Factors Affecting the Occurrence of Brain Metastases: A Descriptive Study on Cancer Patients of University Hospital Center Notre-Dame De Secours, Jbeil- Lebanon, between 2010 And 2015
Introduction: Brain metastases are the most important neurologic complication of cancer. Their incidence and time of appearance increase due to improved techniques for early diagnosis and therapeutic progress. Objectives:This descriptive, retrospective study aims to compare the data on the occurrence of brain metastases in cancer patients of University Hospital Notre-Dame de Secours, Jbeil- Lebanon between 2010 and 2015 with those of the literature. Methods: 102 patients were included according to specific criteria. The number and location of brain metastases have been noted. The dependent variable is the time between the diagnosis of primary cancer and that of brain metastases. The data was analyzed with SPSS 20 (Statistical Package for Social Science). The association between the variables was analyzed with the Student and Mann- Whitney test. The Spearman Test used for the correlation between 2 quantitative variables and survival evaluated by the Kaplan-Meier method. Results: The male gender, diabetes, smoking> 50 PA and breast cancer are associated with a shorter interval till the diagnosis of brain metastases. No significant effect of previous malignancy, hypertension, dyslipidemia, coronary artery disease, histologic grade or primary tumor size was found to influence the duration between primary cancer and brain metastases. Discussion: The small vessel ischemic disease seems to accelerate the development of early brain metastases that may similarly, explain the association with diabetes. Smoking would facilitate the spread of tumor cells, thus an earlier onset of metastases. As for breast cancer and the male sex, our results are consistent with the literature. Conclusion: An early spread of malignancy is associated with male gender, diabetes, smoking and breast cancer. Understanding these factors is essential to develop treatment or even preventive regimens.
Background
Brain metastases are one of the most important neurologic complications of cancer accounting for 9- 17% based on various studies [1]. Their incidence is found to be increasing due to improved imaging techniques (magnetic resonance imaging, MRI) resulting in early diagnosis of small lesions, as well as, improved treatment regimens allowing for their occurrence, more frequently, at late-stage disease [1].
Therefore, time from primary cancer to brain metastases diagnosis is increasing [2].
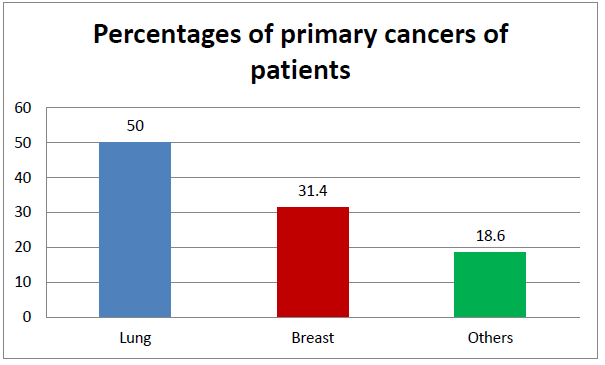
Carcinomas such as lung, breast, kidney and colorectal cancers, melanoma are the most common primary tumors responsible for BM [3, 4, 5, 6]. Lung cancer is the most common primary cancer associated with BM (40-50%) [3, 7]. In fact, pulmonary source is identified as origin of BM in more than 25% of all autopsy-proven brain metastases [8]. Whereas, carcinomas of the prostate, esophagus, oropharynx and other types of skin cancers rarely metastasize to the brain [4, 6]. Patients with brain metastases may present with a variety of symptoms and signs: general, focal, or often, a combination of the two [5]. Generalized impaired cognitive function, hemiparesis, headaches are common presentations (50-60%); while seizures (18%), aphasia (18%) and visual field deficit (7%) are less common [5].
18% out 195 patients with brain metastases presented with seizures and 10% developed late seizures up to 59 weeks from the diagnosis of intracerebral metastases [9]. In addition, seizures are almost exclusively associated with supratentorial disease [9]. Contrast- enhanced MRI is the preferred test for the diagnosis of brain metastases, where they usually appear as well- circumscribed lesions with a variable amount of perilesional edema and a ring pattern or diffuse enhancement [5]. Biopsy is rarely required, and it should be performed when the diagnosis is in doubt [5].
Materials and Methods
Ethics
Since we are conducting an observational study that respects participants’ autonomy and confidentiality and doesn’t induce harm to them, the Institutional Review Board of our hospital waived the need for an approval.
Objectives
This study aims to compare the data on the occurrence of brain metastases in cancer patients of University hospital center Notre-Dame de Secours, Jbeil- Lebanon between 2010 and 2015, with those of the literature.
Study Population
This descriptive, retrospective study was conducted between January 2010 and December 2015. Cases were chosen from the University hospital center Notre-Dame de Secours, located in Jbeil, Lebanon. The records of all patients with brain metastases who underwent whole brain radiotherapy and chemotherapy from 2010 to 2015 were retrospectively reviewed.
Procedure
Medical records of a total of 102 patients were reviewed regarding sex, age, history of seizure and vascular risk factors including pack-year smoking history, hypertension, diabetes mellitus (DM), dyslipidemia, prior percutaneous coronary intervention or coronary artery bypass graft evidence of coronary artery disease (CAD). The primary cancer and the date of its diagnosis and the one of the brain metastases was noted. Brain imaging of the patients were reviewed and the number and locations of the lesions was determined.
Inclusion and Exclusion Criteria
Patients with documented histopathological diagnosis of cancer by a needle, endoscopic or surgical biopsy and with brain metastases on brain imaging (computed tomography or magnetic resonance imaging) and who underwent whole brain radiotherapy and chemotherapy were included, while patients with unavailable histopathological diagnosis or unavailable CT or MRI of the brain, or who underwent prophylactic brain radiotherapy were not included.
Statistical Analysis
With a confidence interval of 95% and a margin of error of 5%, the data were analyzed using SPSS (Statistical Package for Social Science) Version 20. Quantitative variables are expressed as mean ± Standard Deviation (SD) type and qualitative variables as a percentage. A value of P <0.05 was considered significant. Clinical Risk factors were searched using bivariate analysis. Indeed, Comparisons for the quantitative data were carried out between groups using Student Test or Mann-Whitney Test for small samples. Comparisons of quantitative variables were made using the correlation of Spearman.
Metastasis and Duration between tumor and cerebral metastasis were considered as time- dependent data and were analyzed with survival data analysis methods (Kaplan-Meir Test). The Dependent variable in the study is: duration between tumor and metastasis.
Results
Table 1 displays the characteristics of all 102 patients. Patients were predominantly females (55.9%, n=57) and had a median age of 57.19 ± 12.63 years with a range from 28 to 84 years. Vascular risk factors of 85
patients were reviewed: 14 patients (16.5%) had a hypertension, 12 patients (14.1%) had DM, 7 patients (8.2%) had dyslipidemia and 6 patients (7.1%) had evidence of CAD. 15 patients out of 25 had > 50 pack- year smoking history.
lobe (54.9%, n=56), the cerebellum (45.1%, n=46) and the parietal lobe (34.3%, n=35). The temporal lobe (19.6%, n=20), the occipital lobe (13.7%, n=14), the basal ganglia (7.8%, n=8), the brain stem (12.7%, n=13) and the diencephalon (3.9%, n=4) were less commonly involved (Figure 1).Moreover, 8 of 102 patients (7.8%) had a seizure (Figure 2). The dependent variable in the study is the duration between tumor and brain metastasis which is found to be 25.96 ± 34.51 months with a range from 1 to 180 months.
58 patients (56.9%) had [0, 1, 2, 3] brain metastases, 14 patients (13.7%) had [3, 4, 5, 6] brain metastases and 30 patients (29.4%) had > 6 brain metastases. The most common brain metastases locations were: the frontal
| Number | Percentage (%) | ||
|---|---|---|---|
| Sex | Men | 45 | 44.1 |
| Sex | Women | 57 | 55.9 |
| History of other malignancy | Yes | 5 | 7.5 |
| History of other malignancy | No | 62 | 92.5 |
| History of hypertension | Yes | 14 | 16.5 |
| History of hypertension | No | 71 | 83.5 |
| History of DM | Yes | 12 | 14.1 |
| History of DM | No | 73 | 85.9 |
| History of dyslipidemia | Yes | 7 | 8.2 |
| History of dyslipidemia | No | 78 | 91.8 |
| Evidence of CAD | Yes | 6 | 7.1 |
| Evidence of CAD | No | 79 | 92.9 |
| Pack-year smoking history | < or = 50 | 10 | 40 |
| Pack-year smoking history | > 50 | 15 | 60 |
| Breast cancer | Yes | 32 | 31.4 |
| Breast cancer | No | 70 | 68.6 |
| Lung cancer | Yes | 51 | 50 |
| Lung cancer | No | 51 | 50 |
| Histologic grade | Poorly differentiated | 15 | 57.7 |
| Histologic grade | Moderately differentiated | 11 | 42.3 |
| Tumor size in centimeters (cm) | < or = 4 | 12 | 70.6 |
| Tumor size in centimeters (cm) | > 4 | 5 | 29.4 |
| Surgical removal of primary tumor | Yes | 47 | 46.5 |
| Surgical removal of primary tumor | No | 54 | 53.5 |
| Surgical removal of brain metastases | Yes | 8 | 8.1 |
| Surgical removal of brain metastases | No | 91 | 91.9 |
| Number of cerebral metastases | [0-3] | 58 | 56.9 |
| Number of cerebral metastases | [3-6] | 14 | 13.7 |
| Number of cerebral metastases | >6 | 30 | 29.4 |
| Frontal lobe | Yes | 56 | 54.9 |
| Frontal lobe | No | 46 | 45.1 |
| Parietal lobe | Yes | 35 | 34.3 |
| Parietal lobe | No | 67 | 65.7 |
| Temporal lobe | Yes | 20 | 19.6 |
| Temporal lobe | No | 82 | 80.4 |
| Occipital lobe | Yes | 14 | 13.7 |
| Occipital lobe | No | 88 | 86.3 |
| Basal ganglia | Yes | 8 | 7.8 |
| Basal ganglia | No | 94 | 92.2 |
| Cerebellum | Yes | 46 | 45.1 |
| Cerebellum | No | 56 | 54.9 |
| Brain stem | Yes | 13 | 12.7 |
| Brain stem | No | 89 | 87.3 |
| Diencephalon | Yes | 4 | 3.9 |
| Diencephalon | No | 98 | 96.1 |
| Number of extra cerebral metastases | [0-3] | 61 | 73.5 |
|---|---|---|---|
| ]3-6] | 7 | 8.4 | |
| >6 | 15 | 18.1 | |
| Liver metastases | [0-3] | 70 | 88.6 |
| >6 | 9 | 11.4 | |
| Bone metastases | [0-3] | 66 | 84.6 |
| ]3-6] | 5 | 6.4 | |
| >6 | 7 | 9 | |
| Seizure | Yes | 8 | 7.8 |
| No | 94 | 92.2 | |
| Size of the largest brain metastases in millimeters (mm) | N= 61/ Min=3/Max=65 | 23.41 ± 14.68 | |
| Delta in months | N= 95/ Min=1/ Max=180 | 25.96 ± 34.51 | |
| Age in years | N= 102/ Min= 28/ Max= 84 | 57.19 ± 12.63 |
Table 2: Characteristics of all patients.
| Primary cancer | Number | Percentage (%) |
|---|---|---|
| Breast cancer | 32 | 31.4 |
| Lung cancer | 51 | 50.0 |
| Pancreatic cancer | 2 | 2.0 |
| Colorectal cancer | 3 | 2.9 |
| Skin cancer | 3 | 2.9 |
| Ovarian cancer | 1 | 1.0 |
| Renal cancer | 1 | 1.0 |
| Anal cancer | 4 | 3.9 |
| Prostate cancer | 1 | 1.0 |
| Bladder cancer | 1 | 1.0 |
| Endometrial cancer | 1 | 1.0 |
| Vulvar cancer | 1 | 1.0 |
| Mediastinal cancer | 1 | 1.0 |
| Qualitative variables are expressed as a percentage. |
Table 3: Percentage of primary cancer locations.
The results showed that the duration between tumor and brain metastases in men (12.34 ± 16.88 months) is significantly less than in women (37.71 ± 41.13 months) with a P=0.0001 and a significant negative correlation with age was identified (Correlation of Spearman= - 0.251; P=0.014)
History of DM was significantly associated with shorter duration between tumor and brain metastases (9.75 ± 12.26 months, P=0.004) compared to non- diabetic patients.
In addition, patients with more than 50 pack-year smoking history had significantly shorter duration between tumor and brain metastases (10.93 ± 15.224 months, P=0.032) compared to those with ≤ 50 pack- year smoking history.
Patients with breast cancer develop brain metastases significantly in 51.67 ± 45.46 months (P=0.0001) and patients with lung cancer significantly in 7.37 ± 9.69 months. When comparing these two types of cancer, patients with breast cancer develop brain metastases significantly more rapidly than patients with lung cancer (P=0.0001).
Furthermore, 2 patients (6.7%) out of 30 with breast cancer had developed brain metastasis in ≤ 1 month, while 26 patients (56.5%) out of 46 with lung cancer had brain metastases in ≤ 1 month.
It was found that patients who underwent surgical removal of primary tumor develop brain metastases significantly in 41 ± 32.9 months (P=0.0001). No significant effect of prior malignancy, hypertension, dyslipidemia, CAD, histologic grade, or primary tumor size was found on the duration between tumor and brain metastases (Table 3).
| Independent variables | N | Mean ± SD | P value | |
|---|---|---|---|---|
| Sex | Men | 44 | 12.34 ± 16.88 | 0.0001* |
| Sex | Women | 51 | 37.71 ± 41.13 | 0.0001* |
| History of malignancy | Yes | 5 | 11.4 ± 20.57 | 0.188 |
| History of malignancy | No | 57 | 23.96 ± 31.66 | 0.188 |
| History of hypertension | Yes | 13 | 26.02 ± 47.57 | 0.699 |
| History of hypertension | No | 65 | 24.02 ± 27.66 | 0.699 |
| History of DM | Yes | 12 | 9.75 ± 12.26 | 0.004* |
| History of DM | No | 66 | 27.02 ± 33.16 | 0.004* |
| History of dyslipidemia | Yes | 7 | 27.14 ± 41.85 | 0.993 |
| History of dyslipidemia | No | 71 | 24.08 ± 30.61 | 0.993 |
| Evidence of CAD | Yes | 6 | 16.33 ± 23.76 | 0.254 |
| Evidence of CAD | No | 72 | 25.03 ± 32.04 | 0.254 |
| Pack-year smoking history | < or = 50 | 9 | 24.56 ± 17.56 | 0.032* |
| Pack-year smoking history | > 50 | 15 | 10.93 ± 15.224 | 0.032* |
| Breast cancer | Yes | 30 | 51.67 ± 45.46 | 0.0001* |
| Breast cancer | No | 65 | 14.09 ± 18.96 | 0.0001* |
| Lung cancer | Yes | 46 | 7.37 ± 9.69 | 0.0001* |
| Lung cancer | No | 49 | 43.41 ± 40.030 | 0.0001* |
| Breast/Lung cancer | Breast | 30 | 51.67 ± 45.46 | 0.0001* |
| Breast/Lung cancer | Lung | 46 | 7.37 ± 9.69 | 0.0001* |
| Histologic grade | 1 | 15 | 39 ± 39.65 | 0.131 |
| Histologic grade | 2 | 11 | 19.73 ± 19.52 | 0.131 |
| Tumor size | < or = 4 | 12 | 30.67 ± 33.8 | 0.315 |
| Tumor size | > 4 | 5 | 14.8 ± 16.09 | 0.315 |
| Surgical removal of primary tumor | Yes | 44 | 41 ± 32.9 | 0.0001* |
| Surgical removal of primary tumor | No | 50 | 13.22 ± 30.8 | 0.0001* |
| Age at diagnosis | Correlation of Spearman = - 0.251 | 0.014* |
Table 4: Association of different variables with the duration between tumor and metastases in months.
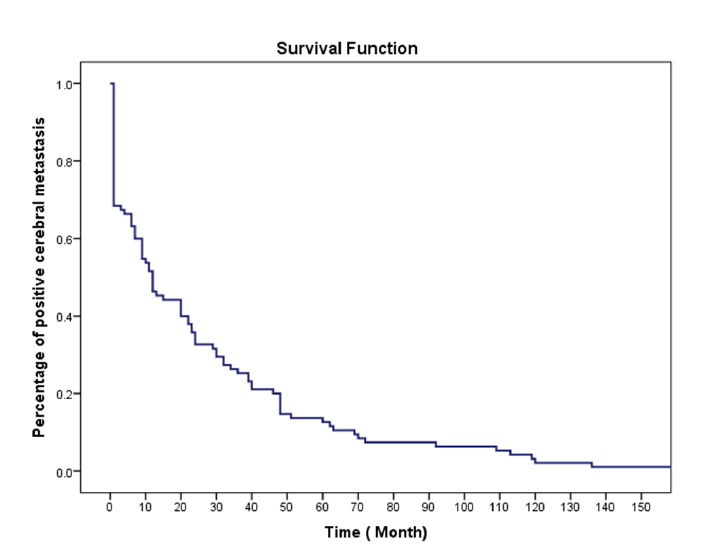
In Table 4, survival analysis was conducted based on the duration between tumor and brain metastases in months and the number of cases and cumulative number of cases were obtained. The survival function is shown in Figure 4.
| 30% | 40% | 50% | 60% | 70% | 80% | 100% | |
| Duration between tumor and brain metastases (in months) | 1 | 7 | 11 | 20 | 30 | 46 | 180 |
| Number of cases (cumulative number of cases) | 30 | 8(38) | 8(46) | 11(57) | 10(67) | 9(76) | 19(95) |
Table 5: Survival analysis.
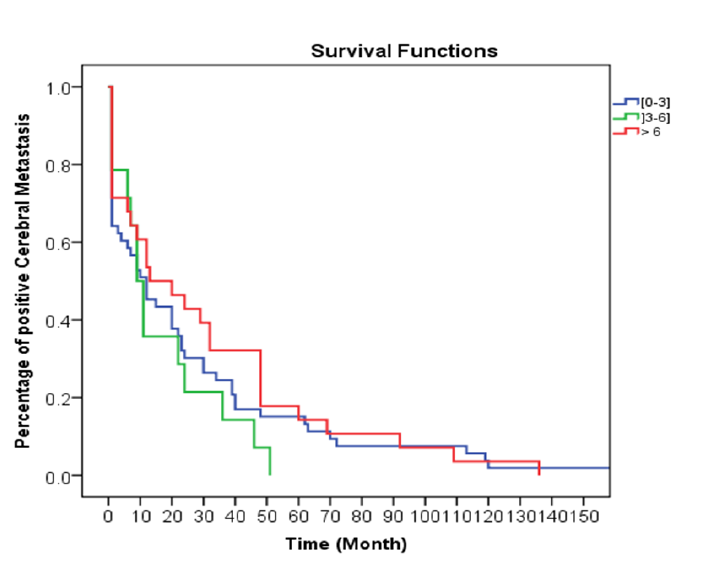
The latter was separated based on the number of brain metastases: [0, 1, 2, 3], [3, 4, 5, 6] and >6. This is shown in Figure 5.
Discussion
The most common source of BM was found to be lung cancer (40-50%), which meets our results [5, 10].
Therefore, patients with brain metastases of unknown origin should undergo evaluation mainly for a lung cancer [10]. In a retrospective series that included 470 patients with brain metastases, seizures were diagnosed in 24% at some point during the illness [11]. While in our study, only 7.8% have presented a seizure at some point throughout the illness.
While studying the number of brain metastases on computed-tomography scans of 288 patients: one brain metastasis was found in 49%, two in 21%, three in 13%, four in 6% and five or more in 11% of scans [12]. Furthermore, breast, colon, and renal cell carcinoma produce more often single brain metastases, while lung cancer and malignant melanoma tend to produce multiple ones [12]. Several factors are thought to influence the risk of development of brain metastases including white matter lesions which are associated with lower number of brain metastases in different cancer types [13]. These lesions, which are common in patients with vascular risk factors, are signs of small vessel disease and reduced perfusion to the brain and thus, less brain metastases than patients without white matter lesions [13]. Another study done by Mazzone, et al. has shown that small vessel ischemic disease (SVID) of the brain, detected on MRI, is a protective factor against the development of BM and high grades of SVID are found in patients without BM [14]. Other factors found to increase the risk of developing brain metastases in patients with non-small cell lung cancer for example, include a young age, large tumor size, lymphovascular space invasion, and hilar lymph node involvement [15]. Furthermore, a recent study concluded that patients with peripheral arterial occlusive disease had significant less brain metastases compared to patients without peripheral arterial occlusive disease; while no single vascular risk factor (arterial hypertension, DM, smoking, hypercholesterolemia) had a significant influence on the number of brain metastases [16]. However, our study results have shown that DM was associated with a shorter duration between primary cancer and brain metastases compared to non-diabetic patients.
Few studies have discussed the duration between primary cancer and brain metastases: out of 238726 adult patients with invasive breast cancer between 2010 and 2013, [17] 968 patients had brain metastases at the time of diagnosis which corresponds to 0.41%. Shaw et al. have studied the association between smoking and metastases particularly in melanoma; it was found that smoking did facilitate the spread of metastases which meets our findings [18]. Another study on breast cancer reported an earlier spread of malignant disease with tobacco usage and obesity [19]. Regarding the distribution of brain metastases, they are usually situated at the grey-white matter junction and more common at the terminal “watershed areas” of arterial circulation, suggesting that tumoral microemboli tend to get trapped in the capillaries of the distal portions of the superficial arteries [12, 20].
Cerebral hemispheres are the most common location, approximately 80%, while cerebellum and brainstem lesions accounts only for 15% and 5%, respectively [12]. A more recent study suggests a predominant involvement of the cerebellum in breast cancer and of the occipital lobe and the cerebellum in non-small cell lung cancer and 85% (734 out of 864 lesions) are located at the grey-white matter junction [20]. This may indicate a difference vulnerability to metastasis in the different areas of the brain [20]. Currently, researchers are studying the relationship between tumor’s molecular biological characteristics such as epidermal growth factor receptor mutation status and the spatial distribution of brain metastases [21].
Study Strengths
Our research is the first to include cancer patient’s records for a whole 6 years, from 2010 to 2015, and the first to describe brain metastases data and compare them to the literature, at University hospital center Notre-Dame de Secours. In addition, our work is one of the few to report association between the duration between primary cancer and brain metastases and the studied variables.
Study Limitations
The first limitation is the small number of patients in our study, limiting our significant results. Second, vascular risk factors were obtained only for a small group of patients because of missing data, otherwise an association between these factors and the number of brain metastases or the duration from the diagnosis of primary disease to their appearance might have been found. The third limitation is that no biological markers or receptors were studied; their association with brain metastases would have complemented our study.
Conclusion
In this retrospective study conducted between 2010 and 2015, in University hospital center Notre-Dame de Secours, Jbeil-Lebanon, an earlier spread of malignancy was found to be associated with male gender, diabetes mellitus, smoking and breast cancer. Lung cancer and breast cancer were the most common primary diseases.
The frontal lobe and the cerebellum were the most common sites of brain metastases. 7.8% of patients had a seizure during their illness. No significant effect of prior malignancy, hypertension, dyslipidemia, CAD, histologic grade, or primary tumor size was found on the duration between tumor and brain metastases.
Understanding the unique brain microenvironment is of great importance nowadays because it may lead us to better understanding of the development of brain metastases and thus, to more efficient therapies and to a lower incidence of brain metastases.
References
-
Nayak L, Lee EQ, Wen PY (2012) Epidemiology of brain metastases. Curr Oncol Rep 14(1): 48-54.
-
Tabouret E, Bauchet L, Carpentier AF (2013) Épidémiologie des métastases cérébrales et tropisme cérébral. Bull Cancer 100(1): 57-62.
-
Johnson JD, Young B (1996) Demographics of brain metastasis. Neurosurg Clin N Am 7(3): 337-344.
-
Schouten LJ, Rutten J, Huveneers HAM, Twijnstra A (2002) Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 94(10): 2698- 2705.
-
DeAngelis LM, Wen PY (2015) Primary and Metastatic Tumors of the Nervous System. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson JL, et al. (Eds.), Harrison’s Principles of Internal Medicine, 19e. New York, NY: McGraw-Hill Education.
-
Barnholtz Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, et al. (2004) Incidence Proportions of Brain Metastases in Patients Diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 22(14): 2865-2872.
-
Sul J, Posner JB (2007) Brain Metastases: Epidemiology and Pathophysiology. Brain Metastases. Boston, MA: Springer US 1-21.
-
Gavrilovic IT, Posner JB (2005) Brain metastases: Epidemiology and pathophysiology. J Neurooncol 75(1): 5-14.
-
Cohen N, Strauss G, Lew R, Silver D, Recht L (1988) Should prophylactic anticonvulsants be administered to patients with newly-diagnosed cerebral metastases? A retrospective analysis. J Clin Oncol 6(10): 1621-1624.
-
Wen PY, Loeffler JS (1999) Management of brain metastases. Oncology (Williston Park) 13(7): 941- 954, 957-61-2, 9.
-
Lynam LM, Lyons MK, Drazkowski JF, Sirven JI, Noe KH, et al. (2007) Frequency of seizures in patients with newly diagnosed brain tumors: A retrospective review. Clin Neurol Neurosurg 109(7): 634-638.
-
Delattre J, Krol G, HT T, JB P (1988) Distribution of brain metastases. Arch Neurol 45(7): 741-744.
-
Berk BA, Nagel S, Hering K, Paschke S, Hoffmann KT, et al. (2016) White matter lesions reduce number of brain metastases in different cancers: a high-resolution MRI study. J Neurooncol 130(1): 203-209.
-
J Mazzone P, Marchi N, Fazio V, Taylor MJ, Masaryk T, et al. (2009) Small Vessel Ischemic Disease of the Brain and Brain Metastases in Lung Cancer Patients. PLoS One 4: e7242.
-
Hubbs JL, Boyd JA, Hollis D, Chino JP, Saynak M, et al. (2010) Factors associated with the development of brain metastases. Cancer 116(21): 5038-5046.
-
Nagel S, Berk BA, Kortmann RD, Hoffmann KT, Seidel C (2018) Can vascular risk factors influence number and size of cerebral metastases? A 3D-MRI study in patients with different tumor entities. Clin Neurol Neurosurg 165: 55-59.
-
Martin AM, Cagney DN, Catalano PJ, Warren LE, Bellon JR, et al. (2017) Brain metastases in newly diagnosed breast cancer: A population-based study. JAMA Oncol 3(8): 1069-1077.
-
Shaw HM, Milton GW (1981) Smoking and the development of metastases from malignant melanoma. Int J Cancer 28(2): 153-156.
-
Daniell HW (1988) Increased lymph node metastases at mastectomy for breast cancer associated with host obesity, cigarette smoking, age, and large tumor size. Cancer 62(2): 429-435.
-
Quattrocchi CC, Errante Y, Gaudino C, Augusto C, Giona MA, et al. (2012) Spatial brain distribution of intra-axial metastatic lesions in breast and lung cancer patients. J Neurooncol 110(1): 79-87.
-
Takano K, Kinoshita M, Takagaki M, Sakai M, Tateishi S, et al. (2016) Different spatial distributions of brain metastases from lung cancer by histological subtype and mutation status of epidermal growth factor receptor. Neuro Oncol 18(5): 716-724.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria