Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions
This study was a comparative single-dose, open-label, randomized, two-treatment, two-sequence, four-period, fullreplicate crossover, in-vivo study to determine the bioequivalence of Easyrect 100 mg Tablets (Avanafil100 mg) manufactured by Egyptian Group for Pharmaceutical Industries for Zeta Pharm for Pharmaceutical Industries versus Spedra® 100 mg Tablets(Avanafil100 mg) manufactured by Menarini International Operations Luxembourg S.A. after a single dose administration given to healthy adult volunteers under fasting conditions. The subjects who conform to the study entry criteria were dosed according to a randomization schedule. The study was designed and completed according to the good clinical and laboratory practices.
Hesham AEliwa1* and AA Alaa Eldin2
Science and Technology (MUST), Egypt
dr.heshamab@gmail.com to the good clinical and laboratory practices.
Introduction
To investigate single-dose bioequivalence of Easyrect 100 mg Tablets manufactured by Egyptian Group for Pharmaceutical Industries for Zeta Pharm for Pharmaceutical Industries (Avanafil100 mg) and Spedra® 100 mg Tablets manufactured by Menarini International Operations Luxembourg S.A. (Avanafil100 mg) given to healthy adult males under fasting conditions [1]. For the ln-transformed ratio (test product/reference product) for the bioequivalence parameters (Cmax, AUC0-t, and AUC0- ∞) while other pharmacokinetic parameters of ke, t1/2, Tmax, and (AUCt/AUC∞)% were reported [2]. The influence of sequence, product, and period effect were tested by ANOVA [3, 4].
The study was carried out by the Makin Research Center (MRC), Nasr city, Cairo, Egypt. This is a submission to obtain registration for a new chemical entity avanafil tablets (Spedra) with proposed indications for the treatment of erectile dysfunction in adult men [5].
Dosage Forms and Strengths
The submission proposes registration of the following dosage forms and strengths:
- Spedra (avanafil) 50 mg tablets blister package
- Spedra (avanafil) 100 mg tablets blister package
- Spedra (avanafil) 200 mg tablets blister package
Methods and Procedures
Study Drug Administration: On study day 1 of each study period, the study drugs were administered according to a randomization plan. The administration of the study drugs was documented in the drug administration form.
- Treatment A: One Easyrect 100 mg Tablets (Avanafil100 mg) taken with 240 mL of water (measured with a 100-mL cylinder) at room temperature.
- Treatment B: One Spedra® 100 mg Tablets (Avanafil100 mg) taken with 240 mL of water (measured with a 100-mL cylinder) at room temperature.
- Prior and Concurrent Medication: According to the study’s protocol, no prescription medication or nonprescription medication was to be taken starting one week before the first study’s drugs administration until the end of the study (collection of the last sample of period II) [6].
- Special Precautions to be taken: Co-administration of avanafil with any form of organic nitrate is contraindicated due to the potentiation of hypotension. Nitrates should not be administered to subjects for at least 12 hours after the last dose of avanafil and should be administered under close medical supervision with appropriate hemodynamic monitoring [7].
Dietary Restrictions, Standardized Diet and Fluid Intake
No consumption of alcohol was permitted for the subjects 48 hours prior to the study’s drugs administration until the collection of the last sample of the respective study period. No consumption of any beverages or foods containing methylxanthines, e.g., caffeine (coffee, tea, cola, cocoa, chocolate, etc.) was Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134.
permitted for the subjects 48 hours prior to the study’s drugs administration until the collection of last blood sample of the respective study period [8].
In addition, the consumption of any beverages or foods containing grapefruit was prohibited one week before the first study’s drugs administration and throughout the entire study.
Food and fluid intake were identical in both study periods, starting from the dinner served 10 hours before study’s drugs administration on study day 1until the end of confinement. Meals were standardized in composition and amount in both periods. The subjects were not allowed to consume any additional beverages or foodstuffs other than those provided throughout the period of confinement [9].
No excessive fluid intake (>150 mL of water per hour) was allowed from 1to10 hours prior to dosing. From one hour before study’s drugs administration to two hours after, no fluid intake was allowed apart from the 240 mL of water used for the administration. Following the four hours, subjects were allowed to drink water but not exceeding 150 mL per hour.
Collection and Handling of Blood Samples for Analysis
In the morning of study day 1of each study period and before study’s drugs administration, a cannula was inserted into the subject’s forearm vein and it remained there until the last blood sample was collected [10].
The volume of blood taken for the determination of Avanafil in plasma was 5 mL per sample. The following blood samples for the analysis of Avanafil in plasma were collected: at the following intervals: 0, 5 min, 10 min, 0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 24 & 48 hours after dosing. The number of blood collections for drug analysis was 17 samples in each study period [11].
Blood samples were collected into tubes containing heparin as an anticoagulant slightly shaken, and centrifuged at approximately 3500 rpm for 10 minutes [12]. After centrifugation, plasma samples were transferred directly into a 5-mL plastic tube. These samples were immediately stored at the study site in an ultradeep freezer at a nominal temperature of -80 oC.
The label of the collecting tubes had the study’s code number, subject number, study period, and the Copyright© Hesham AEliwa and AA Alaa Eldin.
designated sample number. It did not contain information that would allow identifying the given treatment. This assured that the analysts at MRC analyzed the samples blindly. The total amount of blood loss during the whole study (including blood for laboratory tests) did not exceed 350 mL in a period of one month. All procedures involving handling of blood samples will be documented [13].
Bio-analytical Drug Determination Methodology
A high performance liquid chromatographic (Shimadzu Prominence with rack changer) method coupled with mass spectrometric detection (LC-MS/MS) was developed, optimized and validated at MRC laboratories for the determination of Avanafil in human plasma. The method was fully validated according to the “FDA Bioanalytical Method Validation Guidelines 2003”. Linearity of the assay method was verified within the concentration range of 65 - 7500 ng/mL. All results were within the acceptance criteria as stated in the recommended guidelines. The mean recovery of Avanafil was 102.82% at 65 ng/mL, and 91.91% at 7500 ng/ml. The described method is proved to be sensitive, accurate and reproducible with lower limit of quantification of 65 ng/mL for Avanafil [14].
Data Quality Assurance
The MRC’s quality assurance procedures were implemented to assure the built-in quality system. All data entry was done by the trained staff of MRC and checked by the QAU personnel. All procedures were performed according to the internal MRC-approved SOPs with the results being documented and reported. Deliberately, all in-use manuals were archived by the QAU.
All sheets used to document results were issued and approved by the QAU serially, and ultimately reserved in the QAU.
Logbooks were audited internally by the MRC QAU personnel during the internal audit of both the clinical part and the analytical part of the study. All laboratory (clinical and analytical) results were checked and their source documents retained by the QAU [15]. Source document verification was done by the QAU after each data entry. Instrumental outputs after calculations were checked by the QAU personnel. Necessary actions were taken and corrective and/or preventive measures were recommended. A report after each audit period was Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134.
delivered to the MRC management. Report of audits were followed up and reserved by the QAU. The QAU implements an internal quality system to keep all essential records related to the study guaranteeing the appropriate authorized direct access and traceability of data with utmost confidentiality [16].
All audit trails were enabled within the operated software. After the study report preparation, the QAU audited the report and released its quality assurance statement, which evidenced each audit task [17].
Pharmacokinetic Calculations
The pharmacokinetic parameters of Avanafil were estimated using standard non-compartmental methods. The maximal plasma concentration was taken directly from the measured data. The area under the plasma concentration–time curve (AUCt) was calculated from measured datapoints from the time of administration to the time of last quantifiable concentration (Clast) by the linear trapezoidal rule.
The area under the plasma concentration–time curve extrapolated to infinity (AUC∞) was calculated according to the following formula:
AUC0-∞ = AUC0-t + Clast / [ln (2)/t½], where Clast is the last quantifiable concentration. The ratio AUC0- t/AUC0/-∞ as a percent was determined as an indicator for the adequacy of sampling time.
The elimination half-life t½ was calculated as t½ = ln (2)/(-b) where b was obtained as the slope of the linear regression of the ln-transformed plasma concentrations versus time in the terminal period of the plasma curve.
Statistical Analysis
Statistical analysis was performed using a Kinetica version 5.1 (Thermo Scientific, USA).
Reagents, Chemicals & Standards
- Avanafil working standard
- Ezogabine working standard
- Water for chromatography (Sharlau, Spain)
- Acetonitrile, HPLC grade (Sigma Aldrich Chemie GmbH, Steinheim-Germany)
- Ammonium Formate, Dichloromethane, (Sigma Aldrich Chemie GmbH, Steinheim-Germany)
- Blank plasma obtained from the Holding Company for Biological Products & Vaccines (VACSERA), Giza, Egypt.
Copyright© Hesham AEliwa and AA Alaa Eldin.
Statistical Results
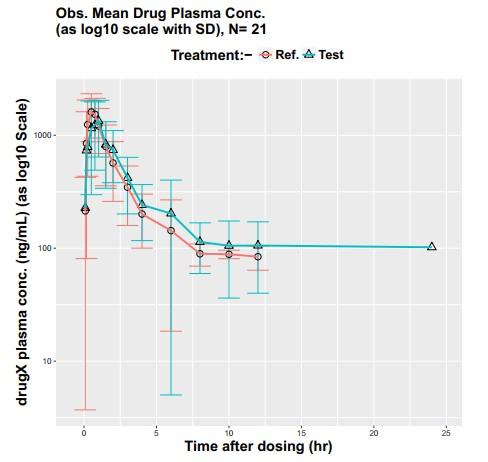
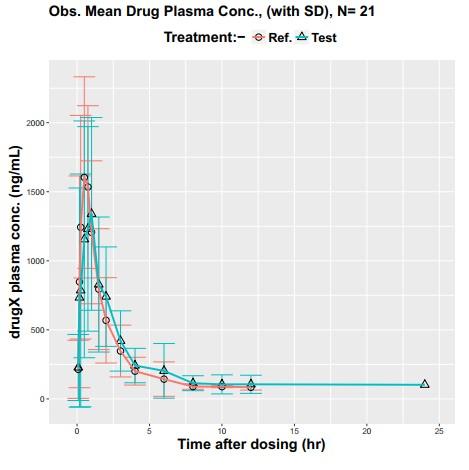
Plasma Concentration-Time Profiles for Each Volunteer
| Test 1st time | Test 2nd time | Reference 1st time | Reference 2nd time | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time (h.) | Dosage Form | Dosage Form | Dosage form | Dosage form | |||||||||||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||||||||||
| 0 | - | - | - | - | - | - | - | - | |||||||
| 0.08333 | 121.08 | 18.55 | 312.38 | 306.11 | 254.24 | 310.16 | 181.86 | 78.4104 | |||||||
| 0.16667 | 569.59 | 733.38 | 1020.3 | 861.78 | 745.98 | 805.23 | 943.441 | 740.035 | |||||||
| 0.25 | 727.19 | 811.81 | 847.89 | 898.53 | 1071.22 | 738.78 | 1405.95 | 859.106 | |||||||
| 0.5 | 1190.91 | 951.12 | 1119.71 | 778.2 | 1660.35 | 683.43 | 1544.44 | 787.087 | |||||||
| 0.75 | 1062.53 | 800.5 | 1390.97 | 658.9 | 1463.24 | 491.45 | 1604.9 | 677.476 | |||||||
| 1 | 1416.05 | 511.97 | 1263.14 | 850.72 | 1188.29 | 550.87 | 1224.1 | 494.923 | |||||||
| 1.5 | 927.33 | 559.95 | 723.85 | 388.32 | 800.36 | 463.7 | 788.952 | 422.62 | |||||||
| 2 | 867.95 | 426.71 | 606.4 | 210.65 | 560.55 | 308.5 | 576.79 | 316.955 | |||||||
| 3 | 500.91 | 242.32 | 338.05 | 158.02 | 344.6 | 188 | 348.737 | 192.337 | |||||||
| 4 | 267.85 | 126.63 | 213.61 | 119.26 | 204.48 | 106.38 | 196.863 | 97.4729 | |||||||
| 6 | 209.02 | 211.91 | 195.11 | 186.34 | 120.99 | 53.49 | 167.15 | 172.089 | |||||||
| 8 | 116.85 | 61.01 | 106.92 | 39.45 | 88.23 | 23.87 | 90.7 | 14.9401 | |||||||
| 10 | 117.58 | 80.38 | 74.15 | 0.21 | 85.1 | 12.16 | 89.76 | 6.58696 | |||||||
| 12 | 115.93 | 80.92 | 85 | 25.46 | 88.17 | 24.9 | 78.1 | 16.8291 | |||||||
| 24 | 102 | - | - | - | - | - | - | - | |||||||
| 48 | - | - | - | - | - | - | - | - |
Table 1: Plasma concentration Average ± SD (ng/mL) of Avanafil following oral administration of Treatment (A) test Table 1: Plasm
| Pharmacokinetic Parameter | Treatment (Mean) | |||
|---|---|---|---|---|
| C (ng/ml) max | T t P d t 1871.62 | R f P d t 1986.02 | ||
| T (h) median max | 0.88 | 0.50 | ||
| AUC (ng.h/ml) 0-t | 3237.21 | 3001.36 | ||
| AUC (ng.h/ml) 0-inf | 3572.64 | 3204.00 | ||
| t 1/2 | 1.94 | 1.64 | ||
| K elimination | 0.49 | 0.60 |
Table 2: Pharmacokinetic Parameter.
| Point Estimate | Lower Confidence Limit | Upper Confidence Limit | ||||||
|---|---|---|---|---|---|---|---|---|
| C (ng/mL) max | 93.72% | 83.89% | 104.69% | |||||
| AUC (ng.hr/mL) t | 108.11% | 95.88% | 121.90% | |||||
| AUC (ng.hr/mL) 0-∞ | 110.74% | 98.93% | 123.96% |
Table 3: 90% Confidence Interval & Point Estimate for Cmax, AUC0-t & AUC0-∞.
Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134.
Copyright© Hesham AEliwa and AA Alaa Eldin.
Statistical Program
| CV Within- Treatment | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect | DF | Sum of Squares | Mean Square | F Value | Pr > F | Significance | |||||||||||||||
| Formula | 1.00 | 0.09 | 0.09 | 0.96 | 0.33 | Non-Significant | . | ||||||||||||||
| Period | 3.00 | 0.02 | 0.01 | 0.07 | 0.97 | Non-Significant | . | ||||||||||||||
| Subject(Sequence) | 19.00 | 1.97 | 0.10 | 1.13 | 0.35 | Non-Significant | . | ||||||||||||||
| (Within) Mean Square Error | 59.00 | 5.43 | 0.09 | . | . | -- | 31.04% | ||||||||||||||
| Sequence | 1.00 | 0.01 | 0.01 | 0.07 | 0.79 | Non-Significant | . |
Table 4: ANOVA table with Confidence Interval for Ln Cmax.
| CV Within- Treatment | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect | DF | Sum of Squares | Mean Square | F Value | Pr > F | Significance | |||||||||||||||
| Formula | 1.00 | 0.13 | 0.13 | 1.18 | 0.28 | Non-Significant | . | ||||||||||||||
| Period | 3.00 | 0.73 | 0.24 | 2.24 | 0.09 | Non-Significant | . | ||||||||||||||
| Subject(Sequence) | 19.00 | 7.80 | 0.41 | 3.80 | <.0001 | Significant | . | ||||||||||||||
| (Within) Mean Square Error | 59.00 | 6.38 | 0.11 | . | . | -- | 33.78% | ||||||||||||||
| Sequence | 1.00 | 0.58 | 0.58 | 1.42 | 0.25 | Non-Significant | . |
Table 5: ANOVA table with Confidence Interval for Ln AUCt.
Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134.
Copyright© Hesham AEliwa and AA Alaa Eldin.
- Error
- 59.00
- 5.63
- 0.10
- .
- .
- --
- 31.65%
- Sequence
- 1.00
- 0.49
- 0.49
- 1.12
- 0.30
- Non-Significant
- .
Table 6: ANOVA table with Confidence Interval for Ln AUCinf.
| Effect | DF | Sum of Squares | Mean Square | F Value | Pr > F | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Formula | 1 | 0.334821 | 0.334821 | 3.73362 | 0.06838 | ||||||||||||
| Period | 1 | 0.43006 | 0.43006 | 4.79563 | 0.04121 | ||||||||||||
| Subject(Sequence) | 19 | 2.01563 | 0.106086 | 1.18297 | 0.359 NS | ||||||||||||
| (Within) Mean Square Error | 19 | 1.70387 | 0.089677 | . | . | ||||||||||||
| Sequence | 1 | 0.040923 | 0.040923 | 0.456332 | 0.5075 |
Table 7: ANOVA table with Confidence Interval for Tmax.
Conclusions
| What Is Already Known About This Subject | ? |
|---|
It is known about this subject comparing the activity of the active ingredient of the drugs to ensure the effectiveness of same active ingredient.
Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134.
| What This Study Adds? |
|---|
The study ensures the same level of drug alternatives for the safety of the patient. This study is comparing two different drugs but the same active ingredient, and to ensure the same level of alternatives to medicine. For Example: Augmentin (amoxicillin and clavulanic acid) and Megamox (amoxicillin and clavulanic acid), differ in trade name but same active ingredient.
The Test product, Easyrect 100 mg Tablets manufactured by Egyptian Group for Pharmaceutical Industries for Zeta Pharm for Pharmaceutical Industries is bioequivalent to the reference drug, Spedra® 100 mg The Test product, Easyrect 100 mg Tablets manufactured by Egyptian Group for Pharmaceutical Industries for Zeta Pharm for Pharmaceutical Industries is bioequivalent to the reference drug, Spedra® 100 mg Tablets manufactured by Menarini International Operations Luxembourg S.A.
References
-
Schuirmann DJ (1987) A Comparison of the Two One- Sided Tests Procedure and the Power Approach fo Assessing the Equivalence of Average Bioavailability', Journal of Pharmacokinetics and Biopharmaceutics 15(6): 657-680. Copyright© Hesham AEliwa and AA Alaa Eldin.
-
Boix-Montanes A (2011) Relevance of equivalence assessment of topical products based on the dermatopharmacokinetics approach, European Journal of Pharmaceutical Sciences 42 (3): 173-179.
-
Skelly JP (2010) A history of biopharmaceutics in the food and drug administration 1968–1993, The American Association of Pharmaceutical Scientists Journal 12(1): 44-50.
-
FDA (2011) CFR-Code of Federal Regulations Title 21- Part 320 Bioavailability and bioequivalence requirement. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER).
-
FDA (1992) Guidance for industry, Statistical procedures for bioequivalence studies using a standard two-treatment crossover design. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER), July 1992.
-
FDA (1996) Guidance for industry, E6 Good Clinical Practice: Consolidated Guidance. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER).
-
FDA (2000) Guidance for industry, Waiver of In vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER).
-
FDA (2001a) Guidance for industry, Statistical approaches to establishing bioequivalence. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER), January 2001.
-
FDA (2001b) Guidance for industry, Bioanalytical Method Validation. U.S. Department of Health and Hesham AEliwa and AA Alaa Eldin. Bioequivalence Study of Easyrect 100 Mg Tablets Versus Spedra® 100 mg Tablets after a Single Oral Dose Administration of Each to Healthy Volunteers Male Adults under Fasting Conditions. Bioequiv & Bioavailab Int J 2018, 2(3): 000134. Human Services. Food and Drug Administration, Center for Drug
-
1FDA (2003) Guidance for industry, Bioavailability and bioequivalence studies for orally administered drug products – General considerations. U.S. Department of Health and Human Services. Food and Drug Administration, Center for Drug Evaluation and Research (CDER) March 2003.
-
Committee for Proprietary Medicinal Products (CPMP) (2000) Note for guidance on the investigation of bioavailability and bioequivalence.
-
Multivariate Approaches for Simultaneous Determination of Avanafil and Dapoxetine by UV Chemometrics and HPLC-QbD in Binary Mixtures and Pharmaceutical Product. J AOAC Int. eng.
-
The European Agency for the Evaluation of Medicinal Products (EMEA). Note for Guidance on the Structure and Content of Clinical Study.
-
The European Agency for the Evaluation of Medicinal Products (EMEA). Note for Guidance on Good Clinical Practice.
-
The European Agency for the Evaluation of Medicinal Products (EMEA). Note for Guidance on the Investigation of Bioavailability and Bioequivalence, CPMP/EWP/QWP/1401/98.
-
FDA/USP23-NF-guidline (1995) United States Pharmacopeia-the National Formulary. Rockville, Maryland, United States Pharmacopeial Convention.
-
World Health organization (1986) Guidelines for the investigation of bioavailability. World Health organization Regional Office for Europe, Copenhagen.
-
World Medical Association Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. Adopted by the 18th WMA General Assembly Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul. Copyright© Hesham AEliwa and AA Alaa Eldin.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review