ventricular ejection fraction, mitral E wave velocity in cm/s, and right ventricular/left ventricular end-diastolic area) were independent predictors for cluster 4. The amalgamation of these three traits produced a ROC area of 0.836. The predictive efficacy of aggregated indicators surpassed that of an individual index (P=0.001). Conclusion: The examination of various clusters according to shock type and the presence or absence of left ventricular (LV) systolic dysfunction, hyperkinetic profile, right ventricular (RV) failure and persistent hypovolemia demonstrated notable disparities in laboratory and hemodynamic parameters, with LV systolic dysfunction correlating with diminished ScvO2 levels and RV failure linked to elevated central venous pressure. The echocardiographic measurements revealed considerable disparities among the clusters, with patients exhibiting left ventricular systolic dysfunction demonstrating reduced left ventricular ejection fraction, left ventricular fractional area change, and mitral E wave velocity. This study offers significant insights into the clinical profiles and related characteristics of septic shock patients, facilitating the formulation of focused treatment regimens.
Abbreviations
SSC: Surviving Sepsis Campaign; LV: Left Ventricular; RV: Right Ventricular; LVEF: Left Ventricular Ejection Fraction; FAC: Left Ventricular Fractional Area Change; EDA: End Diastolic Area; CI: Cardiac Index; SAP: Systolic Arterial Pressure; DAP: Diastolic Arterial Pressure; MAP: Mean Arterial Pressure; CVP: Central Venous Pressure.
Introduction
Septic shock is characterized as a life-threatening organ failure resulting from a dysregulated host response to infection. Sepsis continues to be the primary cause of mortality in critically sick patients, notwithstanding therapeutic advancements [1, 2]. Timely identification of sepsis and subsequent treatment interventions, as per the Surviving Sepsis Campaign (SSC) guidelines, are essential for enhancing survival rates [3, 4]. Sepsis mortality is associated with cardiac dysfunction [5].
Echocardiographic studies have confirmed a significant prevalence of early myocardial alterations, with one study reporting a 39 percent incidence of left ventricular systolic dysfunction on the first day [6]. The categorization of hemodynamics in septic shock into five cardiovascular phenotypes (left ventricular systolic dysfunction, left ventricular hyperkinesia, persistent hypovolemia, right ventricular failure, and well-resuscitated phenotype) has been suggested by nine researchers to facilitate targeted and personalized therapy for hemodynamic support and to predict mortality in septic shock [7]. We predicted that employing a clustering strategy in septic shock patients monitored via transthoracic echocardiography could enhance the characterization of distinct cardiovascular characteristics to predict outcomes.
Patients and Methods
Study Design and Patient Criteria
This Analytic Observational Cohort study was conducted in the Intensive Care Units, Qasr El Eni Hospital, and Maadi Hospitals on 53 adults diagnosed with septic shock. The duration of the study was 6 months during the period from March 2022 to December 2023.
Patients’ Criteria
We included all adult patients diagnosed with septic shock that continues despite sufficient fluid resuscitation and vasopressor administration. However, pregnant women and individuals with terminal malignancies were excluded.
Operational Design
All the patients were subjected to: Initial assessment encompassing personal history, complaints, prior surgical interventions, blood transfusion history, chronic disease history, and medically significant habits such as smoking, along with SOFA, SAPS II, and blood lactate levels.
General examination including vital signs, indicators of pallor such as cyanosis and jaundice, lymphadenopathy, cutaneous evaluation for cyanosis, pharyngeal examination for lymphadenopathy, extremity assessment for diminished peripheral pulses, and neurological evaluation for altered sensorium, lethargy, and coma.
Procedures
Calculate the sequential organ failure assessment (SOFA) score and the simplified acute physiology score (SAPS II) upon admission and on day 7 of admission.
Simplified Acute Physiology Score (SAPS II)
The point score was derived from 12 physiological variables and 3 disease-related variables within the initial 24 hours, along with data regarding prior health status and certain information collected at admission.
The parameters were age, heart rate, systolic blood pressure, temperature, Glasgow Coma Scale, mechanical ventilation or CPAP, PaO2, FiO2, urine output, blood urea nitrogen, sodium, potassium, bicarbonate, bilirubin, white blood cell count, chronic illnesses, and type of admission. Additionally, transthoracic echocardiography was performed to assess all patients and categorize them into five clusters within the first 24 hours following the diagnosis of septic shock, after initial fluid resuscitation and vasopressor administration.
Assessment of left ventricular (LV) systolic function parameters, specifically left ventricular ejection fraction (LVEF) and left ventricular fractional area change (FAC), as well as left ventricular diastolic function parameters, namely maximal mitral Doppler E wave velocity and maximal tissue Doppler velocity of the lateral mitral annulus during early diastole (E′). The right ventricular function is assessed using the ratio of right ventricular to left ventricular end-diastolic area (EDA). Assessment of fluid responsiveness via the inferior vena cava collapsibility index (ΔIVC). Assessment of the velocity time integral (VTI) in the left ventricular outflow tract and the diameter of the aortic annulus to compute left ventricular stroke volume and cardiac index (CI).
Septic shock Patients were categorized into five cardiovascular phenotypes based on echocardiographic measurements: Cluster I: left ventricular (LV) systolic dysfunction absent right ventricular (RV) failure or fluid responsiveness. Cluster II: Left ventricular hyperkinesia absent left ventricular systolic dysfunction, right ventricular failure, or fluid responsiveness. Cluster III: persistent hypovolemia accompanied by left ventricular (LV) systolic function preservation and right ventricular (RV) failure. Cluster IV: right ventricular failure without left ventricular (LV) systolic dysfunction or fluid responsiveness. Cluster V: well resuscitated, with no left ventricular (LV) systolic dysfunction, right ventricular (RV) failure, while demonstrating fluid responsiveness.
In each patient, multiple clinical hemodynamic parameters were prospectively documented at the time of the transthoracic echocardiogram (TTE): heart rate, non- invasive systolic arterial pressure (SAP), diastolic arterial pressure (DAP), mean arterial pressure (MAP), central venous pressure (CVP), serum lactate concentration, and the presence and respective dosages of epinephrine, dobutamine, or norepinephrine. Arterial and central venous blood gas analyses, along with respiratory ventilator settings when relevant, were documented.
The Outcome of the Study
On day 7 and day 30, all mortality cases were documented.
Ethics Approval and Consent to Participate
Official authorization was secured from the Faculty of Medicine, Qasr El Eni University. Official authorization was secured from Qasr El Eni Hospital and Armed Forces Hospitals. Authorization from the ethics committee within the faculty of medicine. Informed written consent was obtained from each patient prior to their inclusion in this study. No participant was obligated to partake in this research if they choose not to. They may withdraw from participation at any moment.
Statistical Analysis
The collected data were encoded, organized, and subjected to statistical analysis utilizing IBM SPSS Statistics software version 28.0 (IBM Corp., Chicago, USA, 2021). Quantitative data underwent normality assessment via the Shapiro-Wilk test, then described as mean ± SD (standard deviation), alongside the minimum and maximum values of the range, and contrasted utilizing an independent t-test. Qualitative data is represented by numbers and percentages and analyzed using the Chi-square test and Fisher’s Exact test for variables with modest predicted frequencies. A binary logistic regression analysis was conducted to evaluate the impact of hemodynamic parameters. The significance level was established at a p-value of <0.050.
Results
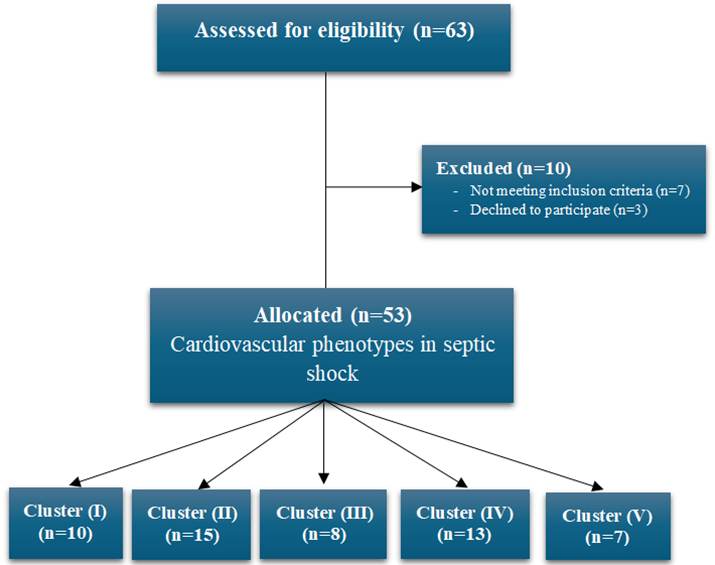
Figure 1 illustrates a flowchart of the research population. Sixty-three patients were evaluated to examine the effects of early cardiovascular phenotypic evaluation in septic shock and its link with outcomes in the Intensive Care Units of Qasr El Eni Hospital and Maadi Hospitals. Ten subjects were excluded from the study (three patients declined consent, and seven patients did not meet the inclusion criteria). Fifty- three patients consented to participate and were allocated into five groups: Cluster I (n=10), Cluster II (n=15), Cluster III (n=8), Cluster IV (n=13), and Cluster V (n=7) (Figure 1).
The average age of patients in Cluster II (LV hyperkinetic profile) was the greatest at 64.20 ±6.41, whereas Cluster III (persistent hypovolemia) had the lowest average age at 59.60 ±9.74. Nonetheless, there was no notable age disparity among the clusters (P=0.667). The mean BMI was greatest in Cluster II (34.40 ±6.64) and least in Cluster V (well resuscitated) (31.86 ±7.77), although no significant variation in BMI was observed among the clusters (P=0.591). Regarding sex distribution, Cluster I (LV systolic dysfunction) comprised only male patients (100%), followed by Cluster III (75%), Cluster II (53.3%), and the lowest in Cluster IV (RV failure) (42.9%), but the difference was not statistically significant (P=0.068). The prevalence of individuals with a smoking history was substantially greater in Cluster I (70.0%) than in the other groups (P=0.012). The prevalence of COPD patients was markedly greater in Cluster I (50.0%) than in the other clusters (P=0.001). The prevalence of individuals with IHD was markedly greater in Cluster I (60.0%) and Cluster V (38.5%) relative to the other clusters (P=0.036). Nonetheless, there was no notable difference in the prevalence of patients with diabetes mellitus and hypertension across the clusters (Table 1).
| Cluster (I) (n=10) | Cluster | P value | ||||||
|---|---|---|---|---|---|---|---|---|
| Total (n=53) | Cluster (II) (n=15) | Cluster (III) (n=8) | Cluster (IV) (n=13) | Cluster (V) (n=7) | ||||
| Age (years), Mean ± SD. | 61.43 ±7.64 | 64.20 ±6.41 | 59.60 ±9.74 | 63.00 ±7.25 | 61.54 ±5.50 | 59.43 ±8.46 | 0.667 | |
| BMI (kg/m2), Mean ± SD. | 32.06 ±6.61 | 34.40 ±6.64 | 31.78 ±6.98 | 32.75 ±5.90 | 30.07 ±6.32 | 31.86 ±7.77 | 0.591 | |
| Sex n (%) | Male | 34 (64.2%) | 10 (100.0%) | 8 (53.3%) | 6 (75.0%) | 7 (53.8%) | 3 (42.9%) | 0.068 |
| Female | 19 (35.8%) | 0 (0.0%) | 7 (46.7%) | 2 (25.0%) | 6 (46.2%) | 4 (57.1%) | ||
| Smoking | 16 (30.2%) | 7 (70.0%) | 1 (6.7%) | 2 (25.0%) | 3 (23.1%) | 3 (42.9%) | 0.012* | |
| DM | 13 (24.5% | 4 (40.0%) | 3 (20.0%) | 1 (12.5%) | 3 (23.1%) | 2 (28.6%) | 0.732 | |
| HTN | 15 (28.3%) | 5 (50.0%) | 3 (20.0%) | 2 (25.0%) | 3 (23.1%) | 2 (28.6%) | 0.531 | |
| COPD | 6 (11.3%) | 5 (50.0%) | 0 (0.0%) | 1 (12.5%) | 0 (0.0%) | 0 (0.0%) | 0.001* | |
| IHD | 15 (28.3%) | 6 (60.0%) | 1 (6.7%) | 1 (12.5%) | 5 (38.5%) | 2 (28.6%) | 0.036* |
Table 1: Demographic and comorbidities data in the study according to the cluster partition.
The laboratory and scores data of the study based on the cluster partition. The investigated variables comprise the cluster number (I-V) and the mean values with standard deviation (SD) of the SOFA score, SAPSII, hemoglobin (Hb), hematocrit (HCT), albumin, creatinine, lactate (mmol/l), and potassium (K) level for each cluster. There are notable disparities in SOFA scores among clusters (p=0.005). Cluster II (patients exhibiting a hyperkinetic left ventricular profile) demonstrated the lowest average SOFA score relative to other clusters. Cluster I (patients exhibiting left ventricular systolic dysfunction) recorded the highest mean SOFA score (10.70). There are notable disparities in SAPSII scores among clusters (p=0.011), with Cluster II exhibiting the lowest mean score (52.40) and Cluster I am presenting the highest (64.90). Patients in Cluster V, who received adequate resuscitation, exhibited the lowest mean creatinine level (0.79). No substantial changes were seen in Hb, albumin, lactate mmol/l, and K levels between the clusters (Table 2).
| Variables | Total (n=53) Mean ± SD. | Cluster | P value | ||||
|---|---|---|---|---|---|---|---|
| Cluster (I) (n=10) Mean ± SD | Cluster (II) (n=15) Mean ± SD | Cluster (III) (n=8) Mean ± SD | Cluster (IV) (n=13) Mean ± SD | Cluster (V) (n=7) Mean ± SD | |||
| Sofa score | 9.19 ±1.46 | 10.70 ±1.25 | 8.73 ±1.33 | 9.13 ±1.89 | 8.62 ±0.96 | 9.14 ±0.90 | 0.005* |
| SAPSII | 55.26 ±8.84 | 64.90 ±7.28 | 52.40 ±8.01 | 54.75 ±11.31 | 51.69 ±5.76 | 54.86 ±5.40 | 0.011* |
| Hb | 13.26 ±1.70 | 13.09 ±1.75 | 13.07 ±1.88 | 12.50 ±1.31 | 13.54 ±1.51 | 14.30 ±1.78 | 0.273 |
| HCT | 40.04 ±3.40 | 37.81 ±4.91 | 40.73 ±2.52 | 37.96 ±3.71 | 40.85 ±1.74 | 42.61 ±1.73 | 0.013* |
| Albumin | 3.95 ±0.44 | 3.88 ±0.46 | 3.93 ±0.45 | 4.19 ±0.18 | 3.83 ±0.45 | 4.03 ±0.53 | 0.441 |
| Creatinine | 1.00 ±0.35 | 1.09 ±0.36 | 0.92 ±0.36 | 1.26 ±0.29 | 0.96 ±0.37 | 0.79 ±0.15 | 0.026* |
| Lactate mmol/l | 3.34 ±1.13 | 4.09 ±1.11 | 2.96 ±1.00 | 3.78 ±1.78 | 2.96 ±0.67 | 3.29 ±0.61 | 0.113 |
| K level | 3.74 ±0.66 | 4.01 ±0.76 | 3.71 ±0.66 | 3.60 ±0.95 | 3.82 ±0.40 | 3.44 ±0.49 | 0.315 |
Table 2: Laboratory and scores data in the study according to the cluster partition.
Additionally, Cluster II, comprising patients with a left ventricular hyperkinetic profile, exhibited the highest left ventricular ejection fraction (EF) and left ventricular fractional area change (LVFAC), alongside the highest mitral E wave velocity, E′ wave velocity, aortic velocity time integral (VTI), and change in superior vena cava (∆SVC). Cluster IV (patients with right ventricular failure) exhibited the largest E/E′ ratio and right ventricular/left ventricular end- diastolic area (EDA). Patients in Cluster I with left ventricular systolic dysfunction exhibited a markedly reduced mean left ventricular ejection fraction (38.50±5.93) and left ventricular fractional area change (37.30±5.56), alongside diminished values for additional echocardiographic parameters, including mitral E wave (57.90±8.40), mitral E′ wave (7.48±1.10), aortic VTI (12.48±1.10), and ∆SVC (10.48±1.10), (Table 3).
| Variables | Total (n=53) Mean ± SD | Cluster | P value | ||||
|---|---|---|---|---|---|---|---|
| Cluster (I) (n=10) Mean ± SD | Cluster (II) (n=15) Mean ± SD | Cluster (III) (n=8) Mean ± SD | Cluster (IV) (n=13) Mean ± SD | Cluster (V) (n=7) Mean ± SD | |||
| Lt vent EF | 56.70 ±9.19 | 38.50 ±5.93 | 59.73 ±7.28 | 56.12 ±4.42 | 63.38 ±4.68 | 58.71 ±5.28 | <0.001* |
| LVFAC | 47.98 ±7.93 | 37.30 ±5.56 | 50.80 ±5.92 | 49.13 ±7.99 | 51.62 ±5.01 | 49.14 ±7.13 | 0.001* |
| Mitral E wave, cm/s | 69.98 ±10.31 | 57.90 ±8.40 | 69.87 ±8.73 | 70.63 ±9.78 | 75.62 ±7.14 | 76.29 ±8.08 | 0.001* |
| Mitral E′ wave, cm/s | 9.59 ±1.58 | 7.48 ±1.10 | 10.15 ±1.20 | 9.83 ±1.60 | 10.29 ±1.04 | 9.83 ±1.43 | 0.001* |
| E/E′ ratio | 7.25 ±1.47 | 5.48 ±1.10 | 7.41 ±1.20 | 7.57 ±1.43 | 8.06 ±1.04 | 7.54 ±1.40 | 0.002* |
| Aortic VTI, cm | 14.32 ±1.46 | 12.48 ±1.10 | 14.47 ±1.20 | 14.58 ±1.43 | 15.14 ±0.90 | 14.81 ±1.35 | 0.001* |
| RV/LV EDA | 0.69 ±0.17 | 0.53 ±0.13 | 0.67 ±0.21 | 0.73 ±0.12 | 0.79 ±0.09 | 0.72 ±0.13 | 0.002* |
| ∆SVC, % | 13.36 ±3.19 | 10.48 ±1.10 | 14.15 ±3.73 | 13.15 ±2.11 | 14.25 ±3.19 | 14.40 ±3.12 | 0.002* |
Table 3: Echocardiographic parameters in the study according to the cluster partition.
Among the 53 patients, 5.7% were administered epinephrine infusion, 35.8% were given norepinephrine, and 7.5% received dobutamine. The proportion of patients receiving each treatment differed among the various clusters. No statistically significant differences were observed in the administration of norepinephrine or dobutamine across the various clusters; however, a trend indicated increased utilization of epinephrine in cluster I (patients with left ventricular systolic dysfunction) relative to the other clusters, although this difference did not achieve statistical significance (Table 4).
| Variables | Total (n=53) | Cluster | P value | ||||
|---|---|---|---|---|---|---|---|
| Cluster (I) (n=10) | Cluster (II) (n=15) | Cluster (III) (n=8) | Cluster (IV) (n=13) | Cluster (V) (n=7) | |||
| Epinephrine infusion | 3 (5.7%) | 2 (20.0%) | 0 (0.0%) | 1 (12.5%) | 0 (0.0%) | 0 (0.0%) | 0.164 |
| Norepinephrine | 19 (35.8%) | 5 (50.0%) | 7 (46.7%) | 1 (12.5%) | 4 (30.8%) | 2 (28.6%) | 0.442 |
| Dobutamine | 4 (7.5%) | 2 (20.0%) | 1 (6.7%) | 1 (12.5%) | 0 (0.0%) | 0 (0.0%) | 0.406 |
Table 4: Hemodynamic treatments in the study according to the cluster partition.
Univariable analysis identified the three biomarkers (Lt Vent EF, LVFAC, and Mitral E wave, cm/s) as independent predictors for cluster 2. The area under the ROC curve for the combination of these three parameters was 0.983. The predictive capacity of combined indicators shown superiority compared to the single measure (P < 0.001), (Figure 2).

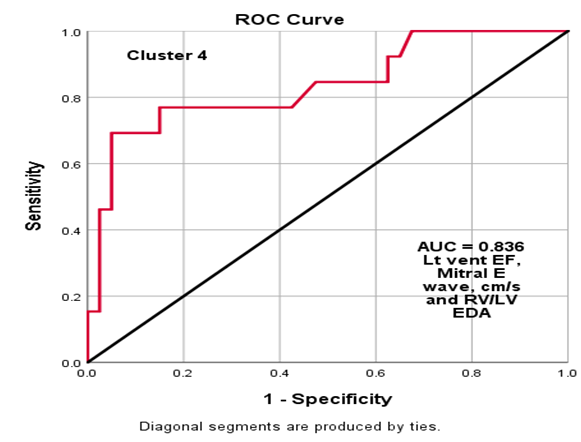
Also, Univariate analysis indicated that the three biomarkers (left ventricular ejection fraction, mitral E wave velocity in cm/s, and right ventricular to left ventricular end- diastolic area ratio) were independent predictors for cluster
4. The amalgamation of these three attributes produced a ROC area of 0.836. The predictive efficacy of aggregated indicators surpassed that of an individual index (P=0.001), (Figure 3).
The study’s outcome was assessed based on cluster division, revealing a significant difference in the 30-day mortality rate across the five clusters (p=0.042). The highest mortality rate was recorded in Cluster (I) LV systolic
- dysfunction (60.0%), followed by Cluster (IV) RV failure
- (38.50%). No mortality was found in patients from Cluster
- (V) who received adequate resuscitation (Table 5). p: p value for comparing between the two studied groups *: Statistically significant at p ≤ 0.05
- In Cluster I, a greater percentage of individuals with diabetes mellitus (75%) and hypertension (60%) encountered death. In Cluster II, every patient with ischemic heart disease (IHD) encountered mortality. In Cluster IV, a
- Cluster (I) patients with
- LV systolic dysfunction
- Mortality (n=6)
- Cluster (II) patients with LV hyperkinetic profile
- Mortality (n=2)
- Cluster (III) patients with persistent hypovolemia
- Mortality (n=2)
- Age
- 67.33 ± 3.7
- 71.00 ± 2.8
- 70.00 ± 1.4
- 67.00 ± 1.6
- Sex (male)
- 6 (60%)
- 0 (0%)
- 2 (33.3)
- 4 (57.1%)
- 0 (0%)
- Smoking
- 4 (57.1%)
- 0 (0%)
- 1 (50%)
- 0 (0%)
- 0 (0%)
- DM
- 3 (75%)
- 1 (33.3)
- 0 (0%)
- 0 (0%)
- 0 (0%)
- HTN
- 3 (60%)
- 0 (0%)
- 0 (0%)
- 1 (33.3%)
- 0 (0%)
- IHD
- 2 (100%)
- 2 (66.7%)
- 1 (33.3%)
- 1 (20%)
- 0 (0%)
Table 5: Associated risk factor with mortality in different clusters.
| Variables | Total (n=53) | Cluster | P value | ||||
|---|---|---|---|---|---|---|---|
| Cluster (I) (n=10) | Cluster (II) (n=15) | Cluster (III) (n=8) | Cluster (IV) (n=13) | Cluster (V) (n=7) | |||
| 30-day mortality | 15 (28.3) | 6 (60.0%) | 2 (13.2%) | 2 (25.0%) | 5 (38.5%) | 0 (0.0%) | 0.032* |
Table 6: Associated risk factor with mortality in different clusters.
greater percentage of male patients (57.1%) and individuals with a smoking history (57.1%) encountered mortality (Table 6).
Cluster (IV) patients with RV failure Mortality (n=5) Cluster (V) patients well resuscitated mortality(n=0) Table 6: Associated risk factor with mortality in different clusters.
The findings demonstrate that age and male gender were strongly correlated with mortality in both univariate and multivariate analyses. In the univariate study, a one- year increase in age corresponded to a 38.2% rise in death risks, while the multivariate analysis indicated a 51.4% increase. Male patients exhibited substantially greater odds of mortality compared to female patients, with odds ratios of 5.262 in the univariate analysis and 21.805 in the multivariate analysis. In this investigation, smoking, diabetes mellitus, hypertension, and ischemic heart disease were not identified as significant predictors of mortality, (Table 7).
| Univariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|
| P | Odds ratio | CI 95% | p | Odds ratio | CI 95% | |||
| upper | lower | upper | lower | |||||
| Age (years) | 0.001* | 1.382 | 1.133 | 1.684 | 0.002* | 1.514 | 1.165 | 1.969 |
| Sex (male) | 0.045* | 5.262 | 1.041 | 26.595 | 0.013* | 21.805 | 1.912 | 28.645 |
| Smoking | 0.332 | 1.867 | 0.529 | 6.583 | ||||
| DM | 0.82 | 0.853 | 0.218 | 3.349 | ||||
| HTN | 0.868 | 1.12 | 0.293 | 4.288 | ||||
| IHD | 0.069 | 0.305 | 0.085 | 1.096 |
Table 7: Univariate and multivariate logistic regression analysis for risk factors that may predict mortality in patients with se
Discussion
Cardiovascular dysfunction is a common manifestation of septic shock and correlates with adverse outcomes. The evaluation of cardiovascular function in these individuals is enhanced by echocardiography [7, 8]. Nonetheless, when utilized in isolation, echocardiography may offer an incomplete representation of the underlying pathophysiology. In recent years, cardiovascular clusters have developed, using clinical and echocardiographic criteria to more accurately delineate the different manifestations of cardiovascular failure in septic shock [9, 10, 11, 12].
In our investigation, patients with left ventricular systolic dysfunction exhibited significantly elevated SOFA and SAPSII scores relative to those with a hyperkinetic profile and prolonged hypovolemia. Nevertheless, no substantial difference was observed in SOFA and SAPSII scores between patients with left ventricular systolic dysfunction and right ventricular failure. Geri G, et al. [7] observed that the SAPS II scores varied significantly among clusters, with Cluster 2 exhibiting the highest scores and Cluster 1 the lowest. Although SOFA scores were not substantially different among clusters, Cluster 4 exhibited the highest median score. Innocenti F, et al. [13] assessed 147 individuals with sepsis and discovered that those with elevated SOFA ratings exhibited impaired left ventricular systolic performance.
In our investigation, patients with left ventricular systolic dysfunction exhibited a reduced ScvO2 level relative to other clusters. No substantial changes were observed in heart rate, respiration rate, temperature, systolic blood pressure, diastolic blood pressure, and mean blood pressure among the clusters. These data indicate that ScvO2 may serve as a valuable signal for identifying patients with left ventricular systolic dysfunction. Conversely, Geri G, et al. [7] indicated that the heart rate was markedly elevated in cluster 2 relative to the other clusters. Cluster 4 exhibited considerably reduced systolic, diastolic, and mean arterial blood pressure compared to the other clusters. The cardiac index in cluster 3 was markedly lower than in the other clusters. Cluster 3 exhibited a considerably elevated ScvO2 in comparison to the other clusters. Cluster 2 exhibited a markedly elevated central venous pressure relative to the other groups.
We established that Cluster I consist of patients exhibiting left ventricular systolic dysfunction, characterized by a markedly reduced mean left ventricular ejection fraction relative to the other clusters. These individuals exhibit reduced LVFAC, diminished mitral E and E’ waves, and decreased aortic VTI, signifying compromised left ventricular function. The E/E’ ratio was markedly lower in Cluster I patients than in the other clusters, signifying compromised diastolic function. The data indicate that patients in Cluster I exhibit considerable left ventricular dysfunction, necessitating specific care measures to enhance outcomes. Geri G, et al. [7] revealed that Cluster 2 had significantly different outcomes compared to the other clusters. Patients in Cluster 2 exhibited the lowest LVEF, LVFAC, mitral E wave, mitral E′ wave, aortic VTI, and RV/LV EDA values, alongside the highest ∆SVC value relative to other clusters. The results indicate that individuals in Cluster 2 may experience more severe heart failure and may necessitate more intensive treatment. Boissier F, et al. [14] indicated that left ventricular systolic failure in septic shock correlates with alterations in loading circumstances, potentially resulting in diminished LVEF.
This study suggested that therapies aimed at loading conditions may enhance LVEF and overall outcomes in septic shock patients with LVSD. Dugar S, et al. [15] discovered that left ventricular ejection fraction (LVEF) exhibited a U-shaped correlation, wherein both elevated and diminished LVEF values were linked to heightened death rates. This indicates that LVSD may exert intricate influences on mortality among patients experiencing septic shock. Kim S, et al. [16] discovered that left ventricular systolic dysfunction (LVSD) correlated with poorer outcomes in individuals experiencing septic shock, with increased left ventricular ejection fraction (LVEF) impairment linked to elevated fatality rates. Sanfilippo F, et al. [17] indicated that a reduction in LVFAC may result in diastolic dysfunction, which may be evaluated using various echocardiographic parameters, such as the mitral E wave, E′ wave, and E/E′ ratio. Research indicates that in individuals with septic shock and left ventricular systolic failure, the mitral E/E′ ratio is markedly elevated in comparison to those with normal left ventricular function [18]. The ROC curve study indicates that an AR of the E wave of mitral inflow ≥750 cm/s² can accurately predict moderate to severe LV diastolic dysfunction with good sensitivity and specificity [19].
Mitral valve regurgitation can influence the mitral E wave velocity, as it indicates blood flow produced by active atrial contraction. In mitral valve regurgitation, the valve leaflets fail to seal securely, resulting in diminished blood flow from the heart to the body. Consequently, an accurate diagnosis is crucial to identify the underlying cause of diminished mitral E wave velocity in individuals with septic shock [19]. Vallabhajosyula S, et al. [20] performed echocardiography on adult patients with severe sepsis and septic shock, revealing that left ventricular systolic dysfunction correlated with reduced ∆SVC, % (p=0.002). A further retrospective cohort study indicated that left ventricular systolic dysfunction correlated with heightened mortality in patients with sepsis and septic shock, although it did not specifically address ∆SVC, %.
A study investigating subclinical left ventricular (LV) systolic dysfunction in septic shock patients employed a global longitudinal strain (GLS) threshold of ≥ -15% to classify LV systolic dysfunction and found a significant correlation between LV systolic dysfunction and reduced ∆SVC, % (p=0.002) (Hai, et al.). A separate study categorized left ventricular (LV) systolic dysfunction according to left ventricular ejection fraction (LVEF) and discovered that patients exhibiting severe LV dysfunction (<30%) experienced a greater prevalence of wall motion abnormalities (including reduced ∆SVC, %) in comparison to individuals with normal LVEF (≥50%) (p<0.001) [16]. We elucidated these results by demonstrating that the mechanism of left ventricular systolic dysfunction in sepsis is influenced by load effects and lipopolysaccharide effects on the systolic function of the left ventricle. In sepsis, the tension in peripheral arteries and veins diminishes, leading to a conversion of stressed volume into non-stressed volume, which results in inadequate effective circulation volume, characterized by low preload and low afterload. At this point, the systolic function of the left ventricle can be markedly improved [21]. In 2017, Vallabhajosyula S, et al. [22] conducted a cohort study with 338 sepsis patients, of whom 55% exhibited right cardiac dysfunction. Cardiac output increases moderately with positive fluid resuscitation in sepsis patients, especially those with septic shock, despite the right ventricle being in a state of low tension under physiological settings. Following the elevation of load on the right ventricle, both the volume load and right cardiac tension concurrently escalate. RVD is induced by lung infections, acute respiratory distress syndrome, and mechanical ventilation, all of which can elevate the afterload on the right heart [22].
The data indicated that the 30-day mortality rate was highest in Cluster I (LV systolic dysfunction) at 60.0%, followed by Cluster IV (RV failure) at 38.5%. Cluster II (LV hyperkinetic profile) exhibited the lowest fatality rate at 13.2%, whereas Cluster V (well-resuscitated patients) recorded no fatalities. The disparity in 30-day mortality between the clusters was statistically significant (p=0.032). In a multivariate model, right ventricular dysfunction was significantly correlated with an elevated 30-day all-cause death rate of 25%. Hassan y, et al. [23] reported that 7% of sepsis patients with left ventricular systolic dysfunction (LVSD) succumbed. Correcting for bias [24] conducted a meta-analysis of over 700 sepsis patients and found no association between left ventricular systolic dysfunction (LVSD) and death in sepsis. The ventricular volume index exhibited no correlation with mortality. A systematic study conducted by Sevilla B, et al. [25] indicated that left ventricular systolic dysfunction (LVSD) lacks both sensitivity and specificity as a mortality predictor in individuals with sepsis. This discrepancy may result from differences in the limited sample size between the two studies [25].
Our results indicate that age is a risk factor related with mortality across various clusters of patients with septic shock. Patients exhibiting an LV hyperkinetic profile had the greatest mean age (71.00±2.8), succeeded by those with chronic hypovolemia (70.00±1.4), LV systolic dysfunction (67.33±3.7), and RV failure (67.00±1.6). The CDC indicates that sepsis-related mortality escalates with advancing age, peaking among individuals aged 65 and beyond [26]. Retrospective cohort research revealed that the all-cause mortality rate for severe sepsis and septic shock patients with left ventricular failure and a mean age beyond 65 years was 43.9%, comparable to the 28-day all-cause mortality rate of 43.1% [27].
Concerning the distribution of gender and mortality among various patient clusters. In patients with left ventricular systolic failure, 60% of deceased individuals were male, but no male patients died among those with a left ventricular hyperkinetic profile or those who were adequately resuscitated. Among patients with persistent hypovolemia, 33.3% of the deceased were male, but in patients with right ventricular failure, 57.1% of the deceased were male. The study by Pietropaoli AP, et al. [28] examined sex-based disparities in hospital mortality among patients with severe sepsis or septic shock necessitating intensive care. The research indicated that hospital mortality rates were not statistically different between males and females. A separate investigation revealed that in a substantial cohort of patients experiencing septic shock due to acute myocardial infarction (AMI), both male and female patients exhibited similar clinical presentations and mortality risks. Lin S, et al. [29] observed gender-specific mortality rates of 28 years and 1 year for individuals. 6,493 men and 5,828 women total 12,321 individuals. 18.37% of the sample perishes at 28 years, comprising 18.57% of males and 18.14% of females (p=0.531). The total one-year mortality rate is 37.46%, comprising 37.24% for males and 37.70% for females (p=0.601).
Our data indicate that smoking correlates with increased mortality in individuals with left ventricular systolic dysfunction and persistent hypovolemia, exhibiting mortality rates of 57.1% and 50%, respectively. Conversely, there were no fatalities among patients who received adequate resuscitation, nor were there any smoking-related deaths in patients exhibiting an LV hyperkinetic profile with RV failure. Smoking is linked to a heightened mortality risk in patients with sepsis [30].
In our investigation, patients with diabetes mellitus (DM) and left ventricular (LV) systolic dysfunction exhibited a death rate of 75%, while those with DM and an LV hyperkinetic profile demonstrated a lower mortality rate of 33.3%. Furthermore, patients with DM and chronic hypovolemia experienced no mortality. Patients with septic shock and LVSD may have a greater prevalence of DM than those without DM. Another study in 2017 revealed that septic shock patients with left ventricular systolic dysfunction and diabetes mellitus exhibited elevated mortality rates relative to those without diabetes mellitus. This study found that the prevalence of diabetes mellitus was 32.7% among septic shock patients with left ventricular systolic dysfunction [31]. A separate study published in the journal Shock in 2019 examined the correlation between diabetes mellitus and septic shock patients with left ventricular systolic dysfunction. The research indicated that patients with diabetes mellitus and left ventricular systolic dysfunction exhibited elevated death rates relative to those without diabetes mellitus [32]. Kushimoto S, et al. [33] identified a significantly elevated in- hospital mortality rate in patients with blood glucose levels <70 mg/dL compared to those with values of 140–179 mg/ dL among those without a prior diagnosis of diabetes.
Our data reveals that patients with left ventricular systolic failure and hypertension exhibit a death rate of 75%. Conversely, patients exhibiting an LV hyperkinetic profile and sustained hypovolemia demonstrate reduced death rates of 33.3% and 0%, respectively. Individuals with right ventricular failure exhibit a death rate of 50%. Patients with ischemic heart disease exhibited a significant death rate across all clusters, with 100% mortality in those with left ventricular systolic dysfunction and 66.7% mortality in those with a left ventricular hyperkinetic profile. Prabhu M, et al. [34] discovered that ischemic heart disease (IHD) was the predominant cause of mortality in septic shock patients with LV systolic dysfunction.
Our study presents the outcomes of univariate and multivariate logistic regression studies aimed at identifying risk variables for mortality in individuals with cardiomyopathy triggered by septic shock. The univariate analysis reveals that advanced age and male gender correlate with a heightened risk of mortality. In the multivariate analysis, advanced age and male gender are significant predictors of mortality. A retrospective study including over 200 patients hospitalized with sepsis or septic shock identified risk factors for septic cardiomyopathy (SICM) as age, male gender, elevated disease severity scores, increased lactate and CRP levels, and pre-existing heart failure [35]. One thousand nine hundred thirty-five patients satisfied the research criteria. 1204 (62.2%) were male, while 731 (37.8%) were female. In multivariable Cox proportional-hazards analysis, females exhibited a reduced risk of in hospital mortality compared to males (HR: 0.74, 95% CI: 0.62–0.89; p=0.001). The subgroup analysis utilizing multivariable Cox proportional hazards indicated that females exhibited reduced in-hospital death rates compared to males (HR: 0.72, 95% CI: 0.58–0.88; p=0.002), [36, 37, 38, 39, 40].
Conclusion
The examination of various clusters according to shock type and the presence or absence of left ventricular (LV) systolic dysfunction, hyperkinetic profile, right ventricular (RV) failure, and persistent hypovolemia demonstrated notable disparities in laboratory and hemodynamic parameters, with LV systolic dysfunction correlating with reduced ScvO2 levels and RV failure linked to elevated central venous pressure. The echocardiographic measurements revealed considerable disparities among the clusters, with patients exhibiting left ventricular systolic dysfunction demonstrating reduced left ventricular ejection fraction, left ventricular fractional area change, and mitral E wave velocity. This study offers significant insights into the clinical profiles and related parameters of individuals with septic shock, which may facilitate the formulation of focused treatment regimens.
Consent for Publication
All authors have read and revised well for the manuscript and agree to publish.
Availability of Data and Material
All data supporting the study are presented in the manuscript or available upon request.
Competing Interests
There is no conflict of interest.
Funding
The author received no financial support for this article’s research, authorship, and publication.
Acknowledgments
Not applicable
Authors’ Information
Not applicable
References
-
Angus DC, Poll T (2013) Severe sepsis and septic shock. N Engl J Med 369(9): 840-851.
-
Gaieski DF, Edwards JM, Kallan MJ, Carr BG (2013) Benchmarking the incidence and mortality of severe sepsis in the United States. Critical care medicine 41(5): 1167-1174.
-
Song J, Cho H, Park DW, Ahn S, Kim JY, et al. (2019) The effect of the intelligent sepsis management system on outcomes among patients with sepsis and septic shock diagnosed according to the sepsis-3 definition in the emergency department. J Clin Med 8(11): 1800.
-
Weiss SL, Peters MJ, Alhazzani W, Agus MS, Flori HR, et al. (2020) Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr Crit Care Med 21(2): e52-e106.
-
Vieillard B, Caille V, Charron C, Belliard G, Page B, et al. (2008) Actual incidence of global left ventricular hypokinesia in adult septic shock. Crit Care Med 36(6): 1701-1706.
-
Begot E, Dalmay F, Etchecopar C, Clavel M, Pichon N, et al. (2015) Hemodynamic assessment of ventilated ICU patients with cardiorespiratory failure using a miniaturized multiplane transesophageal echocardiography probe. Intensive care med 41(11): 1886-1894.
-
Geri G, Vignon P, Aubry A, Fedou AL, Charron C, et al. (2019) Cardiovascular clusters in septic shock combining clinical and echocardiographic parameters: a post hoc analysis. Intensive care med 45: 657-667.
-
Martin L, Derwall M, Zoubi S, Zechendorf E, Reuter DA, et al. (2019) The Septic Heart: Current understanding of molecular mechanisms and clinical implications. Chest 155: 427-437.
-
Kim JS, Kim YJ, Kim M, Ryoo SM, Kim WY (2020) Association between Right Ventricle Dysfunction and Poor Outcome in Patients with Septic Shock. Heart 106(21): 1665-1671.
-
Kakihana Y, Ito T, Nakahara M, Keiji Y, Tomotsugu Y (2016) Sepsis-Induced Myocardial Dysfunction: Pathophysiology and Management. J Intensive Care 4: 1-10.
-
Alroumi F, Abdul AA, Kergo R, Lei Y, Dargin J (2018) The Impact of Smoking on Patient Outcomes in Severe Sepsis and Septic Shock. J Intensive Care 6: 42.
-
Gao JW, Zhang AQ, Wang X, Li ZY, Yang JH, et al. (2015) Association between the Tlr2 Arg753gln Polymorphism and the Risk of Sepsis: A Meta-Analysis. Critical Care 19: 1-8.
-
Innocenti F, Palmieri V, Guzzo A, Stefanone VT, Donnini C, et al. (2018) Sofa Score and Left Ventricular Systolic Function as Predictors of Short-Term Outcome in Patients with Sepsis. Intern Emerg Med 13(1): 51-58.
-
Boissier F, Razazi K, Seemann A, Bedet A, Thille AW, et al. (2017) Left Ventricular Systolic Dysfunction during Septic Shock: The Role of Loading Conditions. Intensive Care Med 43(5): 633-642.
-
Dugar S, Sato R, Chawla S, You JY, Wang X, et al. (2023) Is Left Ventricular Systolic Dysfunction Associated with Increased Mortality among Patients with Sepsis and Septic Shock? Chest 163(6): 1437-1447.
-
Kim S, Lee JD, Kim BK, Kim YH, Kim JH (2020) Association between Left Ventricular Systolic Dysfunction and Mortality in Patients with Septic Shock. J Korean Med Sci 35(4): e24.
-
Sanfilippo F, Huang S, Messina A, Franchi F, Oliveri F, et al. (2021) Systolic Dysfunction as Evaluated by Tissue Doppler Imaging Echocardiography and Mortality in Septic Patients: A Systematic Review and Meta-Analysis. J Crit Care 62: 256-264.
-
Previtali M, Chieffo E, Ferrario M, Klersy C (2012) Is Mitral E/E′ Ratio A Reliable Predictor of Left Ventricular Diastolic Pressures in Patients without Heart Failure? Eur Heart J Cardiovasc Imaging 13: 588-595.
-
Sattarzadeh R, Tavoosi A, Jabbari M, Parsa AF, Geraeli B, et al. (2015) Acceleration Rate of Mitral Inflow E Wave: A Novel Transmitral Doppler Index for Assessing Diastolic Function. Cardiovascular Ultrasound 14: 1-6.
-
Vallabhajosyula S, Gillespie SM, Barbara DW, Anavekar NS, Pulido JN (2018) Impact of New-Onset Left Ventricular Dysfunction on Outcomes in Mechanically Ventilated Patients with Severe Sepsis and Septic Shock. J Intensive Care Med 33: 680-686.
-
Wang J, Wang XT, Liu DW, Zhang HM, Su LX (2020) Induction and Deduction in Sepsis-Induced Cardiomyopathy: Five Typical Categories. Chin Med J (Engl) 133(18): 2205-2211.
-
Vallabhajosyula S, Kumar M, Pandompatam G, Sakhuja A, Kashyap R, et al. (2017) Prognostic Impact of Isolated Right Ventricular Dysfunction in Sepsis and Septic Shock: An 8-Year Historical Cohort Study. Ann Intensive Care 7(1): 94.
-
Bendary A, Said H, Elemary M, Mahrous M (2022) Right Ventricular Function as a Predictor of Short-Term Mortality in Patients with Sepsis and Septic Shock: An Observational Study. Egypt Heart J 74(1): 78.
-
Hassan SY, Settergren M, Henareh L (2014) Sepsis- induced myocardial depression and takotsubo syndrome. Acute Card Care 16(3): 102-109.
-
Huang SJ, Nalos M, Mclean AS (2013) Is Early Ventricular Dysfunction or Dilatation Associated with Lower Mortality Rate in Adult Severe Sepsis and Septic Shock? A Meta-Analysis. Crit Care 17(3): R96.
-
Sevilla B, Ohoro JC, Velagapudi V, Pulido JN (2014) Correlation of left ventricular systolic dysfunction determined by low ejection fraction and 30-day mortality in patients with severe sepsis and septic shock: a systematic review and meta-analysis. J Crit Care 29(4): 495-499.
-
Kramarow EA (2021) Sepsis-Related Mortality among Adults Aged 65 and Over: United States, 2019. NCHS Data Brief 422: 1-8.
-
Yu G, Cheng K, Liu Q, Wu W, Hong H, et al. (2022) Clinical Outcomes of Severe Sepsis and Septic Shock Patients with Left Ventricular Dysfunction Undergoing Continuous Renal Replacement Therapy. Sci Rep12(1): 9360.
-
Pietropaoli AP, Glance LG, Oakes D, Fisher SG (2010) Gender Differences in Mortality in Patients with Severe Sepsis or Septic Shock. Gend Med 7(5): 422-37.
-
Lin S, He W, Hu Z, Bai L, Zeng M (2021) Sex Differences In short and Long-Term Survival Among Critically Ill Patients with Sepsis. Int J Gen Med 14: 613-622.
-
Chicco D, Jurman G (2020) Survival Prediction of Patients with Sepsis from Age, Sex and Septic Episode Number Alone. Sci Rep 10(1): 17156.
-
Song JE, Kim MH, Jeong WY, Young J, Dong H, et al. (2016) Mortality Risk Factors for Patients with Septic Shock after Implementation of the Surviving Sepsis Campaign Bundles. Infect Chemother 48(3): 199-208.
-
Li H, Li C, Bai Y, Chen J, Cai Y (2021) Relationship between Diabetes Mellitus and the Prognosis of Ischemic Heart Failure.
-
Kushimoto, S, Abe T, Ogura H, Shiraishi A, Saitoh D, et al. (2020) Impact of Blood Glucose Abnormalities on Outcomes and Disease Severity in Patients with Severe Sepsis: An Analysis From A Multicenter, Prospective Survey of Severe Sepsis. Plos One 15: E0229919.
-
Prabhu M, Yalakala SK, Shetty R, Ashok T, Sitapara T (2015) Prognosis of Left Ventricular Systolic Dysfunction in Septic Shock Patients. J Clin Diagn Res 9(3): OC05- OC08.
-
Lheureux M, Sternberg M, Brath L, Turlington J, Kashiouris MG (2020) Sepsis-Induced Cardiomyopathy: A Comprehensive Review. Current Cardiology Rep 22(5): 1-12.
-
Kondo Y, Miyazato A, Okamoto K, Tanaka H (2021) Impact of Sex Differences on Mortality in Patients with Sepsis After Trauma: A Nationwide Cohort Study. Front Immunol 12: 678156.
-
Singer M, Deutschman CS, Seymour CW, Shankar HM, Annane D, et al. (2016) The third international consensus definitions for sepsis and septic shock (Sepsis-3): JAMA 315(8): 801-810.
-
Shankar HM, Phillips GS, Levy ML, Seymour CW, Liu VX, et al. (2016) Developing a new definition and assessing new clinical criteria for septic shock: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3): JAMA 315(8): 775-787.
-
Thompson K, Venkatesh B, Hammond N, Taylor C, Finfer S, et al. (2021) Sex Differences in Response to Adjunctive Corticosteroid Treatment for Patients with Septic Shock. Intensive Care Med 47(2): 246-248.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index