A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
Background: Chronic pain is complex and often needs a multi-disciplinary approach focusing on changing cognition (education), movement, and strategies to calm down a hypervigilant nervous system. In the United States (US), multidisciplinary pain programs are expensive, have long waiting periods, not readily accessible and often heavily focused on pharmaceutical interventions and more imaging. Many healthcare systems provide wellness programs, accessible to communities and often inexpensive or free. The primary aim of this study was to determine if a non-pharmacological pain program, delivered by a multidisciplinary team in a wellness program yields positive results. Methods: Over a 2-year span, data was collected on 35 participants in a hospital-based wellness program, focusing on pain neuroscience education (PNE), different forms of exercise and various strategies aimed to calm a hypervigilant nervous system (i.e., relaxation, mindfulness-based-stress reduction, coping skills, etc.). Prior to and immediately following the 4-week program, pain knowledge (Revised Neurophysiology of Pain Questionnaire – rNPQ), pain catastrophization (Pain Catastrophization Scale – PCS) and kinesiophobia (Tampa Scale of Kinesiophobia – TSK) was measured. At the completion of the program, patients were surveyed regarding their experience with the program. Results: At the completion of the study, all formal measures increased significantly – rNPQ (p < 0.001), PCS (p < 0.004) and TSK (p < 0.001), with various patients moving below cut-off scores. Patients highly recommended the class (means score of 8.81 ± 1.69/10), citing learning more about pain and additional ways to treat their pain non-pharmacologically as key takeaways. Conclusion and Relevance: A non-pharmacological, multi-disciplinary pain program, embedded in a wellness program of a healthcare system, yield positive shifts in pain knowledge, pain catastrophization and kinesiophobia, and patients value the program. Delivering such a pain program into existing wellness programs may allow for more local, evidence-based, affordable care for patients with chronic pain within their local communities.
Abbreviations
MCID: Minimal Clinical Important Difference; MDC: Minimal Detectable Change; PCS: Pain Catastrophization Scale; PNE: Pain Neuroscience Education; PT: Physical Therapy; rNPQ: Revised Neurophysiology of Pain Questionnaire; TSK: Tampa Scale of Kinesiophobia; US: United States of America.
Introduction
Epidemiological data shows that approximately one in five people in the world suffer from some form of chronic pain, with nearly seventy percent tied to musculoskeletal disorders [1]. The prevalence of chronic pain is increasing, when compared to data thirty years ago [1, 2]. Chronic pain leads to suffering, loss of productivity, disability, increased healthcare utilization, increased mental and behavioral health issues, and more [2]. To date, most of the data comes from developed countries, and it is anticipated as data emerges from developing countries and regions around the globe, the prevalence and impact of chronic pain may increase [3]. Specific to the United States (US), chronic pain led to the well-documented opioid epidemic, which highlighted the struggle to address chronic pain [4, 5].
In lieu of the opioid epidemic, focus must shift to providing non-pharmacological treatments for chronic pain [6]. Current best-evidence non-pharmacological treatments for chronic pain centers around three distinct, yet intertwined treatment options. First, it’s proposed that treatment must include a cognitive intervention to address maladaptive beliefs including fear-avoidance, pain catastrophizing and more [7]. These cognitive treatments may include pain neuroscience education (PNE), cognitive behavioral therapy, trauma informed care, positive psychology, acceptance and commitment therapy and more [8]. The primary aim of the cognitive intervention is usually center around reduced fear, fear-avoidance and pain catastrophizing, which allows people in pain to move more, which is the second key element of the best-evidence non-pharmacological treatment for chronic pain [7, 8]. Increased movement can be achieved via traditional strategies such as aerobic exercise, resistance exercise, stretches, range of motion, isometric exercises and more [9, 10]. Additionally, non-traditional movement strategies such as yoga, Pilates, Tai Chi, and more can be used to enhance and facilitate movement [11].
Finally, non-pharmacological treatment should also include strategies to decrease sensitization of the nervous system, including breathing exercises, mindfulness-based stress reduction, nutrition, sleep hygiene training, relaxation and more [12, 13]. Calming of the peripheral and central nervous system is currently a key focus in medicine and medical research with a heavy focus on pharmaceutical options such as membrane stabilizers and low-dose anti- depressants [14]. The combination of cognitive treatment, movement and calming of the nervous system provides a comprehensive approach that allows clinicians to truly treat chronic pain from a biopsychosocial approach [15].
Chronic pain is complex, which implies its treatment is complex, and often includes various providers specializing in different aspects of the patient’s pain experience, i.e., a multidisciplinary approach [15, 16]. In the US, multidisciplinary care for chronic pain is significantly lacking, including long waiting lists, high cost, limited regional and local availability and heavily focused on interventional and pharmacological management and imaging [17, 18, 19, 20, 21].
In physical therapy (PT), PNE has emerged as a cognitive intervention for patients with chronic pain to educate patients more about the underlying biological and physiological aspects of their pain experience [22]. Various systematic reviews and meta-analyses have shown the positive effects of PNE for chronic pain including decreased self-reported pain, disability, fear-avoidance, pain catastrophizing, healthcare utilization and increased movement despite pain [23, 24, 25, 26, 27].
By combining PNE with various forms of movement (i.e., aerobic exercise, resistance exercises, etc.), as well as strategies proven to decrease sensitivity of the nervous system (i.e., mindfulness-based stress reduction, breathing, relaxation, etc.), it aligns with current best-evidence treatment for chronic pain, especially from a non-pharmacological perspective [28, 29, 30]. This PNE-approach has since been used as a springboard to educate more healthcare professionals regarding pain science, with the intent to increase pain knowledge and literacy, to allow for a unified approach to patients with chronic pain [31, 32, 33].
In healthcare, education is seen as a cornerstone in changing patient behaviors. To this end, numerous hospitals and healthcare institutions provide community education and classes on various healthcare topics [34, 35]. This may, for example, include education on nutrition, exercise, fall risk, smoking cessation etc.
Many of these educational programs are often built and executed in a wellness program associated with the hospital or healthcare system. To date, very few of these wellness programs focus on pain, especially chronic pain. The primary aim of this study was to determine if a non-pharmacologically focused pain program, delivered by a multidisciplinary team in a wellness program yields positive results, allowing programs such as this to be scaled within wellness programs. A secondary aim was to gain patient perspectives following the program to determine patient preferences and value for such a program.
Methods
Design
This study was a retrospective, mixed-methods, quality improvement study.
Institutional Review and Ethics Approval
Froedtert Holy Family Memorial Medical Center in Wisconsin has a Holy Family Memorial Wellness Center. As patients enroll in various wellness programs, deidentified data is collected by the program prior to and after the various wellness classes to help with quality improvement. Data for this study was obtained from these quality improvement studies, and The Froedtert Health Compliance and Legal Departments and the Medical College of Wisconsin Institutional Review Board deemed this retrospective data collection to be a quality improvement project which is considered non-human subject research and not subject to institutional review board.
Intervention
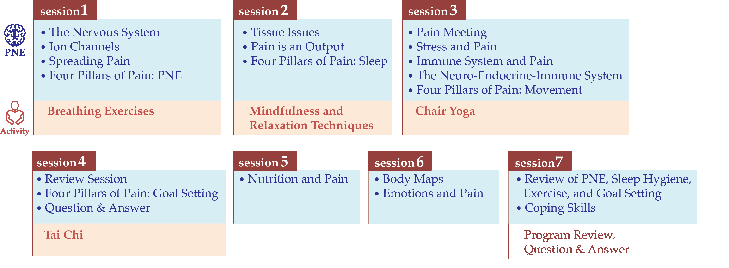
A PT with advanced post-professional education in PNE developed the multidisciplinary pain program to be delivered in the wellness clinic. The program was based on the current best-evidence for the non-pharmacological treatment of chronic pain [15, 22]. The multidisciplinary team included a PT, a licensed counselor, dieticians, a psychologist, exercise physiologist, yoga instructor and personal trainer. Supplemental printed education materials were created by PTs, a nurse, and a dietician. The program consisted of seven sessions over 4 weeks, for a total of twelve hours of instruction (Figure 1). The program consisted of PNE, exercise, goal setting, sleep hygiene, breathing exercises, mindfulness/relaxation techniques, education on nutrition, yoga, and Tai Chi (Figure 1). Classes were held at Holy Family Memorial Wellness Center, part of Froedtert Holy Family Memorial. Education sessions were delivered in a small conference room, and the Tai Chi and yoga sessions were held in an exercise studio room. The PNE content used for this program has been used in various studies focusing on chronic pain [36, 37]. The PNE centered around four key pillars of recovery – education (PNE), sleep (hygiene), movement and goal setting [22, 38]. The PNE covered modern pain science including discussions of peripheral sensitization, central sensitization, biopsychosocial factors associated with pain, threat appraisal of the brain, nociception, stress, and endocrine responses in pain as well as various therapeutic endogenous strategies to ease pain [22, 36, 37, 38, 39].
Participants
Between February 1, 2022, and March 7, 2024, seven cohorts of the class were completed with a convenience sample of 41 participants starting the program. Of the 41 participants that started the program, 35 participants (28 identifying as female, 7 male) provided complete data sets. The average age of participants with complete data sets was 67.57 years (range 52-85 years). Participants were gathered through advertising via social media, signage within the facility, and through facility newsletters, as well as through verbal recommendations from Wellness Center Staff and health care Providers. Participation in this program was completely voluntary. To sign up, participants reviewed and signed a waiver and release for the Wellness Center if they were not already a Wellness Center Member, which included informed consent for the use of their image, likeness, and voice. There were no exclusion criteria for participation in the class. However, participants identified as either a person living with chronic pain or as a family member of someone living with chronic pain. The program (4 weeks; 12 hours) was provided for a fee of $75. Participants had the option of applying for subsidization of this fee through a Wellness Fund, if they cited a financial hardship.
Measures
Participants were assigned a 6-digit code for use when completing outcomes forms, so that no personal information was gathered or shared with the research team. Formal measurements included: Pain knowledge: Pain knowledge was measured using the revised Neurophysiology of Pain Questionnaire (rNPQ). The rNPQ is based on a current pain science text and was used in previous studies measuring the neurophysiology knowledge of patients and health care personnel [40, 41]. The rNPQ is a 12-item test requesting “true,” “false,” or “not sure” answers to statements, with higher scores indicating more correct answers. The questionnaire was adapted similar to a previous study to make it easier for patients to understand (i.e., “nociception” was replaced with “danger messages”). No data is available in patients or healthy controls as to what constitutes a meaningful shift in rNPQ scores. Previous patient studies have reported a mean post-PNE shift of approximately 20-30% [40].
Pain Catastrophization: Pain catastrophization was measured using the Pain Catastrophization Scale (PCS) [42]. The PCS is a self-report questionnaire that assesses inappropriate coping strategies and catastrophic thinking about pain and injury. The PCS has been used in previous pain science studies and demonstrated strong construct validity, reliability and stability [43]. The PCS utilizes a 13-item, 5-point Likert scale with higher scores indicating elevated levels of catastrophizing. Previous studies utilizing the PCS have shown a median score of 18 in healthy individuals, and in patients with pain, the PCS is generally higher [42]. A score of more than 30 out of 52 has been reported as a cut-off score for high levels of catastrophization. In patients with musculoskeletal pain, the minimal detectable change (MDC) is reported as 9.1, and the minimal clinical important difference (MCID) has not been established [42, 43].
Fear of Movement: To evaluate the participant’s pain- related fear of movement and (re)injury the original 17-item Tampa Scale of Kinesiophobia (TSK) was used [44]. Each item is scored on a four-point Likert-type scale that ranges from strongly agree [1] to strongly disagree [4]. Total scores range from 17 to 68, and higher scores indicate more fear of movement and/or (re)injury. In patients with musculoskeletal pain, the MDC for the TSK is reported to be 5.6, and the MCID has not been established [44]. A cut-off score of >37 has been reported as a high level of kinesiophobia.
Participants completed the rNPQ, PCS and TSK prior to the start of class session 1. The outcome measures were completed again, immediately following the conclusion of the last class, session 7, four weeks later. In addition, participants completed a Wellness Center Class Feedback Survey upon completion of the course in week 4, which included open- ended questions requesting write-in answers, closed- ended questions, and a Likert scale question regarding the likelihood of referring friends or family to the program.
Statistical Analysis
The survey data was extracted and entered into Excel spreadsheet. The results of the study were evaluated using SPSS (version 22.0, IBM Corporation). Descriptive statistics of means, standard deviations, and percentages were reported on student group characteristics. Within-group repeated measures and between-group analyses for pain knowledge, pain catastrophizing and kinesiophobia were done using a two-way mixed ANOVA on complete-case analysis. The level of significance was set at p<0.05. Qualitative data was constructed around the main themes. The primary authors analyzed the individual responses to each question and determined the main themes. Each reviewer’s main themes were combined by two reviewers.
Results
Pain Knowledge
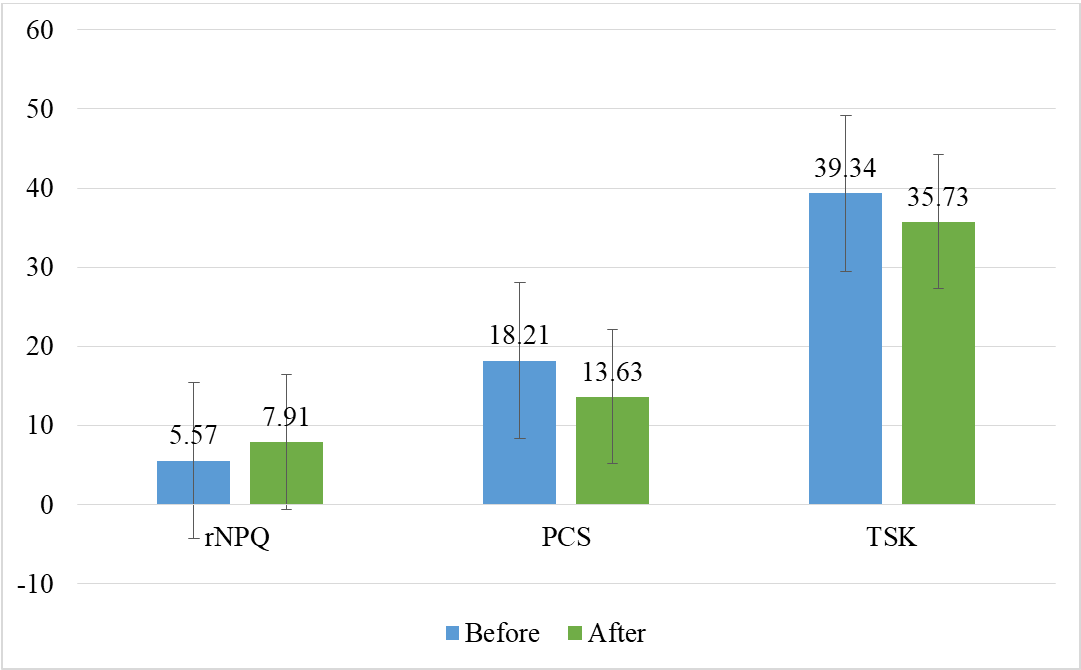
Prior to the wellness program the mean score for the rNPQ was 5.57 (46.4%), and post-program, mean rNPQ scores were 7.91 (65.9%) for an increase of 19.5% (p < 0.001) (Figure 2).
Pain Catastrophization
Prior to the wellness program the mean score for the PCS was 18.21, and post-program, mean PCS scores were 13.63 (p < 0.004) (Figure 2). The mean change did not meet the MDC for the PCS. Prior to the program, 8 patients (22.9%) exceeded the cut-off score for a high PCS score (>30), whereas 5 exceeded the cut-off at the conclusion of the program (14.3%).
Kinesiophobia
Prior to the wellness program the mean score for the TSK was 39.34, and post-program, mean TSK scores were 35.73 (p < 0.001) (Figure 2). The mean change did not meet the MDC for the TSK. Prior to the program, 20 patients (57.1%) exceeded the cut-off score for a high TSK score (>37), whereas 12 exceeded the cut-off at the conclusion of the program (34.3%).
Patient Experience
On a Likert scale (0 not likely at all, 10 very likely) of how likely they are to recommend this class to a friend or family member, patients reported a means score of 8.81 (± 1.69).
Biggest take-away from the program?
All patients (n = 35) reported that the pace of the material was “appropriate” (100%) and the amount of material was “appropriate” (100%). Table 1 showcases the main themes extracted from patient feedback at completion of the program.
The importance of exercise and movement with graded exposure and pacing Learning more about how pain works and increasing understanding of pain Lots of ways to help pain, i.e., sleep, exercise, nutrition Topics and/or activities they found most beneficial?
Diet, nutrition and pain Lots of ways to help pain, including the 4 pillars Everything – a lot of good information Tai Chi and Chair yoga What topics and/or activities did they not like and why? Chair yoga Sitting a lot If they were to recommend this class to a friend, what would they say to them? You learn a lot about pain
- Lots of things you can do for your pain
- Was very helpful and gives hope
- How can we improve your experience?
- Keep as is – not too many changes
- Shorter classes
- Add information on medications
Table 1: Patient feedback after completion of the program.
Discussion
The results from this study show that a non- pharmacological, multi-disciplinary pain program, embedded in a wellness program, yield positive shifts in pain knowledge, pain catastrophization and kinesiophobia. From a patient perspective, the program was seen of value, allowing increased knowledge and understanding of pain, as well as non-pharmacological ways to help their pain and disability.
In this study, the results related to pain knowledge, pain catastrophization and kinesiophobia mirror previous PNE study results [36, 37, 40, 45, 46]. A growing number of studies show that patients, in different clinical settings and dealing with different chronic pain diagnoses, increase their knowledge of pain after receiving PNE. The 19% increase in pain knowledge is in line with other studies [40]. This increase in pain knowledge has been postulated to be a key part of the reconceptualization of pain in patients, allowing for a decrease in fear, especially related to movement, as well as provide hope, which is reflected in a decrease in catastrophization [46]. Both these shifts were also observed in this study, which underscores the fact that a non- pharmacological, PNE-based, multi-disciplinary study can be a viable addition to healthcare systems wellness programs. The quantitative results from this study are supported by the qualitative data, whereby patients reported the increase understanding of pain as the primary benefit of the program. It is well documented that high levels of fear, fear-avoidance and kinesiophobia powerfully predict pain behaviors, including limiting much-needed movement [7]. The current evidence strongly favors various forms of movement and exercise as a key part of improving disability, self-efficacy and pain relief. High levels of fear, fear-avoidance and kinesiophobia hinder a patient’s willingness to move, and normalizing these maladaptive cognitions are often needed prior to, or in combination of movement-based therapies [15, 45]. In this study, the combination of education and various movement strategies were key to the different results. In addition to altering cognitions and increased movement, additional strategies of the program (i.e., nutrition, coping skills, breathing, relaxation, mindfulness-based stress reduction), provided the much-needed third component of a comprehensive pain program – strategies to calm down a hypervigilant nervous system [12]. Adding these strategies not only aligned with current best evidence but were also valued by patients to teach them ways to help their pain, thus increasing self-efficacy.
In the current rehabilitation environment in the US, group-therapy remains a struggle, primarily due to reimbursement. In outpatient, orthopedic and private practice, reimbursement is tied to fee for service and heavily weighted towards one-on-one care, with limited ability to develop, implement and delivery group therapy, including group therapy sessions for chronic pain. Most group therapy sessions for chronic pain are often found in federally funded systems (i.e., Department of Veteran’s Affairs, Department of Defense) [47, 48], or large healthcare systems that add pain programs which can be offset financially with funded procedural medical interventions (i.e., injections, nerve- ablations), and imaging studies. In the US multi-disciplinary care programs for chronic pain are expensive, limited in availability, not readily available in local communities and often have long waiting lists [17, 18, 19, 20, 21]. The results of this pilot study show that a community-based program can be developed, implemented and meet patient needs when placed within already-available programs, such as wellness programs. Given the global epidemic of chronic pain, it is time for hospitals and healthcare systems to expand wellness programs to not only address well-known and well- understood issues such as obesity, smoking cessation and fall risk, but also chronic pain. In this study, the most a patient would have paid was $75 for the 7-session program, averaging just over $10/session, which is significantly less than the current average outpatient physical therapy co-pay of nearly $40/visit [49], thus alleviating an additional burden for patients and access to a much-needed, non-pharmacological program for chronic pain. With approximately 70-80 million American suffering from chronic pain [18], and the vast healthcare system in the US, adding a multi-disciplinary, non- pharmacological program that serves the local community and is cost-effective, to existing wellness programs, may be a powerful way to meet patient needs.
The study contains various limitations. First, as a retrospective, quality control study, various potentially key data sets were missing and would have added to the study, i.e., self-reported pain ratings, disability, patient demographic information, etc. Tracking self-reported pain and disability would have allowed insight to determine if the changes in pain knowledge, pain catastrophization and kinesiophobia were correlated to shifting those two key variables which typically are used to determine success of musculoskeletal interventions. Second, the results obtained for this study were only gathered at the conclusion of the study, with no longer-term follow-up available. Various behavioral studies have shown that true behavioral change occurs after six months, and future studies should at minimum track post- intervention data for 6 months.
Conclusion
A non-pharmacological, multi-disciplinary pain program, embedded in a wellness program of a healthcare system, yield positive shifts in pain knowledge, pain catastrophization and kinesiophobia and patients valued the program to learn more about pain and find additional, non-pharmacological strategies to ease their pain. Building and executing such a pain program into existing wellness programs may allow for more local, evidence-based, affordable care for patients with chronic pain within their local communities.
References
-
(2015) Global Burden of Disease Study, C., Global, regional and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386(9995): 743-800.
-
Nahin RL, Feinberg T, Kapos FP, Terman GW (2023) Estimated Rates of Incident and Persistent Chronic Pain Among US Adults, 2019-2020. JAMA Netw Open 6(5): e2313563.
-
Wu A, March L (2020) Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med 8(6): 299.
-
Bryson EO (2018) The opioid epidemic and the current prevalence of substance use disorder in anesthesiologists. Curr Opin Anaesthesiol 31(3): 388-392.
-
Wilkerson RG, Kim HK, Windsor TA (2016) The Opioid Epidemic in the United States. Emerg Med Clin North Am 34(2): 1-23.
-
Agarwal V, Louw A, Puentedura EJ (2020) Physician- Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report. Int J Environ Res Public Health 17(9).
-
Vlaeyen JW, Crombez G, Linton SJ (2016) The fear- avoidance model of pain. Pain 157(8): 1588-1589.
-
Main CJ, Simon CB, Beneciuk JM, Greco CM, George SZ, et al. (2023) The Psychologically Informed Practice Consultation Roadmap: A Clinical Implementation Strategy. Phys TheR 103(7).
-
Naugle KM, Fillingim RB, Riley JL (2012) 3rd, A meta- analytic review of the hypoalgesic effects of exercise. The journal of pain: official journal of the American Pain Society 13(12): 1139-1150.
-
Wewege MA, Jones MD (2021) Exercise-Induced Hypoalgesia in Healthy Individuals and People With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. J Pain 22(1): 21-31.
-
Seshadri A, Adaji A, Orth SS, Singh B, Clark MM, et al. (2020) Exercise, Yoga, and Tai Chi for Treatment of Major Depressive Disorder in Outpatient Settings: A Systematic Review and Meta-Analysis. Prim Care Companion CNS Disord 23(1).
-
Meeus M, Nijs J, Vanderheiden T, Baert I, Descheemaeker F, et al. (2015) The effect of relaxation therapy on autonomic functioning, symptoms and daily functioning, in patients with chronic fatigue syndrome or fibromyalgia: a systematic review. Clinical rehabilitation 29(3): 221-233.
-
Kim SH, Schneider SM, Bevans M, Kravitz L, Mermier C, et al. (2013) PTSD symptom reduction with mindfulness- based stretching and deep breathing exercise: randomized controlled clinical trial of efficacy. J Clin Endocrinol Metab 98(7): 2984-2992.
-
Cooper TE, Derry S, Wiffen PJ, Moore RA (2017) Gabapentin for fibromyalgia pain in adults. Cochrane Database Syst Rev 1: CD012188.
-
Zimney K, Van Bogaert W, Louw A (2023) The Biology of Chronic Pain and Its Implications for Pain Neuroscience Education: State of the Art. J Clin Med 12(13).
-
Nijs J, Lahousse A, Fernández-de-Las-Peñas C, Madeleine P, Fontaine C, et al. (2023) Towards precision pain medicine for pain after cancer: the Cancer Pain Phenotyping Network multidisciplinary international guidelines for pain phenotyping using nociplastic pain criteria. Br J Anaesth 130(5): 611-621.
-
Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJEM, Ostelo RWJG, et al. (2015) Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ 350: h444.
-
Nahin RL (2022) Use of Multimodal Multidisciplinary Pain Management in the US. JAMA Netw Open 5(11): e2240620.
-
Castel LD, Freburger JK, Holmes GM, Scheinman RP, Jackman AM, et al. (2009) Spine and pain clinics serving North Carolina patients with back and neck pain: what do they do, and are they multidisciplinary? Spine 34(6): 615-622.
-
Choiniere M, Dion D, Peng P, Banner R, Barton PM, et al. (2010) The Canadian STOP-PAIN project - Part 1: Who are the patients on the waitlists of multidisciplinary pain treatment facilities? Canadian journal of anaesthesia 57(6): 539-548.
-
Guerriere DN, Dion D, Peng P, Banner R, Barton PM, et al. (2010) The Canadian STOP-PAIN project - Part 2: What is the cost of pain for patients on waitlists of multidisciplinary pain treatment facilities? Canadian journal of anaesthesia 57(6): 549-558.
-
Louw A, Riera-Gilley V (2024) Pain Neuroscience Education: Teaching People About Pain. J Pain Palliat Care Pharmacother 38(3): 292-301.
-
Lin LH, Lin TY, Chang KV, Wu WT, Oezcakar L (2024) Pain neuroscience education for reducing pain and kinesiophobia in patients with chronic neck pain: A systematic review and meta-analysis of randomized controlled trials. Eur J Pain 28(2): 231-243.
-
Shin S, Kim H (2023) Carryover Effects of Pain Neuroscience Education on Patients with Chronic Lower Back Pain: A Systematic Review and Meta-Analysis. Medicina (Kaunas) 59(7): 1268.
-
Suso-Marti L, Cuenca-Martínez F, Alba-Quesada P, Muñoz-Alarcos V, Herranz-Gómez A, et al. (2022) Effectiveness of Pain Neuroscience Education in Patients with Fibromyalgia: A Systematic Review and Meta- Analysis. Pain Med 23(11): 1837-1850.
-
Siddall B, Ram A, Jones MD, Booth J, Perriman D, et al. (2021) Short-term impact of combining pain neuroscience education with exercise for chronic musculoskeletal pain: a systematic review and meta- analysis. Pain.
-
Romm MJ, Ahn S, Fiebert I, Cahalin LP (2021) A Meta- Analysis of Therapeutic Pain Neuroscience Education, Using Dosage and Treatment Format as Moderator Variables. Pain Pract 21(3): 366-380.
-
Wood L, Hendrick PA (2019) A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-term outcomes of pain and disability. Eur J Pain 23(2): 234-249.
-
Marris D, Theophanous K, Cabezon P, Dunlap Z, Donaldson M (2021) The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: A systematic review and meta-analysis of randomized controlled trials. Physiother Theory Pract 37(4): 461-472.
-
Louw A, Sluka KA, Nijs J, Courtney CA, Zimney K (2021) Revisiting the Provision of Pain Neuroscience Education: An Adjunct Intervention for Patients but a Primary Focus of Clinician Education. J Orthop Sports Phys Ther 51(2): 57-59.
-
Louw A, Vogsland R, Marth L, Marshall P, Cox T, et al. (2019) Interdisciplinary Pain Neuroscience Continuing Education in the Veterans Affairs. Clin J Pain 35(11): 901-907.
-
Louw A, Schmieder A, Peppin E, Farrell K, Zimney K, et al. (2020) Can a pain neuroscience education lecture alter treatment choices for chronic pain in physician assistant students? Psychological Disorders and Research 3(2): 1-5.
-
Zimney K, Louw A, Johnson J, Peppers S, Farrell K (2018) Effects of Pain Science Education on Physician Assistant Students Understanding of Pain and Attitudes and Beliefs about Pain. South Dakota Medical Journal 71(11): 506-511.
-
Upton A, Spirou D, Craig M, Saul N, Winmill O, et al. (2025) Health literacy and obesity: A systematic scoping review. Obes Rev: e13904.
-
Ionescu R, Allen LA, Breathett K, Fowler BK, Jackson EA, et al. (2025) Health Literacy in Heart Failure: A Review of the Gaps and Challenges. JACC Adv 4(3): 101608.
-
Louw A, Zimney K, Puentedura E (2016) Retention of pain neuroscience knowledge: a multi-centre trial. New Zealand Journal of Physiotherapy 44(2): 91-96.
-
Louw A, Puentedura E (2014) Therapeutic Neuroscience Education, Pain, Physiotherapy and the Pain Neuromatrix. International Journal of Health Sciences 2(3): 33-45.
-
Louw A, Zimney K, O’Hotto C, Hilton S (2016) The clinical application of teaching people about pain. Physiotherapy Theory and Practice 32(5): 385-395.
-
Louw A (2013) Why Do I Hurt? A Neuroscience Approach to Pain. Minneapolis: OPTP.
-
Moseley L (2003) Unraveling the barriers to reconceptualization of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. The journal of pain : official journal of the American Pain Society 4(4): 184-189.
-
Catley MJ, O’Connell NE, Moseley GL (2013) How Good Is the Neurophysiology of Pain Questionnaire? A Rasch Analysis of Psychometric Properties. The journal of pain: official journal of the American Pain Society 14(8): 818- 827.
-
Sullivan MJ, Bishop SR, Pivik J (1995) The pain catastrophizing scale: development and validation. Psychological assessment 7(4): 524.
-
Osman A, Barrios FX, Gutierrez PM, Kopper BA, Merrifield T, et al. (2000) The Pain Catastrophizing Scale: further psychometric evaluation with adult samples. Journal of behavioral medicine 23(4): 351-365.
-
Hapidou EG, O’Brien MA, Pierrynowski MR, de Las Heras E, Patel M, et al. (2012) Fear and Avoidance of Movement in People with Chronic Pain: Psychometric Properties of the 11-Item Tampa Scale for Kinesiophobia (TSK-11). Physiother Can 64(3): 235-241.
-
Meeus M, Nijs J, Van Oosterwijck JPT, Alsenoy VV, Truijen S (2010) Pain Physiology Education Improves Pain Beliefs in Patients with Chronic Fatigue Syndrome Compared with Pacing and Self-Management Education: A Double-Blind Randomized Controlled Trial. Arch Phys Med Rehabil 91(8): 1153-1159.
-
Louw A, Zimney K, Puentedura EJ, Diener I (2016) The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiotherapy Theory and Practice 32(5): 1-24.
-
Benedict TM, Nitz AJ, Abt JP, Louw A (2021) Development of a pain neuroscience education program for post- traumatic stress disorder and pain. Physiother Theory Pract 37(4): 473-485.
-
Benedict TM, Nitz AJ, Gambrel MK, Louw A (2024) Pain neuroscience education improves post-traumatic stress disorder, disability, and pain self-efficacy in veterans and service members with chronic low back pain: Preliminary results from a randomized controlled trial with 12-month follow-up. Mil Psychol 36(4): 376-392.
-
Louw A, Sumner K, Bruzzone H (2023) All’s well that end’s well in physical therapy? The relative importance of Copays in patients with low back pain attending physical therapy. International journal of reserach in physical medicine and rehabilitation 1(1): 1-6.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial
- PNF-Augumented Balance Training Using Balance Beam and Balance Board: A Controlled Trial Assessing Walking Speed Outcomes in Stroke Patients