Arsenic Exposure and the Risk of Cancer
It is known that exposure to environmental chemicals increases the risk of cancerous and non-cancerous pathologies. Geomedical and anthropic evidence indicates that there is a close relationship between increased morbidities from cardiovascular diseases and cancer among the population in the Antofagasta Region and the etiology of exposure to arsenic. The most commonly used drugs with chemotherapy are platinum-based. The present work characterizes short-term urinary evacuation, that is, the pooled urine excreted 24 hours after the first cycle of treatments of cancer patients with cisplatin or carboplatin. The inorganic biochemical status and behavior of excreted As, Se and Pt administered to and evacuated by patients could be involved in the post-treatment quality of life of the patients and the evolution and final outcome of the disease. There were 90 patients in the group, 32 with lung cancer and 58 with different cancers termed “other types of cancerâ€, as well as 10 patients untreated with platinum-based drugs. Platinum and selenium were determined by ICP-OES and As by HGAAS. The detection limits were 7.7, 5.4 and 0.2 (ng/mL), respectively. The decreasing tendency of the administered Pt followed the order: carboplatin (other types of cancer) >cisplatin (lung cancer) >cisplatin (other types of cancer); the short-term urinary excretion of Pt was low. The decreasing tendency of the quantities of excreted Se was: carboplatin (other types of cancer) >cisplatin (other types of cancer) ≈ cisplatin (lung cancer); and the tendency of decreasing quantities of excreted As was cisplatin (other types of cancer) >carboplatin (other types of cancer) >cisplatin (lung cancer).The quantities of excreted Pt did not present significant differences among the cases of patients with lung cancer or with other cancers treated with cisplatin, despite significant variations in the quantities of Pt administered by the drug. The tendency in quantities of excreted Pt was similar to that of selenium and arsenic, but the evacuation of selenium was greater than that of arsenic, including in the group of patients with “other types of cancer†treated with drugs without Pt. The results of the study could arise from the subtle participation of antagonist mechanisms among Se, As and Pt that are involved in apoptotic and autophagic events in homeostasis, which could indicate the presence of cancer in patients from areas with chronic exposure to arsenic, as is the case of the Antofagasta Region in Chile.
Introduction
The deterioration of the quality of healthy life for the inhabitants of the Antofagasta Region of Chile is reflected in particular by the increased risk of contracting cancer and cardiovascular and neurological pathologies. Although the problem could be multimetalic [1], arsenic appears to be one of the main environmental stresses causing these serious health problems [2, 3]. According to geomedical and anthropic sources [4], there could be a close relationship between the incidence of cancer and its evolution among patients in the Antofagasta Region, associated with the status of As and Se, and Pt administered in acute form through drugs like cisplatin and carboplatin [5].
The geological structures of certain places on the planet have an influence on human health [6]. The Antofagasta region of Chile is located in a Andean Altiplano-coastal desert system. Large-scale mining activities have been carried out in the region over a long period [7], which has had an impact on ecosystems and the quality of health of human beings [8]. Human health problems of cancerous and non-cancerous pathologies associated with contamination by As are present in many parts of the world [9]. However, this situation reaches alarming levels in the Antofagasta Region given that the incidence of cardiovascular pathologies [3] and lung cancer, which is similar whether the arsenic is ingested or inhaled [10], and the mortality rates by cancer are higher than those in any other population exposed to arsenic in the world [11].
There is an overwhelming amount of knowledge about the toxic effects of arsenic on ecosystems and humans [12]. However, there is a wide variety of diseases, disorders and dysfunctions related specifically to exposure and the stressing effects of other heavy metals, and the imbalance of essential elements when conditions of exposure submit human beings to synergetic multi-elemental effects [1]. Pt is a heavy metal that is non-essential for living things. In recent years there has been interest within the scientific community in Pt as a pollutant owing to its emission from automobile catalyzers, its use in prosthesisand in anti-tumor drugs [13, 14]. The administration of Pt-based drugs has an impact at the cellular level, affecting human metabolism and physiology and submitting homeostasis to stress. On the one hand, it tends to maintain electrolytes, nutrients and trace elements in a steady state, while minimizing the adverse effects of toxic substances like heavy metals [15, 16]. The main side effects of the application of Pt drugs are loss of hearing (ototoxicity), kidney dysfunction (nephrotoxicity) [17], and resistance to anti-cancer drugs [18]. The spreading of the cancer or metastasis [19] represents the failure of this type of treatment.
The antagonist or mutually detoxifying effects between arsenic and selenium has been confirmed in many ecosystem wild species and in humans [20, 21]. In humans selenium presents bioinorganic antagonism with As and Pt [22, 23, 24] and apparently the status of selenium could be of particular importance in humans submitted to environmental stress by heavy metals. The protective effect of selenium strengthens the cellular antioxidant capacity of DNA and other cellular components from damage by reactive oxygen species (ROS) [23, 25] through antioxidant selenium enzymes such as glutathione peroxidase [26] and thioredoxin reductase, which require Se (IV) for their expression [23, 27]. Selenium has been recognized as a broad-spectrum anti-cancer agent and has even been considered as a prime element in drug- chemotherapy treatment [28]. The vulnerability of this cellular protection capacity can also result in side effects of and resistance to Pt-based drugs [18] and metastasis [29, 30].
The present work assumes that selenium is the main antagonist of As and Pt. There is evidence that not only arsenic can inhibit the anti-cancer effect of selenium [31], but also its interaction with essential trace elements and other heavy metals such as Cu, Zn, Cd, Hg, Sn, Pb, Ni, Co, Sb, Ag, Au and Mo [32]. A study by Vahter [33] about urinary excretion of Se and As among pregnant women from northern Chile found a significant association between the concentrations of these elements excreted in the urine. Drugs that contain Pt, such as cisplatin and carboplatin, have been shown to increase the biliary excretion and distribution of Se in tissue, but Pt has not been shown to significantly influence the urinary or respiratory excretion of Se [34]. However, the distribution of Se in tissue is altered by cisplatin, resulting in high concentrations of Se in the liver, kidney, plasma and low levels of Se in the testicles and brain. Drugs based on As, Pt and Au can alter the availability of selenium in the synthesis of selenoenzymes and interferes with the availability of Se, altering its distribution, methylation and/or excretion [35].
The presence of Pt-based drugs in the cells and their distribution in sub-cellular compartments (17) depends on transport mechanism to and from the cells, which are stages of homeostasis that are not well understood. In the case of Pt, this occurs via chaperon proteins of the homeostasis of copper, the transport protein termed CTR1 [15, 35]. The control of Pt output from the cells also involves two types of proteins, ATP7A and ATP7B that belong to the family of P-type ATpase [15]. Numerous studies conducted with large quantity of different Pt complexes have established a series of generalizations about the mechanisms of action and the relationship between structure and reactivity to anti-cancer drugs [36]. In these mechanisms, it is supposed that if a drug like cisplatin is able to pass through the cellular membrane and reach the nucleus of the cancerous cell, it will interact with the DNA forming complexes that facilitate apoptosis, thus inhibiting the proliferation of sick cells [17]. At the same time, Se and Pt of cisplatin may inhibit the catalytic function of the telomerase [37], interfering with the maintenance of telomere length, which can help in restricting the replication of tumor cells [38].
Studies of urinary excretion of Pt among patients submitted to chemotherapy with cisplatin have generally been carried out well after treatment, ranging from six months to 16.8 years [39]. In the present work, we investigated the provision of platinum to cancer patients via cisplatin and carboplatin drugs and the corresponding short-term excretion of As, Se and Pt in 24-hour urine, which is immediately after the first or second cycle of treatment. The short-term urine can be a good matrix to determine the behavior of As, Se and Pt among patients whose cancer was very probably triggered by exposure to arsenic. The knowledge obtained could contribute to a better understanding of the mechanisms of side effects, resistance to Pt-based drugs, optimal doses of these drugs and the resistance or permissiveness to the diffusion of cancer or metastasis.
Materials and Methods
The work was carried out in accordance with the Helsinki Declaration and with consent and authorization of the Health Service of Antofagasta, Chile, according to ORD 4391 (August 20, 2008), as well as the authorization of the Ethics and Biosafety Committee of the Universidad de Antofagasta (CEICREV / 2008).
Population and Sample Collection
The urine samples were collected for 24h immediately after the infusion of platinum-based drug to 90 patients with cancer in the Antofagasta Region, Chile. The samples were provided by the Oncological Center of Antofagasta Regional Hospital. The distribution of the types of cancer of the patients was the following: 32 lung cancer, 16 cancer of the ovaries, 12 cervical-uterine cancer, 8 testicular cancer, 5 of the thymus, 3 of the esophagus, 3 gastric cancers, 3 Hodgkin’s lymphomas one each of cancer vagina, gallbladder, tonsils, salivary glands, osteosarcoma and bladder, respectively. Three of the four patients with ovarian cancer initially treated with cisplatin were again treated with cisplatin after 28 days, while the fourth patient was treated with carboplatin. Patients with cancers other than lung cancer were termed patients with “other cancers”. Only patients in this group were treated with carboplatin. As well, there were 10 24-hour urine samples of patients submitted to treatment without platinum-based drugs. The samples were collected between May and August of 2005.
Chemicals, Solutions, Materials and Instruments
Chemicals employed were Instra (J. T. Baker), Suprapur (Merck) and of p.a. quality. The solutions were prepared in deionized water subsequently distilled in quartz, with conductivity of less than 0.5 µMHO/cm at 25 °C. The deionization was done in a deionizer with two ionic exchange cartridges Cole Parmer (USA) in tandem, Metex 01506-45– Research 01506-35.
The glass materials used were sequentially treated for 24 hours with 2 M solutions of hydrochloric and nitric acid, prepared from quality p.a. Merck chemicals. After washing with water, the glass materials were treated for another 24 hours with a 0.025 M solution of the disodium salt of ethylendiaminotetraacetic acid (EDTA), prepared from Titriplex III reactive from Merck, after which they were rinsed with water.
The standard dilutions were prepared based on the primary solution of Pt(II) Certipur from Merck and of Se(IV) from the primary solution Tritisol from Merck, both of 1000 mg L-1. Based on these, an intermediate standard dissolution of 50 mgL-1was prepared, from which the working dilutions were prepared. The standard As solutions were prepared from a primary solution of disodium arsenate Titrisol Merck of 1000 mgL-1, from which an intermediate standard dissolution of 500 mgL-1 was prepared for the working dilutions. To generate arsenic hydride, a 10 M solution of chlorhydric acid was supplied, prepared from the Instra chemical of J. T. Baker. A solution of sodium borohydride at 3% p/v was used, prepared in a solution of sodium hydroxide at 1% p/v, both p.a. quality Merck chemicals.
The urine samples were transported at a temperature of 4-5ºC to the laboratory, which was acclimatized, pressurized and equipped with a laminar flow hood (Labconco Purifier Class II). The samples were microfiltered in a Nalgene system through a Millipore membrane of cellulose ester with pore size of 0.45 µm and diameter of 47 mm. The samples were then preserved in storage at-20ºC. Immediately after being thawed out, the urine samples were again microfiltered, this time through a Millpore cellulose ester membrane of with 0.22 µm pore, protected by a borosilicate glass pre-filterMFS of 0.7 µm and 47 mm in diameter.
To have a control with a matrix of electrolytes with an ionic force comparable to that of the human urine of the cancer patients, surrogate urine was prepared by diluting sub-tidal seawater three times with distilling it deionized water. As a reference, the measured average salinity of the urine samples was 13 ppt, which were measured with an Orion Ionometer model 1260 (USA), previously calibrated.
Digestion of the Urine Samples
The urine samples and the controls were mineralized by wet process in Teflon bombs with 10 mL of nitric acid Instra-Baker JT, for 2 h at 150ºC in a homemade ceramic oven with an internal temperature sensor. Once cooled and open, additionally 0.25 mL of perchloric acid and 0.50 mL of sulfuric acid were added to the Teflon bombs with the digested samples, both acids of Suprapure, Merck grade. Samples were then reheated under the same time and temperature conditions as before. Finally, the samples were transferred to Erlenmeyer flasks and heated at 250ºC under a gas extraction hood to eliminate excess acids. The volumes of the samples were completed at 50 mL with deionized water, and then microfiltered through a 0.22 µm Millipore membrane with a 0.7 µm fiberglass pre-filter (MFS GF 75).
To determine total arsenic, 5 mL aliquots of samples and controls were digested to semi-reflux under a temperature program between 85 and 300ºC [40]. Once cooled, the samples and controls were diluted volumetrically with HCl 0.5 M, prepared from the Instra reactive from Baker JT.
Determination of total Pt and Se in urine through inductively coupled plasma optical emission spectrometry (ICP–OES)
With the aim of meeting the condition of matrix matching for both acidity and ionic force, aliquots of three samples of digested urine were diluted volumetrically with a NaOH solution, yielding an average acidity equivalent to an approximate pH of 2. To compatibilist the condition of similarity of ionic force and acidity for the preparation of the analytical control for the Pt and Se determinations, seawater was diluted 8 times (10 mL of sample diluted three times
| As | |
|---|---|
| HG-AAS | |
| Bandpass width | 2 nm |
| Bandpass height | Normal |
| Lamp current | 8.0 mA |
| Backup current | 30 mA |
| Temperature EHG 3000 | 920ºC |
| N2 flow | 45-50 mL /min |
| Stabilizing time of the signal | 60 sec |
| Reading time | 10 sec |
| Pt - Se | |
| ICP-OES | |
| Pt spectral line | 265.945 nm |
| Se spectral line | 196.026 nm |
| Nebulizing flow | 0.40 L/min |
| Line detection height | 6.8 mm |
| Pump | 17.0 rpm |
| Power | 1200 W |
| Auxiliary Gas | 0.6 L/min |
| Ar feed | 12.0 L/ min |
| Nebulizing chamber | Spray Trace with Micromist nebulizer at 200 µL/ min. |
Table 1: Instrumental conditions for urine As, Pt and Se determinations.
and diluted volumetrically with 50 mL). When necessary, the solution was adjusted to pH 2 with Instra nitric acid of J. T. Baker. Subsequently, the bi-metallic Pt-Se standard was also prepared in this medium.
To construct the calibration curve, the platinum- selenium bimetallic standard was prepared by dilution of the solutions of 50 µg / mL, in the order Pt-Se: both of 100; 500-200; 1000-300; 2.500-400; and 5.000-500 ng / mL. The bimetallic standard of the highest concentrations was used in the optimization instrumental parameters. The ICP-OES measurements was carried out in a GBC Integra XL (Australia), conducted in a Spray Trace nebulizer chamber from Glass Expansion (USA). N2 and Ar2 analytical grade 5 gases were used. The optimized experimental conditions are shown in Table 1. The urine samples of patients treated and not treated with platinum-based drugs were submitted to the procedures and analytical methods previously described. The base line was adjusted with the analytical blank solution, that is, surrogate urine, diluted as described before, and the quality controls were made evaluating the recovery of internal Pt-Se standards over the analytical control and real samples.
Determination of total Asin urine with hydride generation atomic absorption spectrometry (HGAAS)
Determination of As was done in an atomic absorption spectrophotometer GBC 909 AA implemented with a continuous flow hydride generator HG 3000 and an electrothermal atomization system EHG 3000, employing quartz cell supplied by GBC (Australia) and a boosted current lamp named super lamp from As Photron (Australia).The optimized conditions for measuring As through hydride generation atomic absorption spectrometry (HGAAS) is presented in Table 1. Multiple standard addition methodology was applied, for which an intermediate standard solution was prepared in HCl 0.5 M of 500 mg / L from a primary standard solution, Titrisol Merck, from which a working solution of 1000 µg / L was prepared. Based on this solution, additions were made on a sample of surrogate urine, which had been made from 2.0 µg / L in As. The additions were 50, 100, 150 and 200 µL, to which the concentrations added were 2, 4, 6 and 8 ng / mL, respectively.
The urine samples of patients treated and not treated with platinum-based drugs were submitted to the procedures and analytical methods previously described. The base line was adjusted with the analytical blank solution, that is, diluted succedaneum urine, as described before, and the quality controls were made evaluating the recovery of internal Pt-Se standards over the analytical control and real samples.
Creatinine Urine Analysis
One of the most commonly used tests to evaluate renal function is the clearance or endogenous creatinine depuration of the blood [41], which consists of measuring the volume of blood that the kidney is capable of depurating per minute in creatinine. Prior to beginning treatment with anticancer drugs, it is recommended that the patient’s creatinine clearance (CrCl) level not be above 60 mL / min [42]. One of the ranges considered normal for creatinine is between 80-120mL/min [43]. The Jaffé method [44] was applied in this work to determine CrCl, which involves spectrophotometric measurement of the reaction between picric acid and creatinine.
Statistics
The statistical analysis was made with the STATISTICA 9.1 program (Stat Soft, Tulsa, Oklahoma, USA); a value of p < 0.05 was considered statistically significant.
Results and Discussion
Determination of Pt, Se and As
The calibration curves for the ICP – OES determinations of the total concentrations of platinum and selenium in urine, were linear. In the case of Pt, the parameters of the calibration equation were: Intercept = 93.45 counts x seg-1, slope = 1.079 counts x sec-1/concentration, r = 0.9998. For Se, the parameters were: Intercept = 55.47 counts x sec-1, slope = 1.720 counts x sec-1 / concentration, r = 0.9880.
The linearity parameters of the application of the multiple standard addition methodology for the total arsenic concentrations were also linear: Intercept = 0.0375 uA, slope = 0.01615 uA / concentration, r = 0.9977. The results of the quality control and analytical validation are presented in Table 2.
| N | C. Adic. (ng / mL) | C. Enc. ng / mL) | % Rec. | ± CV (%) | Er (%) | LD (ng/mL) | |
|---|---|---|---|---|---|---|---|
| Pt | 11 | 1000 | 971 | 97.1 | 5.7 | 2.9 | 7.7 |
| Se | 11 | 300 | 290.9 | 97 | 6.3 | 3 | 5.4 |
| As | 11 | 4 | 3.87 | 96.7 | 6.1 | 3.3 | 0.22 |
Table 2: Analytical validation of the determinations of As, Se and Pt in urine.
Statistical Parametric Treatment
The Table 3 shows the descriptive statistical results of the Pt administered by drugs and the quantities of Pt, As and Se excreted, discriminated by the type of drug and cancer. The results presented in Table 3, it can be observed that the decreasing tendency of administered Pt was: carboplatin (other types of cancer; 695 mg) >cisplatin (lung cancer, 163 mg) > cisplatin (other types of cancer; 120 mg). The tendency of excreted Pt was same as that of administered Pt. The tendency of quantities of excreted Se was: carboplatin (other types of cancer; 1.59 µg) >cisplatin (other types of cancer; 1.22 µg) ≈ cisplatin (lung cancer; 1.28 µg). In the case of excreted As, the tendency was: cisplatin (other types of cancer; 71 ng) >carboplatin (other types of cancer; 40.8 ng) > cisplatin (lung cancer; 23.5 ng). It is interesting to note that in the treatment of other types of cancer with drugs without Pt, there was a higher level of evacuation of Se than of As, which implies a negative impact on the protective effect of Se on DNA and other cellular components from damage by reactive oxygen species (ROS) [25].
| Drug | Type of cancer | Parametrs | PtSUM(mg) | PEX(μg) | SeEX(μg) | AsEX(ng) | ||
|---|---|---|---|---|---|---|---|---|
| Cisplatin | Lung cancer | X | 163 | 35.3 | 3.62 | 127 | ||
| Cisplatin | Lung cancer | Med | 156 | 28.2 | 1.28 | 23.5 | ||
| Cisplatin | Lung cancer | DS | 66.6 | 25.9 | 6.45 | 267 | ||
| Cisplatin | Lung cancer | n | 32 | 32 | 24 | 21 | ||
| Cisplatin | Lung cancer | Min | 39.1 | 3.94 | 0.208 | 1.88 | ||
| Cisplatin | Lung cancer | Max | 263 | 90.4 | 22 | 1180 | ||
| Cisplatin | Lung cancer | Cisplatin | Other types of cancer | X | 174 | 40.1 | 1.35 | 216 |
| Med | 120 | Cisplatin | Other types of cancer | 32.5 | 1.22 | 71 | ||
| DS | 324 | Cisplatin | Other types of cancer | 36.1 | 0.717 | 424 | ||
| n | 47 | Cisplatin | Other types of cancer | 47 | 36 | 31 | ||
| Min | 31.6 | Cisplatin | Other types of cancer | 0.76 | 0.354 | 18.8 | ||
| Max | 2297 | Cisplatin | Other types of cancer | 175 | 2.84 | 2300 | ||
| Carboplatin | Other types of cancer | X | 695 | 262 | 1.59 | 40.8 | ||
| Carboplatin | Other types of cancer | Med | 743 | 283 | 1.63 | 22.5 | ||
| Carboplatin | Other types of cancer | DS | 189 | 201 | 0.711 | 46.9 | ||
| Carboplatin | Other types of cancer | n | 11 | 11 | 9 | 6 | ||
| Carboplatin | Other types of cancer | Min | 433 | 9.8 | 0.516 | 2.53 | ||
| Carboplatin | Other types of cancer | Max | 917 | 680 | 2.52 | 121 | ||
| Control samples | Other types of cancer | X | 1.77 | 62 | ||||
| Control samples | Other types of cancer | Med | 1.78 | 62 | ||||
| Control samples | Other types of cancer | DS | 1.14 | 59.4 | ||||
| Control samples | Other types of cancer | n | 7 | 2 | ||||
| Control samples | Other types of cancer | Min | 0.333 | 20 | ||||
| Control samples | Other types of cancer | Max | 3.29 | 104 |
Table 3: Basic statistics of the administered Pt amounts through the applied drugs and the excreted amounts of Pt, As and Se in 2
Creatinine clearance was determined to evaluate renal impact after the first cycle of treatment with cisplatin among patients with lung and other cancers, and patients with cancer of the ovaries submitted to a second cycle of treatment (patients 5, 6, 15 and 25), as well as patients with other cancers treated with carboplatin. According to one of the most recognized threshold ranges [43], 82 of the 90 patients Drugs Type of cancer Parameter µgPtEX/g Cr µg SeEX/g Cr ng AsEX/g Cr Cisplatin Lung cancer presented kidney damage, which shows the impact of these treatments; however, this is a controversial parameter [45]. On the other hand, the population data of the quantities of excreted Pt, Se and As in 24-hour urine of cancer patients, normalized by g of creatinine (Table 4), presented the same tendency of distribution and statistical significance as the non-normalized excreted quantities.
X 1.05 143 5.57 Med 1.06 49 2.08 DS 0.625 263 8.94 n 32 24 21 Min 0.136 7 0.36 Max 2.52 1028 31.1
| Cisplatin | Other types of cancer | X | 1.39 | 83.9 | 7.96 |
|---|---|---|---|---|---|
| Med | 0.969 | 40.7 | 2.55 | ||
| DS | 1.59 | 186 | 17.1 | ||
| n | 47 | 36 | 31 | ||
| Min | 0.11 | 11.3 | 0.28 | ||
| Max | 7.26 | 1136 | 91.2 | ||
| Carboplatin | Other types of cancer | X | 13.3 | 156 | 10.1 |
| Med | 11.9 | 72.2 | 2.55 | ||
| DS | 9.76 | 182 | 18.5 | ||
| n | 11 | 9 | 6 | ||
| Min | 0.78 | 25.5 | 0.4 | ||
| Max | 32.5 | 484 | 47.7 | ||
| Control samples | Other types of cancer | X | 51.6 | ||
| Med | 54.6 | ||||
| DS | 33.7 | ||||
| n | 7 | ||||
| Min | 5.3 | ||||
| Max | 92.3 |
Table 4: Basic statistics of the excreted amounts of Pt, As and Se expressed as metal x(g creatinine)-1 in 24-hour urine (ex = ex
The comparison between the reference of normalized quotients of total metal amount values for healthy persons, that is to say, As 33,3 µg / g CRE [46, 47]; Se (women) 9.8 µg / g CRE; Se (men) 13.5 / g CRE [48]; and, Pt 3.3 ng / g CRE [49] and the results obtained in this work, indicate that the mean of this quotient in persons with cancer were lower than those for healthy persons, while the quotients obtained for Se and Pt were higher than the quotients for healthy persons. Comparing the quotients of persons with cancer from this work to those of persons with cancer obtained from other studies, As (arsenisized persons without cutaneous lesions) 116 µg / g CRE; As (arsenisized patients with skin cancer) 121,2 µg / g CRE (46); Se 206,7 µg / g CRE [50] and Pt 0.30- 4.18 µg / g CRE [39], it can be observed that in the case of As, the mean values of the quotient are lower than those of persons with skin cancer reported in the literature. For Se, the values reported in the literature are higher than ours, and for Pt from cisplatin, the quotients were within the range of those previously reported. However, in the case of Pt from carboplatin, the quotient obtained in this work was approximately three times as high as the value found in the literature [39]. Owing to the multiplicity of factors involved in the excretion of creatinine, there producibility of the heavy metal / creatinine quotient values is they are not analytically satisfactory, so this parameter it is poorly representative clinically [45].
There were no significant differences in the amounts of excreted Pt between patients with lung and other cancers treated with cisplatin, despite significant differences in the quantities of administered Pt. The amounts of excreted Se and As were similar to that of excreted Pt, independent of the type of Pt-based drug and the type of cancer being treated. Nevertheless, there was less evacuation of arsenic than selenium, which suggests that Pt favors the evacuation of Se, or in other words, Pt is more antagonistic to selenium than As, while selenium is also antagonistic to arsenic [23, 24, 31, 51].
Multivariate Statistical Treatment
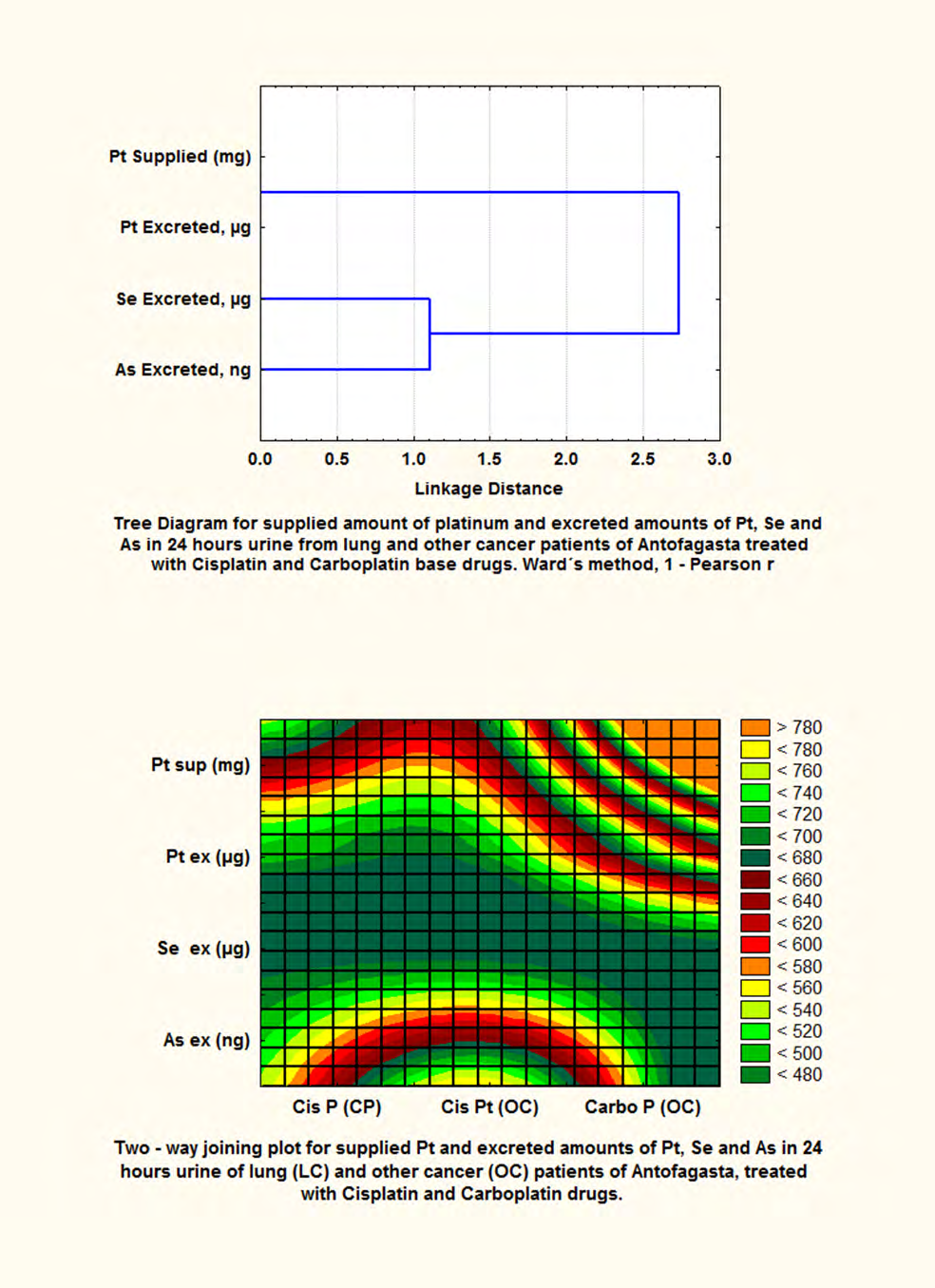
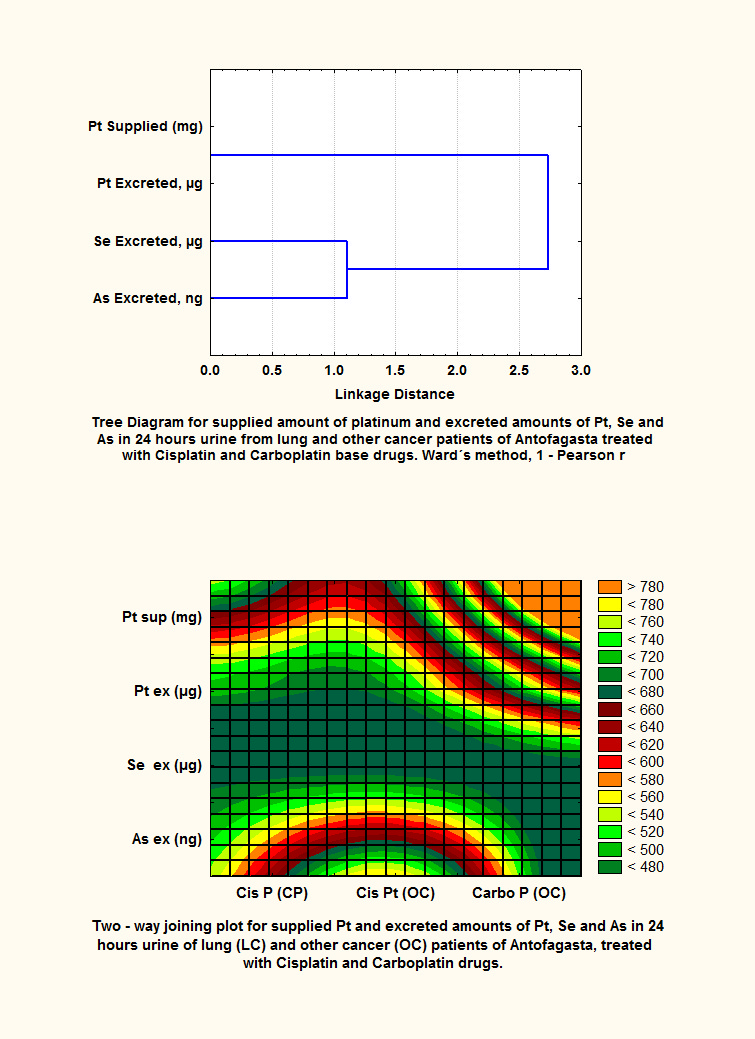
The cluster technique was applied to the involved variables, that is to say, Pt administered amounts through Pt- based drugs and the amounts of Pt, As and Se evacuated in 24-hour urine, following treatment of cancer patients with cisplatin and carboplatin. Cluster analysis is a multivariate statistical methodology applied to data sets when there is a lack of information about the classes making up the data. The basic objective is to group the variables by similarities [52]. The technique is based on two important aspects, the way of measuring the distance between the variables (metric) and the groupings or clusters (linkage or amalgamation rule) [53]. The technique was applied to the most representative sets of values in accordance with the tendency of the data distribution according to the Shapiro-Wilkinson test; Ward’s method was applied with Pearson’s 1-r approximation, to measure the distance between variables and the groupings or clusters.
Figure 1 shows the dendrogram of the variables related to the 24-hour urine after the first cycle of treatment with cisplatin to lung cancer and other cancer patients. As well, four patients with ovarian cancer were considered after a second cycle of treatment. Carboplatin was only used to treat patients with other cancers, in that one of them came of a second treatment cycle. Figure 2 shows two main groupings [Pt administered-Pt excreted] and the amounts of As and Se evacuated dueto Pt induction [Se, As excreted]. From the application of the bidimensional grouping technique Figure 2, it was possible to compare the quantitative extension of administered Pt and the corresponding evacuations of Pt (µg), Se (µg) and As (ng) in 24-hour urine. It can be concluded that urinary excretion of Pt following the infusion of cisplatin and carboplatin at short term is low, even in the case of more than one cycle of applying the drug, which implies that Pt is predominantly distributed and bio-accumulated in tissue. In healthy persons the expression of selenoproteins requires the incorporation of selenocysteine through the mediation of tRNA, for which a daily intake of 55 µg of selenium is necessary [27].
Figures 3 and 4 show the plotting results for the statistic dispersion due the application of the linear correlation model of excretion of Se and As, respect to Pt excretion then the treatment with cisplatin for lung and other cancers, respectively. In the case of Pt from cisplatin for patients with other cancers (Figure 3), the evacuation tendency of As is inverse to the increased evacuation of Pt. In relation to the evacuation of Se, only a small group of patients presented increased excretion of Se in function of Pt increased excretion. In the majority of the cases, selenium was distributed above and below the interval of confidence (95 %). For Pt from cisplatin administered to lung cancer patients (Figure 4), the evacuation of As increased linearly with the increased excretion of Pt, and the evacuation of Se was similar to that described for patients with other cancers treated with cisplatin. In the case of patients with cancers other than lung cancer who were treated with carboplatin, the dispersion plott of evacuated Se and As compared to excreted Pt (Figure not shown) presents inverse tendencies, which was more significant for As (r = -0.2713).
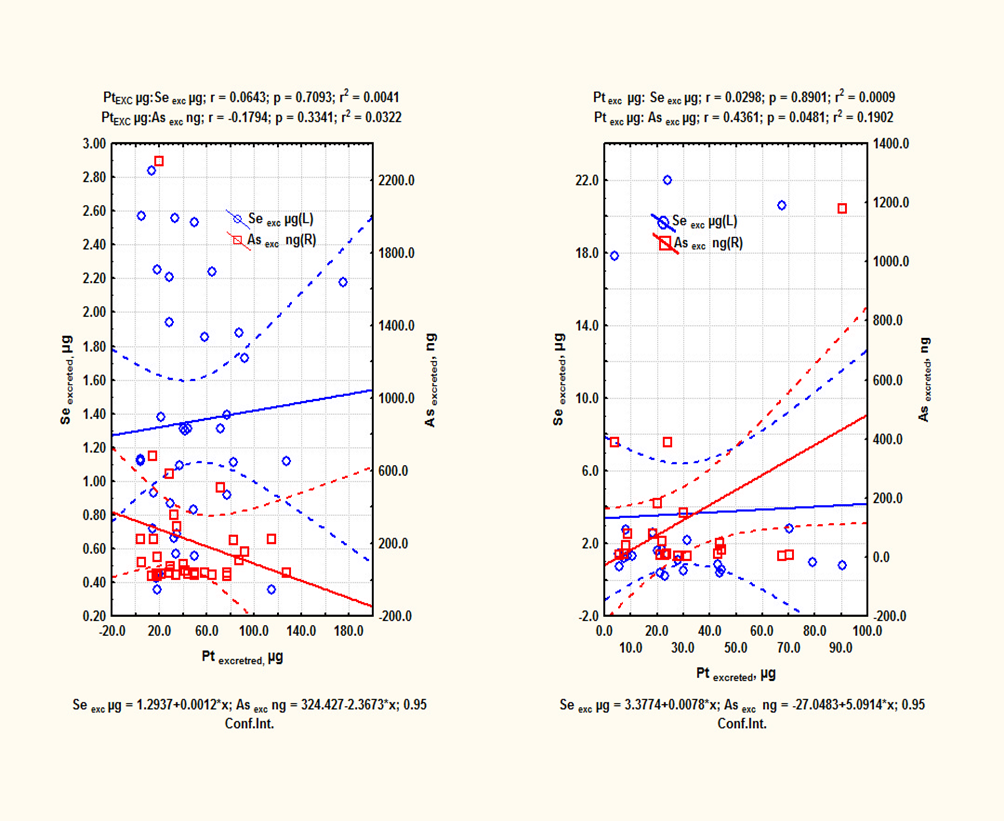
With regard to Pt administered through cisplatin to patients with other cancers, evacuations of Se and As did not present any tendencies. In the case of cisplatin, administered to lung cancer patients, As tended to present an inverse linear tendency(r = -0.2918). In terms of Pt administered with carboplatin to patients with other cancer, As tended to present a direct linear tendency(r = 0.3987) and Se tended to present an inverse linear tendency (r = -0.2388).There is a well-established correlation between exposure to arsenic in the Antofagasta Region and the risk of bladder, lung and skin cancer [54]. Thus, the status of arsenic and selenium in these patients could be important for the activation of carcinogenic mechanisms due to exposure to arsenic [55]. It has been proposed that these mechanisms involve both genetic and epigenetic processes [56, 57], the latter being related to the stress that arsenic provokes in cells without affecting their DNA, but that directly influence genome expression. In this complementary mechanism, arsenic participates as an opportunistic carcinogen, enhancing the genotoxicity and mutagenicity of other environmental stressors [55]. As well, during the treatment with Pt-based drugs, the patient was exposed to an acute impact by Pt, subjecting homeostasis to stress, which is an auxiliary metabolic mechanism to repair biochemical cellular deregulation.
Among cancer patients from areas exposed to chronic effects of arsenic, selenium - platinum and also arsenic can participate synergically in the regulated and unregulated activation of apoptosis, phagocytosis, and cellular homeostasis involved to toxicological and hormesical mechanisms in competence [17, 56, 58, 59]. Specifically, hormesis is the regulated overcompensation of the perturbation of cellular homeostasis [15, 60]. Apoptosis, or programmed cell death, is a normal process through which damaged cells die. This process is deactivated or deregulated in a cancerous state, resulting in the proliferation of cancerous cells. Autophagy, which literally means “eating one’s self”, is a survival mechanism that allows the cells to partially digest its own content, which can be a double-edged sword in that it can help in the survival of healthy cells to the detriment of moribund cells, but the reverse is also possible. Chemical substances can assist autophagy [61] in destroying cancerous cells that are resistant to apoptosis.
Given that, Platinum and Arsenic are not essential elements for human beings, while Se is essential [28], one mayor evacuation of Se than As implies its protective effect is being reduced, being favored side-effects, metastasis or cancer dissemination [23, 27, 62].
Conclusion
The analytical validation and the quality control results of the determinations of Pt and Se by ICP-OES and As by HGAAS in 24-hour urine of cancer patients, indicate that the techniques applied in this work were analytically suitable and the surrogate urine prepared from contaminant-free seawater, proved be important to optimize the analytical merits and the representativeness of the applied analytical techniques.
The short-term Pt, As and Se 24-hour urinary evacuation, that is, immediately after the first or second cycle of treatment of cancer patients with cisplatin or carboplatin, was characterized. The group under study was composed of 90 cancer patients from the Antofagasta region, among whom patients with lung cancer predominated. As is well know, the region is subject to chronic exposure to arsenic. The short term urinary excretion of Pt administered through Pt-based drugs was low, including in the cases with more than one cycle of applying the drug, which implies that the Pt is predominantly distributed and bio-accumulated in the tissues. The decreasing tendency of Pt administered by the drugs was carboplatin (other types of cancer) >cisplatin (lung cancer) >cisplatin (other types of cancer) and the tendency of excreted Pt was the same as that of the administered Pt; while there was observed a decreasing tendency in the amounts of excreted Se with carboplatin (other types of cancer; 1.59µg) >cisplatin (other types of cancer; 1.22µg) ≈ cisplatin (lung cancer; 1.28µg). In turn, the tendency in decreasing quantities of excreted As was cisplatin (other types of cancer; 71ng) >carboplatin (other types of cancer; 40.8ng) >cisplatin (lung cancer; 23,5ng). The group of patients with other types of cancer, treated with drugs not containing Pt also presented a higher evacuation of selenium than of As.
According to the threshold range of one of the most recognized creatinine clearance indices, 82 of the 90 patients presented renal damage. The values of the metal/creatinine quotients obtained in this work represent short-term evacuations, which were different from the reference values of the quotients of healthy persons. For As, the mean of the values of the quotients of persons with cancer reported in this work were lower than those of healthy persons. In turn, our results for Se and Pt were higher than the quotients for healthy persons. The quotients from other studies for arsenic and selenium from persons with cancer were higher than those obtained in this work, but the quotients in our study for Pt from cisplatin were within the range reported previously for persons with cancer. In the case of Pt from carboplatin, the quotient obtained in this work was approximately three times as high as the range found in the literature. Apparently, the data for short-term metal creatinine-1 quotients there is still insufficient for to establish some type of clinical correlation, which could be poorly representative.
The amounts of excreted Pt did not present significant differences between patients with lung cancer and other cancers treated with cisplatin, despite the significant variations in the amount of Pt administered in the drug. In turn, the amounts of excreted Se and As behaved similarly to excreted Pt. Nevertheless, the amount of excreted arsenic was less than that of selenium. Therefore, Pt favors the evacuation of selenium, that is, Pt is more antagonistic to selenium than As, but selenium is also antagonistic to As.
References
-
Madden EF (2003) The Role of Combined Metal Interactions in Metal Carcinogenesis: A Review. Reviews on Environmental Health 18(2): 91-109.
-
Marshall G, Ferreccio C, Yuan Y, Bates MN, Steinnaus C, et al. (2007) Fifty-Year Study of Lung and Bladder Cancer Mortality in Chile Related to Arsenic in Drinking Water. J Natl Cancer Inst 99(12): 920-928.
-
Román DA, Pizarro I, Rivera L, Cámara C, Palacios MA, et al. (2004) An approach to the arsenic status in cardiovascular tissues of patients with coronary heart disease. Hum Exp Toxicol 30(9): 1150-1164.
-
Selinus O (2004) Medical Geology: an emerging speciality. Terrae 1(1): 8-15.
-
Pasetto M, D’Andrea M, Brandes A, Rossi E, Monfardini S (2006) The development of platinum compounds and their possible combination. Critical Reviews in Oncology/Hematology 60(1): 59-75.
-
Selinus O, Alloway JA, Centeno RB, Finkelman RF, Smedley VP (2005) Essential of Medical Geology. Impacts of the Natural Environmental on Public Health (Elsevier, U. S. A., London).
-
Gordon RB (2002) Production residues in copper technological cycles. Resources, Conservation and Recycling 36(2): 87-106.
-
Ferreccio C, Sancha AM (2006) Arsenic exposure and its impact on health in Chile. J Health Popul Nutr 24(2): 164-175.
-
Rahman M (2006) International research on arsenic contamination and health. J Health Popul Nutr 24(2): 123-128.
-
Smith AH, Ercumen A, Juan J, Steinmaus CM (2009) Increased lung cancer risks are similar whether arsenic is ingested or inhaled. J Expo Sci Environ Epidemiol 19(4): 343-348.
-
Smith A, Marshall G, Yuan Y, Ferreccio C, Liaw J, et al. (2006) Increased Mortality from Lung Cancer and Bronchiectasis in Young Adults after Exposure to Arsenic in Utero and in Early Childhood. Environ Health Perspect 114(8): 293-1296.
-
Duker A, Carranza E, Hale M (2005) Arsenic geochemistry and health. Environ Int 31(5): 631- 641.
-
Kelleand L (2007) The resurgence of platinum-based cancer chemoterapy. Nat Rev Cancer 7(8): 573-584.
-
Kalavrouziotis IK, Koukoulakis PH (2009) The Environmental Impact of the Platinum Group Elements (Pt, Pd, Rh) Emitted by the Automobile Catalyst Converters. Water Air Soil Pollut 196: 393-402.
-
Kuo MT, Chen HHW, Song IS, Savaraj N, Ishikawa T (2007) The roles of copper transporters in cisplatin resistance. Cancer Metastasis Rev 26(1): 71-83.
-
Bharti SK, Singh SK (2009) Recent Developments in the Field of Anticancer Metallopharmaceuticals. International Journal of Pharm Tech Research 1: 1406- 1420.
-
Burger H, Loos WJ, Eechoute K, Verweij J, Mathijssen RHJ, et al. (2011) Drug transporters of platinum – based anticancer agents and their clinical significance. Drug Resistance Updates 14(1): 22-34.
-
Heffeter P, Jungwirth U, Jakupec M, Hartinger C, Galanski M, et al. (2008) Resistance against novel anticancer metal compounds: Differences and similarities. Drug Resistance Updates 11(1-2): 1-16.
-
Chen Y, Jungsuwadee P, Vore M, Butterfield DA, St Clair DK (2007) Collateral Damage in Cancer Chemotherapy: oxidative stress in nontargeted tissues. Mol Interv 7(3): 147-156.
-
Rossman TG, Uddin AN (2004) Selenium prevents spontaneous and arsenite-induced mutagenesis. International Congress Series 1275: 173-179.
-
Agusa T, Nomura K, Kunito T, Anan Y, Iwata H, et al. (2008) Interelement relationships and age –related variation of trace element concentrations in liver of striped dolphins (_Stenella coeruleoalba_) from Japanese coastal waters. Marine Pollution Bulletin 57(6-12): 807-815.
-
Spallholz JE, Boylan LM, Rhaman MM (2004) Environmental hypothesis: is poor dietary selenium intake an underlying factor for arsenicosis and cancer in Bangladesh and West Bengal, India? Science of the Total Environment 323(1-3): 21-32.
-
Zeng H, Uthus EO, Combs GF (2005) Mechanistic aspects of the interaction between selenium and arsenic. J Inorg Biochem 99(6): 1269-1274.
-
Pilsner JR, Hall MN, Liu X, Ahsan H, LLievski V, et al. (2011) Associations of Plasma Selenium with Arsenic and Genomic Methylation of Leukocyte DNA in Bangladesh. Environ Health Perspect 119(1): 113-118.
-
Markovic SD, Djacic DS, Cvetkovic DM, Obradovic AD, Zizic JB, et al. (2010) Effects of Acute In vivo Cisplatin and Selenium Treatment on Hematological and Oxidative Stress Parameters in Red Blood Cells of Rats**.** Biol Trace Elem Res 142(3): 660-670.
-
Patrick L (2004) Selenium biochemistry and cancer: a review of the literature. Alternative Medicine Review 9(3): 239-258.
-
Li D, Graef GL, Yee JA, Yan L (2004) Dietary Supplementation with High- Selenium Soy Protein Reduces Pulmonary Metastasis of Melanoma cells in Mice. J Nutr 134(6): 1536-1540.
-
Brinkman M, Buntinx F, Muls E, Zeegers MP (2006) Use of selenium in chemoprevention of bladder cancer. Lancet Oncol 7(9): 766-774.
-
Stone RL, Sood AK, Coleman RL (2010) Collateral damage: toxic effects of targeted antiangiogenic therapies in ovarian cancer. Lancet Oncol 11(5): 265-475.
-
Pani G, Galeotti T, Chiarugi P (2010) Metastasis: cancer cell`s escape from oxidative stress. Cancer Metastasis Rev 29(2): 351-378.
-
Gregus Z, Gyurasics A, Csanaky I (2000) Effects of Arsenic-, Platinum-, and Gold-Containing Drugs on the Disposition of Exogenous Selenium in Rats. Toxicological Sciences 57(1): 22-31.
-
Schrauzer GN (2009) Selenium and selenium- antagonistic elements in nutritional cancer prevention. Crit Rev Biotechnol 29(1): 7-10.
-
Vahter M, Bjorkman L, Goessler W (2007) Concentrations of biomarjers in spot urine samples need adjustment for variation in dilution-Comment on: Distribution of urinary selenium and arsenic among pregnant women exposed to arsenic in drinking water. Environmental Research 104(2): 312-313.
-
Hail N, Cortes M, Drake EN, Spallholz JE (2008) Cancer chemoprevention: A radical perspective. Free Radical Biology & Medicine 45(2): 97-110.
-
Abada P, Howell SB (2010) Regulation of Cisplatin Cytotoxicity by Cu Influx Transporters. Metal-Based Drugs.
-
Chaney SG, Campbell SL, Bassett E, Wu Y (2005) Recognition and processing of cisplatin-and oxaliplatin- DNA adducts. Critical Reviews in Oncology /Hematology 53(1): 3-11.
-
Btasiak J, Kadkubek M, Kowalik J, Romanowicz-Makowska H, Pertynski T (2002) Inhibition of Telomerasa Activity in Endometrial Cancer Cells by Selenium-Cisplatin Conjugate Despite Susppression of its DNA-Damaging Activity by Sodium Ascorbate. Teratog Carcinog Mutagen 22(1): 73-82.
-
Zvereva MI, Shcherbakova DM, Dontsova OA (2010) Telomerase: Structure, Functions, and Activity Regulation. Biochemistry 75(13): 1563-1583.
-
Gerl A, Schierl R (2000) Urinary Excretion of Platinum in Chemoterapy-treated long-term Survivors of Testicular Cancer. Acta Oncologica 39(4): 519-522.
-
Welz B, Melcher M (1985) Decomposition of marine biological tissues for determination of arsenic, selenium and mercury using hydride-generation and cold – vapor atomic absorption spectrometry. Anal Chem 57(2)**:** 427- 431.
-
Rafey M, Lipkowitz M (2007) How Accurate are formulas that calculate creatinina clearance? Nature Clinical Practice 4: 188-189.
-
Banchero P, Saldombide L (2004) Uso de quimioterapia en la insuficiencia renal. Rev Med Uruguay 20(2): 145- 149.
-
Boeniger M, Lowry L, Rosenberg J (1993) Interpretation of Urine Resuts Used to Asses Chemical Exposure with Emphasis on Creatinine Adjustments: A Review. American Industrial Hygiene Association 54(10): 615- 627.
-
Husdan H, Rapoport A (1967) Estimation of Creatinine by the Jaffe Reaction, A comparison of Three Methods. Metabolic-Renal Unit and the departament of Biochemistry, Toronto Western Hospital, and the departament of medicine and of Pathological Chemistry, University of Toronto, Toronto Canada.
-
Barr DB, Wilder LC, Caudill SP, González AJ, Needham LL, et al. (2005) Urinary Creatinine Concentrations in the U.S. Population: Implications for Urinary Biologic Monitoring Measurements. Environ Health Perspect 113(2): 192-200.
-
Valenzuela OL, Borja-Aburto VH, García-Vargas GG, Cruz- González MB, García-Montalvo EA, et al. (2005) Urinary trivalent methylated arsenic species in a population chronically exposed to Inorganic arsenic. Environ Health Perspect 113(3): 250-254.
-
Cavar S, Bosnjak Z, Klapec T, Barisic K, Cepelak I, et al. (2010) Blood selenium, glutathione peroxidase activity and antioxidant supplementation of subjects exposed to arsenic via drinking water. Environmental Toxicology and Pharmacology 29(2): 138-143.
-
Oster O, PellwItz W (1990) The renal excretion of selenium. Biol Trace Elem Res 24(2): 119-146.
-
Zeiner M, Ovari M, Zaray G, Steffan I (2006) Selected urinary metal reference concentrations of the Viennese population-urinary metal reference values (Vienna). J Trace Elem Med Biol 20(4): 240-244.
-
De Mondragón MC, Jaffé WG (1971) Selenio en alimentos y en orina de escolares de diferentes zonas de Venezuela. Separata de Archivos Latinoamericanos de Nutrición 21(2): 185-195.
-
Prince RC, Gailer J, Gunson DE, Turner RJ, George GN, et al. (2007) Strong poison revisited. J Inorg Biochem 101(11-12): 1891-1893.
-
Forina M, Armanino C, Raggio V (2002) Clustering with dendrograms on interpretation variables. Analytica Chimica Acta 454(1): 13-19.
-
Pletnev I, Zernov V (2002) Clasifcation of metal ions according to their complexing properties: a data – driven approach. Analytica Chimica Acta 455(1)**:** 131-142.
-
Yuan Y, Marshall G, Ferreccio C, Steinmaus C, Selvin S, et al. (2007) Acute Myocardial infarction Mortality in Comparison with Lung and Bladder Cancer Mortality in Arsenic-exposed Region II of Chile from 1950 to 2000. Am J of Epidemiol 166(12): 1381-1391.
-
Andrew AS, Burgess JL, Meza MM, Demidenko E, Waugh MG, et al. (2006) Arsenic exposure is associated with decreased DNA repair in vitro and individuals exposed to drinking water arsenic. Environ Health Perspect 114(8): 1193-1198.
-
Ren X, Aleshin M, Jo WJ, Dills R, Kalman DA, et al. (2011) Involvement of N-6 Adenine-Specific DNA Methyltransferase 1 (N6AMT1) in Arsenic Biomethylation and its Role in Arsenic- Induced Toxicity. Environ Health Perspect 119(6): 771-777.
-
Ren X, McHale CM, Skibola CF, Smith AH, Smith MT, et al. (2011) An Emerging Role for Epigenetic Dysregulation in Arsenic Toxicity and Carcinogenesis. Environ. Health Perspect 119(1): 11-19.
-
Bozhkow A, Padalko V, Dlubovskaya V, Menzianova N (2010) Resistance to heavy metal toxicity in organisms under chronic exposure. Indian J Exp Biol 48(7): 679- 696.
-
Mathijssen RHJ, De Jong FA, Loos WJ, Van Der Bol, JM, Verweij J, et al. (2007) Flat-Fixed Dosing Versus Body Surface Area – Based Dosing of Anticancer Drugs in Adults: Does It Make a Difference ? The Oncologist 2007, 12(8): 913-923.
-
Hanekamp JC (2008) Micronutrients, Hormesis and the Aptitude for the Maturation of Regulation. Am J Pharm. & Toxicol 3(1): 144-151.
-
Wu WKK, Sakamoto KM, Milani M, Aldana-Masankgay G, Fan D, et al. (2010) Macroautophagy modulates cellular response to proteasome inhibitors in cancer therapy. Drug Resist Updat 13(3): 87-92.
-
Zachara B, Salak A, Koterska D, Manitius J, Wasowicz W (2004) Selenium and glutathione peroxidases in blood of patients with different stages of chronic renal failure. J Trace Elem Med Biol 17(4): 291-299.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells