High Incidence and Mortality of Cervical Cancer in the Southern United States
Cervical cancer incidence and mortality rates have dramatically decreased in the United States in the past three decades. However, these rates remain high in most Southern states. We conducted a literature review to summarize socio-demographic factors and healthcare-seeking behaviors that may contribute to higher rates in the South. Identified factors included cervical cancer disparities among African American women, low socioeconomic status (SES), limited knowledge of human papilloma virus (HPV) and cervical cancer, low coverage of Pap test and HPV vaccination, and stigma towards HPV and cervical cancer. Existing interventions have made a moderate decrease for incidence and mortality of cervical cancer. More evidence-based culturally-tailored interventions are needed to resolve existing cancer disparities, improve access to care, promote HPV vaccination, and eliminate barriers to cervical cancer screening to address cervical cancer disparity in this region.
Stahr1, Tamier L Wells1, Hao Wu3, Ronda Henry-Tillman4 and L
Joseph Su1
Tel: 501-526-8909; E-mail: jtao@uams.edu
disparity in this region.
Keywords: Cervical cancer; Human papilloma virus; South
Cervical Cancer Incidence and Mortality in the South
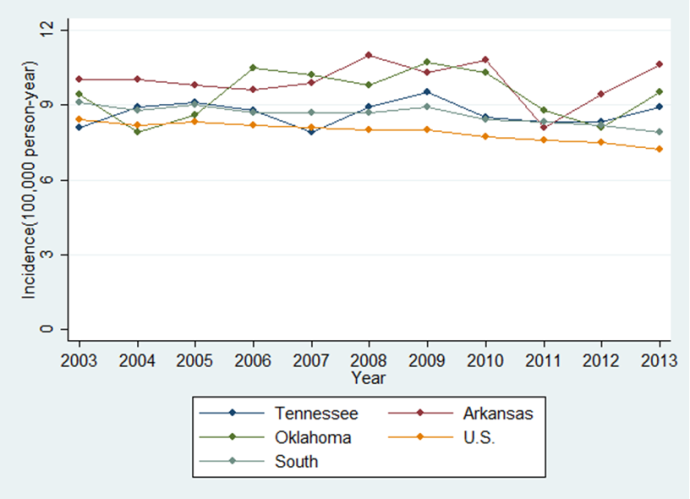
Cervical cancer was once the third most common gynecological cancer in the United States [1]. Cervical cancer screening tests commonly known as Pap tests have contributed to the decline in cervical cancer incidence and mortality in the U.S. [2]. The U.S. Centers for Disease Control and Prevention (CDC) reported that age-adjusted cervical cancer incidence rates had decreased from 9.8 per 100,000 person-year in 1999 to 7.7 per 100,000 person-year in 2013. Similarly, the mortality rate had reduced from 2.8 in 1999 to 2.2 in 2013 [3]. However, cervical cancer incidence and mortality rates remain high in Southern states (Figures 1 and 2) [4]. Arkansas had the highest cervical cancer incidence (10.6 per 100,000 person-year) in 2013, followed by Oklahoma (9.5 per 100,000 person-year), Tennessee (8.9 per 100,000 person-year), Texas (8.7 per 100,000 person-year), Alabama (8.5 per 100,000 person-year), Florida (8.4 per
100,000 person-year), Louisiana (8.2 per 100,000 person- year), and Mississippi (8.1 per 100,000 person-year). For mortality, Mississippi was the highest (4.0 per 100,000 person-year) in 2013, followed by Alabama (3.6 per 100,000 person-year), Louisiana (3.5 per 100,000 person- year), Arkansas (3.4 per 100,000 person-year), Tennessee and Florida (2.8 per 100,000 person-year), Texas (2.7 per 100,000 person-year), and Oklahoma (2.4 per 100,000 person-year). Given the persistently higher cervical cancer incidence and mortality rates in the South, the goal of this manuscript is to identify and explore the shared features that may lead to higher cervical cancer incidence and mortality.
Cervical Cancer Disparities among African American Women
![Figure 2: Cervical cancer mortality in the United States and southern states, 2003-2013 (Data was from United States Cancer Statistics (USCS)). The African American population is concentrated in the South. According to the 2015 census, 37% of people living in Mississippi are African Americans. More than 15% of people living in the South are African American. Racial disparities exist in terms of cervical cancer among African American women. Human Papilloma virus (HPV) is the most common cause of cervical cancer. The prevalence of HPV was significantly higher among African Americans (39.2%; 95% confidence interval [CI], 31.0-49.4%) than that in Non-Hispanic Whites (24.2%; 95% CI, 20.5-28.6%) in 2003-2004 [5]. African American women were more likely to report not having received a Pap test, [4,6] and no recommendation from their doctors for cervical cancer screening [7] African American women are less likely to get standard treatment for cervical cancer than Non- Hispanic White women [8]. African American women are more likely to be diagnosed at the late stage [9]. The higher incidence and mortality rates of cervical cancer in African American women were observed during 1999 to 2013. In 2013, cervical cancer incidence rates were 8.8 and 7.2 per 100,000 person-year for African American and Non-Hispanic Whites; cervical cancer mortality rates were 3.8 and 2.2 per 100,000 person-year among African American and Non-Hispanic Whites [3].](/fulltextimages/824/fig_2.png)
Figure 2: Cervical cancer mortality in the United States and southern states, 2003-2013 (Data was from United States Cancer Statistics (USCS)). The African American population is concentrated in the South. According to the 2015 census, 37% of people living in Mississippi are African Americans. More than 15% of people living in the South are African American. Racial disparities exist in terms of cervical cancer among African American women. Human Papilloma virus (HPV) is the most common cause of cervical cancer. The prevalence of HPV was significantly higher among African Americans (39.2%; 95% confidence interval [CI], 31.0-49.4%) than that in Non-Hispanic Whites (24.2%; 95% CI, 20.5-28.6%) in 2003-2004 [5]. African American women were more likely to report not having received a Pap test, [4, 6] and no recommendation from their doctors for cervical cancer screening [7] African American women are less likely to get standard treatment for cervical cancer than Non- Hispanic White women [8]. African American women are more likely to be diagnosed at the late stage [9]. The higher incidence and mortality rates of cervical cancer in African American women were observed during 1999 to 2013. In 2013, cervical cancer incidence rates were 8.8 and 7.2 per 100,000 person-year for African American and Non-Hispanic Whites; cervical cancer mortality rates were 3.8 and 2.2 per 100,000 person-year among African American and Non-Hispanic Whites [3].
Socioeconomic Status (SES) in the South
As defined by the United States Census Bureau, 90% of the Southern states are considered to be rural [10]. A substantial proportion of people in the South (27-51%) live in rural areas, except for Florida and Texas [11]. People living in rural areas are likely to have limited access to health care facilities because insurance status and distance traveling to such facilities. Hence, rural populations are less likely to seek cervical cancer screenings, and are at a higher risk for developing and dying from cervical cancer [12]. Under-education and high poverty levels are also common features in the South. Most Southern states are listed as the top 10 least- educated states [13]. Of people living in the South, 15%- 19% have a family household lower than the federal poverty line [14]. Research has shown that people with less than a high-school education and living below poverty line were more likely to be HPV-infected [5]. Further increasing the detrimental effects of HPV on this population is that they are less likely to seek cervical cancer screening due to limited access to health care, which leads to higher incidence and mortality rates from HPV-related cancers. Additionally, individuals without healthcare insurance are less likely to receive timely and consistent cervical cancer screening [15]. Medicaid is a federally-funded insurance option for eligible low-income women. In 2015, Medicaid provided approximately 17% of eligible nonelderly women with insurance nationwide [16]. However, most Southern states have only enrolled a small proportion of Medicaid-eligible women, which leaves most low-income women in the South uninsured [17]. From 12% to 21% of nonelderly women living in the South were uninsured in 2015 [16]. Consequently, low SES and lack of insurance coverage could be responsible for the high incidence and mortality rates of cervical cancer in the South [4].
Knowledge about HPV and Cervical Cancer HPV infection is common among sexual active adults. Approximately 75% to 85% of sexually active people can have HPV infection during their lifetime [18]. Most HPV infections can be resolved spontaneously without clinical symptoms. However, persistent oncogenic HPV infections are one of risk factors for cervical cancer. Accurate knowledge about HPV and its relation to cervical cancer are critical for cervical cancer prevention [19, 20, 21]. Even though knowledge itself does not have a direct effect on the change of health behavior [22], it can urge people to seek health care when mediated by risk perceptions, social influence, and self-efficacy [23]. A national survey about HPV and cervical cancer shows only 40% of women have heard about HPV and less than 20% knew HPV can cause cervical cancer [24]. Being Non-Hispanic Whites and having a college education were associated with knowledge about HPV [24, 25]. Since people living in the South are less likely to have a college education and/or self-identify as Non-Hispanic Whites, it is plausible that fewer people living in the South know about HPV and cervical cancer. Limited knowledge about HPV and cervical cancer could have an indirect impact on the high incidence and mortality rates of cervical cancer in the South, as it may contribute to the reasons that women in the South do not receive regularly cervical cancer screening and do not to vaccinate their children to prevent from HPV infection.
Cervical Cancer Screening
In 2001, a combination of Pap testing and HPV testing was recommended for cervical cancer screening [26]. Pap test has a high specificity to detect cancerous or precancerous lesions. HPV testing is able to detect oncogenic HPV infections, even before precancerous lesions exist. Widespread cervical cancer screening in the U.S. has contributed to the dramatic decrease incervical cancer incidence in the past three decades. However, regional disparity in cervical cancer screening rates has been documented. A study shows that 88% of women in the south reported having a Pap test [7], which was lower than that in a national survey (93%) [27]. Data from the U.S. CDC also indicates that women in the South were less likely to report having a Pap test in the past three years, which would result in women with cancerous or precancerous lesions not being diagnosed until late stage and higher incidence and mortality rates for cervical cancer in the South [28].
HPV Vaccinate
HPV infection is the most common cause of cervical cancer [29, 30, 31]. Among 30 to 40 types of sexually transmitted HPV, HPV genotypes 16 and 18 caused approximately 70% of all cervical cancer cases [32]. HPV vaccine is effective in the prevention of HPV-associated genital warts and cervical abnormalities [33, 34, 35]. Despite approval of the HPV vaccine in 2006, the United States has been slow to vaccinate adolescents. The percentage of completion of at least 3 HPV vaccine doses among female adolescents in the U.S. has increased from 16.6% in 2008 to 41.9% in 2015 [36]. However, it is still far away from the 80% coverage goal set by the Healthy People by 2020. Completion rates in the South are even worse [36, 37]. The HPV vaccination coverage rates in most Southern states are lower than the national rates. Mississippi had the lowest coverage for 3 HPV vaccine doses (24.4% in 2015) among female adolescents [36]. Most Southern states do not have any regulation towards HPV vaccination among adolescents. Only Texas and Louisianan require public education about HPV and cervical cancer. Limited knowledge about HPV and cervical cancer is one of the obstacles for HPV vaccination. [38, 39, 40] Research has shown that low HPV vaccine coverage is associated with the high incidence and mortality rates of cervical cancer in the U.S. [41]
Stigma towards HPV and Cervical Cancer
Stigma is a social process, and includes labeling, stereotyping, separation, status loss, and discrimination [42, 43, 44]. Stigma is towards people with undesirable attribution, which cause devaluation for individuals [45]. Cancer-related stigma has been well documented in the literature, especially for cancers that are caused by voluntary behaviors [46]. Cervical cancer patients are more likely to be stigmatized because sexually transmitted HPV causes cervical cancer. Although research exploring stigma among cervical cancer patients is limited, results indicate that women with cervical cancer experience enacted stigma - prejudice and discrimination; they also had felt stigma - the expectation of stigmatization, and internalized stigma - negative feelings and beliefs because of HPV infection [47, 48, 49, 50, 51]. Stigma is also associated with delayed treatment for patients whose diseases are caused by sexually transmitted diseases (STDs) [52, 53]. High level of stigma towards HPV and cervical cancer may contribute to the high incidence and mortality rates of cervical cancer in the South. Studies have shown that limited knowledge about HPV and cervical cancer leads to higher levels of stigma towards HPV infection and cervical cancer [47, 50, 51]. As less people living in the South have adequate knowledge about HPV and cervical cancer, women reside in Southern states with cervical cancer may endure higher levels of stigma. People living in southern states also tend to express a higher level of religiosity, particularly Protestant Christianity. In the Southern states, the percentage of adults reporting high religiosity varies from 54% to 77% [42]. High religiosity is associated with higher levels of stigma towards STDs [54]. Hence, stigma towards HPV and cervical cancer is likely to be higher in the South. Stigma towards HPV and cervical cancer could be one of the major barriers to HPV vaccination and cervical cancer screening, diagnosis, and treatment [46, 55].
Interventions and Future Research to Decrease Cervical Cancer Incidence and Mortality
Efforts have been put in place to address racial disparity related to cervical cancer. Existing interventions have shown their effect on broadcasting knowledge about HPV and cervical cancer, including individual-directed counseling, culturally sensitive print materials, access- enhancing, peer navigators, community education, and mass media campaign, and improving cervical cancer screening [56, 57, 58]. Although African American women still have higher cervical cancer incidence rates than Non- Hispanic White women, a decline has been observed owing to available Government programs, such as National Breast and Cervical Cancer Early Detection Program (NBCCEDP), have provided low SES women with increased access to timely cervical cancer screenings and diagnosis [59]. Most Southern states have their own programs that offer cervical cancer services for undeserved and uninsured women. However, these programs do not meet the needs of all eligible women. For example, NBCCEDP only covers 6.5% of eligible women for cervical cancer screening through their program [49]. Since many of these eligible women may have limited health literacy, outreach education and assistance on how to apply for free cervical cancer screenings are needed to improve the coverage of these federal and state-funded programs. Improving access to preventive care is critical to improving cervical cancer screening rates. However, a substantial proportion of women, especially in the South may be reluctant to receive Pap and/or HPV testing in clinics due to embarrassment, stigma, or fear [60]. Alternative screening method for cervical cancer is needed for people who never or have under-screened for cervical cancer. Self-collected HPV testing is a promising alternative, as it can protect privacy and reduce stigmatization towards HPV infection [61, 62]. However, there are many challenges for self-collected HPV testing including: 1) how to effectively inform individuals of test results and provide people with positive testing results of oncogenic HPV infections a timely referral; 2) how to retain those high risk women for further follow-up, and 3) how to make self-collected HPV testing kit affordable for women who are uninsured or underinsured. Once these challenges are resolved, self-collected HPV testing could increase the coverage of cervical cancer screening and may contribute to decreased cervical cancer incidence and mortality rates in the South. Stigma towards HPV and cervical cancer could be one of contributing factors for the high incidence and mortality of cervical cancer rates in the South. Even though cervical cancer stigma has been widely discussed, few published studies are available. The effect of stigma towards HPV and cervical cancer on health care seeking has been concluded based on stigma related to other STDs. Most studies on stigma towards HPV and cervical cancer used a qualitative approach [47, 48, 50, 63]. A few studies utilized a quantitative method to measure stigma with scales modified from those for HIV/AIDS or other STDs [49, 64]. There is barely any research on interventions for stigma towards HPV and cervical cancer [65]. Limited research suggests that emphasis on the high prevalence of HPV infections and focusing on only oncogenic HPV infections that cause cervical cancer may reduce stigma [64, 65]. There is a critical need for a psychometrically-tested scale to measure stigma towards HPV and cervical cancer, which is valid and reliable across diverse populations, particularly populations that are burdened by disparate HPV and cervical cancer rates. Additional research is necessary to design interventions to reduce stigma and to explore stigma’s effect on care- seeking behavior and diagnosis and prognosis of cervical cancer. The reduction of stigma towards HPV and cervical cancer could benefit for the prevention of cervical cancer for the underserved minority population, especially in the South. HPV vaccination is considered the primary prevention tool against HPV-related cancer. However, low rates of HPV vaccination acceptability and series completion make it hard to achieve the expected protective effect at the population level. The lack of physicians’ enthusiastic recommendation and the unwillingness of parents to vaccinate their children are mainly responsible for the low coverage of HPV vaccination [66]. The publication of Accelerating HPV vaccine uptake: urgency for action to prevent cancer in 2014 called for increased efforts to encourage physicians to assertively recommend HPV vaccination and educate parents about benefits of the HPV vaccine. However, a significant increase of HPV vaccination uptake among American adolescents has still not been observed. Although school-based HPV vaccination programs have achieved success in the United Kingdom and Australia, it remains highly controversial to enforce HPV vaccination at schools in the U.S. Financial concern is another obstacle for HPV vaccination. The Federal Affordable Care Act (ACA) requires that the HPV vaccine should be covered by most health insurance by January 2017, which will hopefully result in a modest increase of HPV vaccination among adolescents. Similarly, government-sponsored medical programs may further increase HPV vaccine uptake among underinsured or uninsured adolescent and young adults. Given the barriers identified to date to increase HPV vaccination coverage for people living in the South, resources and efforts should be tailored to increase the coverage of HPV vaccination for the sake of reducing cervical cancer incidence and mortality rates.
Conclusion
High cervical cancer incidence and mortality rates in the South are due to multiple factors, including cervical cancer disparities among African Americans, poverty, limited knowledge of HPV and cervical cancer, low insurance and medical provider coverage especially in rural areas, and stigma towards HPV and cervical cancer. Although interventions and practice-based efforts have tried to address these problems, significant problems still exist. Effective and creative interventions that are customized to southern culture, especially among African Americans are needed to reduce cervical cancer incidence and mortality in the South.
References
-
American Cancer Society. Cancer facts and figures, 1998. In. Atlanta: American Cancer Society.
-
Smith HO, Tiffany MF, Qualls CR, Key CR (2000) The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States--a 24-year population-based study. Gynecol Oncol 78(2): 97-105.
-
Cervical Cancer Rates by Race and Ethnicity. In. CDC.gov: Centers for Disease Control and Prevention; 2015.
-
Freeman HP, Wingrove BK (2005) Excess cervical cancer mortality: a marker for low access to health care in poor communities. Rockville, MD: National Cancer Institute, Center to reduce cancer health disparities 5: 5282.
-
Dunne EF, Unger ER, Sternberg M, Mc Quillan G, Swan DC, et al. (2007) Prevalence of HPV infection among females in the United States. Jama 297(8): 813-819.
-
Bazargan M, Bazargan SH, Farooq M, Baker RS (2004) Correlates of cervical cancer screening among underserved Hispanic and African-American women. Prev Med 39(3): 465-473.
-
Peterson NB, Murff HJ, Cui Y, Hargreaves M, Fowke JH. (2008) Papanicolaou testing among women in the southern United States. J Womens Health (Larchmt) 17(6): 939-946.
-
Shavers VL, Brown ML (2002) racial and ethnic disparities in the receipt of cancer treatment. J Natl Cancer Inst 94(5): 334-357.
-
Virnig BA, Baxter NN, Habermann E, Feldman RD, Bradley CJ (2009) A Matter Of Race: Early- Versus Late-Stage Cancer Diagnosis: African Americans receive their cancer diagnoses at more advanced stages of the disease than whites do. Health affairs (Project Hope) 28(1): 160-168.
-
United States Census Bureau. 2010 Census Urban Lists Record Layouts. In: United States Census Bureau.
-
Urban and Rural Population by States. In. Census.gov: Census; 2010.
-
Newmann SJ, Garner EO (2005) Social inequities along the cervical cancer continuum: a structured review. Cancer Causes Control 16(1): 63-70.
-
Evan Comen, Thomas C. Frohlich, Michael B. Sauter (2016) America’s Most and Least Educated States: A Survey of All 50.
-
Hussein AA, Welty CJ, Ameli N, Cowan JE, Leapman M, et al. (2015) Untreated Gleason Grade Progression on Serial Biopsies during Prostate Cancer Active Surveillance: Clinical Course and Pathological Outcomes. J Urol 194(1): 85-90.
-
Hsia J, Kemper E, Kiefe C, Zapka J, Sofaer S, et al. (2000) The importance of health insurance as a determinant of cancer screening: evidence from the Women's Health Initiative. Ev Med 31(3): 261-270.
-
Women’s Health Insurance Coverage. In: Foundation KF, editor. Women's Health Policy. KFF.org; 2016.
-
Source of Screening Affects Women's Eligiblity for Coverage of Breast and Cervical Cancer Treatment in Some States: United States Government Accountability Office; 2009.
-
Weaver BA (2006) Epidemiology and natural history of genital human papillomavirus infection. J Am Osteopath Assoc 106(3 Suppl 1): S2-8.
-
Asgary R, Alcabes A, Feldman R, Garland V, Naderi R, et al. (2015) Human Papillomavirus Knowledge and Attitude among Homeless Women of New York City Shelters. Womens Health Issues 25(6): 727- 731.
-
Al-Naggar RA, Low WY (2010) Isa ZM. Knowledge and barriers towards cervical cancer screening among young women in Malaysia. Asian Pac J Cancer Prev 11(4): 867-873.
-
Hawkins NA, Cooper CP, Saraiya M, Gelb CA, Polonec L (2011) Why the Pap test? Awareness and use of the Pap test among women in the United States. J Womens Health (Larchmt) 20(4): 511-515.
-
Viswanath K, Breen N, Meissner H, Moser RP, Hesse B, et al. (2006) Cancer knowledge and disparities in the information age. J Health Commun 11(1): 1-17.
-
Waller J, McCaffery K, Wardle J (2004) Beliefs about the risk factors for cervical cancer in a British population sample. Prev Med 38(6): 745-753.
-
Tiro JA, Meissner HI, Kobrin S, Chollette V (2007) What do women in the U.S. know about human papillomavirus and cervical cancer? Cancer Epidemiol Biomarkers 16(2): 288-294.
-
Cates JR, Brewer NT, Fazekas KI, Mitchell CE, Smith JS (2009) Racial differences in HPV knowledge, HPV vaccine acceptability, and related beliefs among rural, southern women. The Journal of Rural Health 25(1):93-97.
-
Wright TC, Jr. Cox JT, Massad LS, Carlson J, Twiggs LB, et al. (2013) 2001 consensus guidelines for the management of women with cervical intraepithelial neoplasia. Am J Obstet Gynecol 189(1): 295-304.
-
Sirovich BE, Welch HG (2004) The frequency of Pap smear screening in the United States. J Gen Intern Med 19(3): 243-250.
-
Control CD, Prevention (2013) Cervical cancer screening among women aged 18-30 years-United States, 2000-2010. MMWR. Morbidity and mortality weekly report 61(51-52): 1038.
-
Nuovo GJ, Pedemonte BM (1990) Human papillomavirus types and recurrent cervical warts. JAMA 263(9): 1223-1226.
-
Lorincz AT, Reid R, Jenson BA, Greenberg MD, Lancaster W, et al. (1992) Human papillomavirus infection of the cervix: relative risk associations of 15 common anogenital types. Obstetrics & Gynecology 79(3): 328-337.
-
Lorincz AT, Reid R (1989) Association of human papillomavirus with gynecologic cancer. Current opinion in oncology 1(1): 123-132.
-
Schiffman M, Wentzensen N (2010) From human papillomavirus to cervical cancer. Obstet Gynecol 116(1): 177-185.
-
Brotherton JM, Fridman M, May CL, Chappell G, Saville AM, et al. (2011) Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study. Lancet 377(9783): 2085-2092.
-
Gertig DM, Brotherton JM, Budd AC, Drennan K, Chappell G, et al. (2013) Impact of a population- based HPV vaccination program on cervical abnormalities: a data linkage study. BMC Med 11: 227.
-
Brewer NT, Reiter PL (2007) Re: Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women. J Natl Cancer Inst 102(19): 1517-1518.
-
Reagan-Steiner S (2016) National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years—United States, 2015. MMWR. Morbidity and Mortality Weekly Report 65(33): 850-858.
-
Sudenga SL, Royse KE, Shrestha S (2011) Role and uptake of human papillomavirus vaccine in adolescent health in the United States. Adolescent health, medicine and therapeutics 2011(2): 63.
-
Wong LP, Sam IC (2010) Ethnically diverse female university students' knowledge and attitudes toward human papillomavirus (HPV), HPV vaccination and cervical cancer. Eur J Obstet Gynecol Reprod Biol 148(1): 90-95.
-
Wilson AR, Hashibe M, Bodson J, Gren LH, Taylor BA, et al. (2016) Factors related to HPV vaccine uptake and 3-dose completion among women in a low vaccination region of the USA: an observational study. BMC Womens Health 16: 41.
-
Brewer NT, Fazekas KI (2007) Predictors of HPV vaccine acceptability: a theory-informed, systematic review. Prev Med 45(2-3): 107-114.
-
Moss JL, Reiter PL, Brewer NT (2005) Correlates of human papillomavirus vaccine coverage: a state- level analysis. Sex Transm Dis 42(2): 71-75.
-
Link BG, Phelan JC (2001) Conceptualizing stigma. Annual review of Sociology pp: 363-385.
-
Weiss MG, Ramakrishna J (2006) Stigma interventions and research for international health. Lancet 367(9509): 536-538.
-
Earnshaw VA, Chaudoir SR (2009) From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS Behav 13(6): 1160-1177.
-
ErvingGoffman S. Notes on the Management of Spoiled Identity. Englewood Cliffs, New Jersey: Pren-tice-Hall 1963.
-
Lebel S, Devins GM (2008) Stigma in cancer patients whose behavior may have contributed to their disease. Future Oncol 4(5): 717-733.
-
Kahn JA, Slap GB, Bernstein DI, Tissot AM, Kollar LM, et al. (2007) Personal meaning of human papillomavirus and Pap test results in adolescent and young adult women. Health Psychol 26(2): 192- 200.
-
McCaffery K, Irwig (2005) Australian women's needs and preferences for information about human papillomavirus in cervical screening. Journal of Medical Screening 12(3): 134-141.
-
Ohaeri JU, Campbell OB, Ilesanmil AO, Ohaeri BM (1998) Psychosocial concerns of Nigerian women with breast and cervical cancer. Psychooncology 7(6): 494-501.
-
Perrin KK, Daley EM, Naoom SF, Packing-Ebuen JL, Rayko HL, et al. (2006) Women's reactions to HPV diagnosis: insights from in-depth interviews. Women Health 43(2): 93-110.
-
Waller J, Marlow LA, Wardle J (2007) The association between knowledge of HPV and feelings of stigma, shame and anxiety. Sex Transm Infect 83(2): 155-159.
-
Cunningham SD, Kerrigan D, Pillay KB, Ellen JM (2005) Understanding the role of perceived severity in STD-related care-seeking delays. Journal of Adolescent Health 37(1): 69-74.
-
Liu H, Detels R, Li X, Ma E, Yin Y, et al. (2008) Stigma, delayed treatment, and spousal notification among male patients with sexually transmitted disease in China. Sexually transmitted diseases 29(6): 335-343.
-
Lichtenstein B, Neal TM, Brodsky SL (2008) The stigma of sexually transmitted infections: Knowledge, Attitudes, and an educationally-based intervention. Health Educ Monogr ser 25: 28-33.
-
Cunningham SD, Kerrigan DL, Jennings JM, Ellen JM (2009) Relationships between Perceived STD- Related Stigma, STD-Related Shame and STD Screening Among a Household Sample of Adolescents. Perspect Sex Reprod Health 41(4): 225-230.
-
Han HR, Kim J, Lee JE, Hedlin HK, Song H, et al. (2011) Interventions that increase use of Pap tests among ethnic minority women: a meta‐analysis. Psycho‐Oncology 20(4): 341-351.
-
Baron RC, Rimer BK, Breslow RA, Coates RJ, Kerner J, et al. (2008) Client-directed interventions to increase community demand for breast, cervical, and colorectal cancer screening a systematic review. Am J Prev Med 35(1): S34-55.
-
Black ME, Yamada J, Mann V (2002) A systematic literature review of the effectiveness of community- based strategies to increase cervical cancer screening. Can J Public Health 93(5): 386-393.
-
Cancer Facts & Figures for African Americans 2016- 2018. In. American Cancer Society.
-
Scarinci IC, Litton AG, Garces-Palacio IC, Partridge EE, Castle PE (2013) Acceptability and usability of self-collected sampling for HPV testing among African-American women living in the Mississippi Delta. Womens Health Issues 23(2): e123-30.
-
Arbyn M, Verdoodt F, Snijders PJ, Verhoef VM, Suonio E, et al. (2004) Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: a meta-analysis. The lancet oncology 15(2): 172-183.
-
Sultana F, English DR, Simpson JA, Brotherton JM, Drennan K, et al. (2005) Rationale and design of the iPap trial: a randomized controlled trial of home- based HPV self-sampling for improving participation in cervical screening by never- and under-screened women in Australia. BMC Cancer 14: 207.
-
McCaffery K, Forrest S, Waller J, Desai M, Szarewski A, et al. (2003) Attitudes towards HPV testing: a qualitative study of beliefs among Indian, Pakistani, African-Caribbean and white British women in the UK. Br J Cancer 88(1): 42-46.
-
Shepherd MA, Gerend MA (2013) The blame game: cervical cancer, knowledge of its link to human papillomavirus and stigma. Psychol Health 29(1): 94-109.
-
Kwan TT, Tam KF, Lee PW, Lo SS, Chan KK, et al. (2010) De-stigmatising human papillomavirus in the context of cervical cancer: a randomised controlled trial. Psychooncology 19(12): 1329- 1339.
-
National Vaccine Advisory Committee (2016) Overcoming Barriers to Low HPV Vaccine Uptake in the United States: Recommendations from the National Vaccine Advisory Committee: Approved by the National Vaccine Advisory Committee on June 9, 2015. Public Health Rep 131(1): 17-25.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria