Bioequivalence Study of Two Formulations of Cefixime
Cefixime is a broad-spectrum oral antibiotic used for treating a wide variety of bacterial infections. Study Objective: The objective of this study was to find out whether bioequivalence study of Cefixime 200 mg, Profim® capsule manufactured by PT Promedrahardjo Farmasi Industri in comparison with Cefixime 100 mg, Cefspan® capsule manufactured by PT Dankos Farma, For PT Kalbe Farma Tbk, under license by Astellas Pharma Inc., Osaka – Japan. Methods: The study was conducted using an open-label, randomized, single-dose, two-periods, two-treatments, crossover study under fasting conditions with 8 (eight) days washed-out period between each period. According to the random design, a single oral dose of the test drug or reference drug was administered to 30 healthy male subjects after overnight fasting. The number of subjects who finished the study was twenty-eight (28) healthy male subjects. Serial plasma samples were obtained over a 32 hours period. Plasma concentrations of the drug were determined by LC-MS/MS method. From the Cefixime concentration vs. time curves, the following pharmacokinetic parameters were obtained: AUC0-32h, AUC0-∞, and Cmax, while the statistical interval proposed was 80.00 - 125.00% for AUC0-32h and Cmax with 90% Confidence Interval (CI) with α = 5.00%. The estimation of Tmax and T1/2 in the bioequivalence study was based on a nonparametric statistical procedure on the original data using Wilcoxon Sign Test. Results: The main pharmacokinetic parameters of the test drug Profim® (BN: B051A21P-1)/ reference drug, Cefspan® (BN: KCEFB00038) ratio were as follows: AUC0-32h: 105.86 (95.41 - 117.44) with CV Intra Subjects was 22.72% and Cmax: 105.63 (95.33 - 117.03) with CV Intra Subjects was 22.43 %. Whilst TMAX of the test drug Profim® (BN: B051A21P-1)/ reference drug, Cefspan® (BN: KCEFB00038) were respectively 4.50 (3.50 – 6.00) h and 4.50 (3.00 – 6.00) h; mean T1/2 were respectively 4.18 ± 0.78 h and 4.14 ± 0.56 h; and mean Slope were respectively (-0.17) ± 0.03 h and (-0.17) ± 0.02 h. There is no adverse event that occurred during this study. Conclusion: The present study demonstrated that the evaluated test drug Profim® (BN: B051A21P-1) were bioequivalence in term of both rate and extent of absorption to the reference drug Cefspan® (BN: KCEFB00038).
Introduction
Cefixime is a 3rd generation of cephalosporin which has marked in vitro bactericidal activity against a wide variety of gram-positive and gram-negative organisms. It is particularly active against many Enterobacteriaceae, Haemophilus influenzae, Streptococcus pyrogens, Streptococcus pneumonia, and Branhamella catarrhalis. Cefixime has been indicated for uncomplicated urinary tract infections, otitis media, pharyngitis and tonsilitis, acute exacerbation of chronic bronchitis, and uncomplicated gonorrhea (cervical/ urethral) [1] (Figure 1).
Cefixime (CAS 125110-14-7) is described chemically as ((6R,7R)-7[2-(2-Amino-4-thiazolyl)glyoxylamido]-8-oxo-3- vinyl-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylic acid, 72-(Z)-[O-(carboxymethyl)oxime]trihydrate). The empirical formula is C16H15N5O7S2 • 3H2O. The molecular weight of cefixime is 507.50. Cefixime is a white, light-yellow powder, slightly soluble in water, acetone, and glycerin; practically insoluble in ether and ethyl acetate. Soluble in propylene glycol [2].
Cefixime has bactericidal action and the action inhibition of cell-wall synthesis [3]. It has high affinity for penicillin- binding proteins (PBP) 1 (1a, 1b, and 1c) and 3, with the site of activity varies according to the organism [4].
Absorption of Cefixime following a single oral dose of 100 or 200 mg in healthy, fasted adults, maximum serum at 4 hours were, respectively, 0.69, 1.13, and 1.95 μg/mL. The serum half-life was 2.3 - 2.5 hours. Cefixime distributes through penetration into sputum, tonsils, maxillary sinus mucosal tissue, otorrhea, biliary fluid, and gall-bladder tissue is good [4].
No antibacterially active metabolites are found in the human serum or urine. Cefixime is excreted primarily renally.
The extent of urinary excretion (up to 12 hours) after oral administration of 50, 100, or 200 mg (potency) in healthy, fasted adults was about 20-25%. Maximum urine concentrations were, respectively 42.9, 62.2, and 82.7 mg/ mL at 4 - 6 hours [4].
Study Protocol
The study protocol was reviewed and approved by the Ethics Committee of the Medical Faculty University of Indonesia and the National Agency for Drug and Food Control of Republic Indonesia (BPOM RI).
The protocol described all details of the project, including design of the study, clinical procedures, bioanalysis of blood samples obtained from the participants, pharmacokinetic and statistical data analysis, bioequivalence evaluation, the informed consent form, and ultimately documentation and final report issuance.
Ethical Considerations
The study was carried out according to The International Council for Harmonization (ICH) guidelines for Good Clinical Practice (GCP) and the declaration of Helsinki provisions [5, 6]. Each subject was given the informed consent form during the screening phase before starting the study. A meeting was arranged by the principal investigator and clinical investigators to explain all details of the study to the subject, including the purposes, risks, advantages, procedures, and the right as a research subject to withdraw at any time during the study, and the compensation in case of any harm caused by the study.
Study Design
An open-label, randomized, single-dose, two-periods, two-treatment, and fasting condition were applied in this study [1]. The subjects were randomly assigned to each dosing sequence of the investigational drug products (test and reference formulations). This study was carried out on thirty (30) healthy male subjects. The number of subjects who finished the study was twenty-eight (28) healthy male subjects.
Inclusion and Exclusion Criteria for Participation in the Study
The subjects were regarded eligible for participation in this research based on the following inclusion criteria: willing to sign an informed consent, adult male/female subjects with ages between 18-55 years and body mass index (BMI) ranges from 18–25 kg/m2, vital sign after 10 minutes resting within ranges: pulse rate 60-90 bpm, respiratory rates 12-20 x/ minutes, systolic blood pressure 100-130 mmHg and diastolic blood pressure 60-90 mmHg, the subject must have 12 lead ECG without any significant abnormalities, and negative result of rapid test antigen Covid 19 in 1st and 2nd period.
The exclusions criteria including participate in another study within 3 months prior to the first day of study drug administration, pregnant or lactating female, smokers and smoking more than 10 cigarettes per day, intake of any prescription drug or non-prescription drug within 7 days prior the first day of drug administration of this study, blood donation or blood loss of 300 mL (or more) within 3 months prior to the first day of study drug administration, history of drug and/or alcohol abuse or dependency within 12 months prior to the first day of study drug administration, known hypersensitivity or contraindication to the study drug, any surgical or medical condition (present or history) which might significantly alter the absorption, distribution, metabolism or excretion of the study, e.g. gastrointestinal disease including gastric or duodenal ulcers or history of gastric surgery, history of any bleeding or coagulative disorders, clinically significant hematology abnormalities, clinically significant urinalysis abnormalities, renal insufficiency (plasma’s creatinine concentration ≥ 1.50 mg/dL), history or presence of any liver dysfunction (SGPT, alkaline phosphate, total bilirubin ≥ 1.5 ULN), and positive result of HBsAg, HCV, and/ or HIV test. Health screening conducted is prior to the study to evaluate the subject’s health condition based on inclusion and exclusion criteria.
Health Screening
Subjects were through medical examination within 30 days prior to their first study drug administration day. These include assessment of physical examination, vital signs (i.e. blood pressure, pulse rate, and body temperature), and ECG was conducted by Responsible Physician in Biometrik. Laboratory values of liver function (AP, SGPT, SGOT, and total/direct bilirubin), renal function (serum creatinine and urea), routine hematology (hemoglobin, hematocrit, erythrocytes, platelets leucocyte count, leukocyte differential count, and erythrocytes sedimentation rate), blood glucose, routine urinalysis (specific gravity, pH, leucocytes esterase, nitrite, albumin, glucose, ketones, urobilinogen, bilirubin, occult blood, tubular and sediment) were tested by Clinical Laboratory. Immunology test for HBsAg, HCV, HIV, and Rapid Test Antigen Covid-19 was conducted in Biometrik. During the screening and immunology test (HBsAg, HCV, and HIV) approximately 10 mL (equivalent to 2 teaspoons) of blood samples were drawn from each subject.
Drug Products Administration
The subjects were admitted to the Biometrik Riset Indonesia on a day before the study for quarantine. All subjects were fasted for 10 hours overnight starting from 09.00 p.m. until 07.00 a.m. to drug administration. On dosing day at 07.00 a.m. subjects were instructed to consume one (200 mg) capsule of the test drug or two (2@100 mg) capsules of the reference drug. The reference drug used in this study was 2 (two) capsules of 100 mg Cefixime since that the reference drug marketed in Indonesia is only available in 100 mg dose.
Single oral dose of the study drug was given in a pill case, swallowed by each subject with 250 mL of water according to randomization. After 2 hours, warm water was provided as desired. No food was allowed until 4 h after study drug administration. Standard meals were reserved at 4 h (breakfast), 6 h (lunch), and 12 h (dinner) after study drug administration. Subjects were remaining in sitting position until 4 hours period after drug administration. Subjects were not allowed to exit the clinical facility except with Responsible Physician’s permission.
Blood Samples Collection
After fasting overnight, approximately at 06.00 a.m. on sampling day, 5 mL pre-dose blood sample was collected within one hour prior to drug administration for each period. After drug administration, a 5 mL blood sample was taken at 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 5.5, 6, 9, 12, 16, 24, and 32 hours drug administration.
After a washout period of eight days, subjects underwent the second period of the study. The procedure of the second period was repeated in the same manner to complete the crossover design.
Total volume of blood were taken during the study is approximately 180 mL or equivalent to 18/25 glass of drinking water, which is consisting of 10 mL blood sample (equivalent to 2 teaspoons) were taken for screening and 170 mL blood sample (equivalent to 17/25 cup of mineral water) were taken for each subject during two periods of sampling.
Blood samples were drawn with disposable syringe and transferred into K3EDTA blood collection tubes. Plasma was separated by centrifugation at 7,000 rpm (≈ 6,793 x g) for 5 minutes and immediately transferred plasma into three clean microtubes 2.0 mL, consist two microtubes for analysis and one microtube for retained sample.
Plasma separation was carried out in a plasma separation room with a temperature range of 20 - 30° C, and humidity range 40 - 70% RH.
Statistical Analysis
The statistical method for testing bioequivalence is ANOVA for 2-treatments, 2-sequence, 2-period cross- over comparing AUC0-32h, AUC0-∞, and CMAX after transformation of the original into their logarithmic values where the factors formulation, period, sequence, and subject nested within the sequence was used to explain overall variability in the observations. Bioequivalence is concluded if the 90% confidence interval with α = 5.00% of the Test/Reference geometric means ratio is in the range of 80.00-125.00% for AUC0-32h, AUC0-∞, and CMAX [7, 8]. This acceptance criterion is according to the Indonesian Guidelines, Pedoman Uji Bioekivalensi, Badan Pengawas Obat dan Makanan (BPOM), Jakarta [7]; European Guidelines on The Investigation of Bioequivalence European Medicines Agency (EMA) [8]; and ASEAN Guidelines for The Conduct of Bioequivalence Studies [9]. EquivTestPK software (Statistical Solution Ltd, Saugus, MA, USA) was used to perform the statistical analysis of AUC0-32h, AUC0-∞ and CMAX using analysis of variance (ANOVA) after transformation of the data to their logarithmic (ln) values.
$$ 90 \% \mathrm {CI} = \left(X _ {\mathrm {T}} - X _ {R}\right) \pm t _ {0. 1 (\mathrm {v})} \sqrt {S ^ {2} \left(\frac {1}{n _ {T R}}\right) + \frac {1}{n _ {T R}}} $$
2 T 0.1(v)
Using the error variance (S2) obtained from the ANOVA; the 90% confidence intervals with α = 5.00% were calculated from the following equation: X̅T, X̅R: the means of In transformed values for the test drug [T] and the reference drug [R].
- S2: the error variance obtained from the ANOVA.
- nTR, nRT: the number of subjects of sequence TR and RT.
- t0.1: the t-value for 90% CI with α = 5.00% .
- v: the degree of freedom of the error variance from ANOVA.
The anti (ln) of the above confidence intervals (CIs) are the 90% CIs with α = 5.00% of the ratios of the test/ the reference geometric means. The difference in TMAX was analyzed non-parametrically on the original data (not transformed) using Wilcoxon Test [7].
Meanwhile, T1/2 was analyzed using parametric or non- parametric statistics on the original data (not transformed) depending on whether the data is normally distributed or not using Wilcoxon Test [7].
Assay Methodology and Validation
Prior to the assay of Cefixime in sample, bioanalytical method validation was evaluated for anticoagulant effect (i.e. comparing the effect of CPDA anticoagulant used in blank plasma bought from Indonesian Red Cross for method validation towards anticoagulant used in K3EDTA anticoagulant used in blood collection tube to collect blood samples); selectivity; carry-over; calibration curve and Lower Limit of Quantification (LLOQ); precision and accuracy; matrix effect; dilution integrity; and stabilities (i.e. short term stability at room temperature and post-preparative/ autosampler batch integrity, freeze-thawed stability, also long term stability) [10]. An assay of Cefixime concentration in plasma was carried out by a fully validated LC-MS/MS with LLOQ 50.00 ng/mL and used Etoricoxib as internal standard.
Data Quality Assurance
Drug accountability is maintained by investigators who keep all the records of the disposition of all study drugs received, administered, accidentally destroyed, and destroyed when expired according to criteria in Indonesian Guidelines, Pedoman. Uji Bioekivalensi, Badan Pengawas Obat dan Makanan [7]. The rest of the plasma samples analysis was destroyed following stability long-term validated method, while retain samples will be destroyed for at least 1 year after the final reports had been sent to the Sponsor. The data handling and verification were maintained by making Case Report Form (CRF) which was filled legibly using a blue ball- point. The forms were verified against all original records. A copy was retained in the investigator’s files, and all other copies were given to the Sponsor.
Sponsor generally performs site/clinical monitoring of clinical trial to assure high quality trial conduct. Therefore Sponsor was appointing their personnel as Monitor of study. The Monitor is committed to professional secrecy. They perform monitoring of individual case histories, assess adherence to the study protocol, ensure the ongoing implementation of appropriate data entry and quality control procedures, and in general assess adherence to Good Clinical Practices [11].
Results and Discussion
Demographic Data and Adverse Event
Total number of subjects who finished this study was 28 healthy subjects. The demographic data of subjects are tabulated in Table 1 below.
| Min | Max | |
|---|---|---|
| Age (year) | 21 | 51 |
| BMI (kg/m²) | 18 | 25 |
| Pulse (bpm) | 64 | 90 |
| Respiratory Rate (x/minute) | 16 | 18 |
| Blood Pressure (mm/Hg) | 100/70 | 130/90 |
Table 1: Demographic Data of 28 Subjects.
Results and Discussion
Bioanalytical Result
Results of applying the bioanalytical method to the bioavailability/bioequivalence study of Profim® (BN: B051A21P-1) manufactured by PT Promedrahardjo Farmasi Industri in twenty-eight (28) subjects were all calibration curves of the subject showed good linearity within the range of ng/mL with the coefficient of correlation (R2) ≥ 0.99. For Accuracy and precision provided on Table 2 below.
| Accuracy | Precision | |
|---|---|---|
| QC Low (148.63 ng. mL-1) | 2.23% | 7.65% |
| QC Med (4,954.34 ng. mL-1) | 3.72% | 7.34% |
| QC High (7,431.51 ng. mL-1) | 1.63% | 7.44% |
| LLOQ (50.04 ng. mL-1) | 0.12% | 4.38% |
Table 2: Accuracy and Precision.
Pharmacokinetic Analysis
The pharmacokinetic parameters (AUC0-32h, AUC0-∞ CMAX, and TMAX) of test drug (T) and reference drug (R) were calculated and compared to assessed bioequivalence.
The calculated 90% CI with α = 5.00% for the geometric mean of individual and the ratios of AUC0-32h and AUC0-∞ as well as Cmax for the test drug Profim® (BN: B051A21P-1) and reference drug Cefspan® (BN: KCEFB00038), were all within 80.00 - 125.00% interval.
This was in conformity with the standard guideline for bioavailability/bioequivalence study issued by the National Agency of Food and Drug Control of the Republic of Indonesia.
The main pharmacokinetic parameters drug of study Cefixime, obtained form 28 subjects after oral administration of test drug with reference drug showed in Table 3 below.
| Parameter | Mean (SD) | Geometric Mean Ratio of T/R (90% CI) | % Intrasubject CV | Statistical power (%) | |
|---|---|---|---|---|---|
| Test | Reference | ||||
| AUC (ng.h/ml) 0-32 | 15,570.91 (6,664.51) | 15,363.87 (9,771.36) | 105.86% (95.41%-117.44%) | 22.72% | 100% |
| AUC (ng.h/ml) 0-∞ | 16,190.85 (6,683.09) | 15,995.20 (9,792.11) | 106.00 %( 96.55%-116.36%) | 20.42% | 100% |
| C (ng/ml) MAX | 1,812.44 (707.81) | 1,757.42 (932.90) | 105.63% (95.33%-117.03%) | 22.43% | 100% |
| T (hours) 1/2 | 4.18 ± 0.78 | 4.14 ± 0.56 | |||
| T (hours) MAX | 4.50 (3.50-6.00) | 4.50 (3.00-6.00) |
Table 3: Pharmacokinetic Parameters of Cefixime After a Single-Dose Oral Administration of Test & Reference Drug.
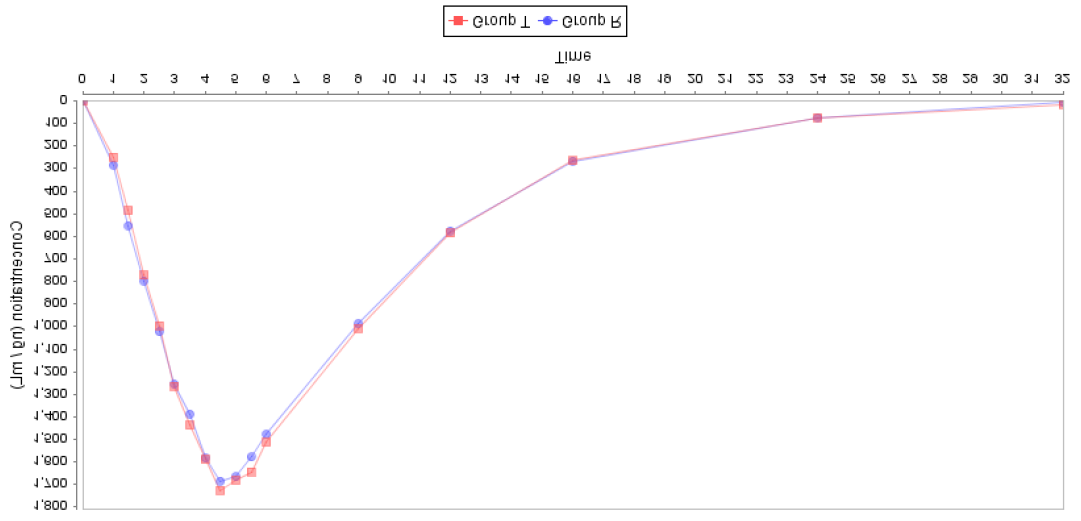
The means of plasma concentrations vs. time profiles after single dose of oral administration of investigational products are shown in Figure 2 below.
Conclusion
Based on the data obtained from the bioequivalence study, it is concluded that Profim® (BN: B051A21P-1) manufactured by PT Promedrahardjo Farmasi Industri is BIOEQUIVALENCE in term of both rate and extent of absorption to the reference drug Cefspan® (BN: KCEFB00038) manufactured by PT Dankos Farma, For PT Kalbe Farma Tbk, Under License by Astellas Pharma Inc., Osaka – Japan with Geometric Mean Ratio (GMR) and 90% confidence interval for AUC0-32 and CMAX parameter in the range of 105.86% (95.41%-117.44%) and 105.63% (95.33%-117.03%) respectively (requirement 80.00 - 125.00% for AUC0-t and CMAX) and the intra-subject coefficient of variation is 22.72% and 22.43%. Therefore, it can be assumed that the two formulations are therapeutically equivalent and therefore interchangeable.
References
-
Patil S, Hajare A, Krishnaprasad K (2014) Open-Label, Randomized, Crossover Comparative Bioavailability Study Of Cefixime From Two Tablet Formulations After Single Oral Administration. International Journal Basic Clinical Pharmacology 3(1).
-
USP Safety Data Sheet: Cefixime.
-
USP Reference Standard: Cefixime.
-
Dankos Farma PT, For PT Kalbe Farma Tbk, Under License by Astellas Pharma INC, Osaka – Japan. Cefspan® Product Insert.
-
(2015) Guidelines for Good Clinical Trial Methods. National Agency of Drug and Food Control.
-
Williams JR (2008) The Declaration of Helsinki and public health. Bulletin of the World Health Organization 86(8): 650-652.
-
(2015) Bioequivalence Test Guidelines. National Agency of Drug and Food Control.
-
(2010) Guideline on the Investigation of Bioequivalence. European Medicines Agency, London.
-
(2015) ASEAN Guidelines for the Conduct of Bioequivalence Studies, pp: 1-43.
-
(2011) Guideline on Bioanalytical Method Validation. European Medicines Agency.
-
(2006) Guidance for Clinical Trial Sponsors - Establishment and Operation of Clinical Trial Data Monitoring Committees. US Department of Health and Human Services, Food and Drug Administration, USA.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review