The Effect of the COVID-19 Pandemic on Pediatric Respiratory Hospitalizations
Background: The COVID-19 pandemic has dramatically influenced all aspects of clinical work worldwide. Data coming from the southern hemisphere reported less isolation of common winter viruses. This study evaluated annual trends in respiratory diseases’ related admissions before and during the COVID-19 pandemic. Methods: In this retrospective analysis we compared Electronic Medical Records (EMR) of respiratory hospitalizations from November 2020 through January 2021 to the same period in the previous two years. We collected data regarding number of admissions, epidemiological and clinical presentation, and isolation of respiratory pathogens. Results: There were 1488 respiratory hospitalizations (58% males) over the three winter seasons in three general pediatric wards (632 in 2018-2019, 701 in 2019-2020 and 155 in 2020-2021). Daily admissions decreased significantly during the COVID-19 pandemic from median values of 6 per day (Interquartile range - IQR 4-9) and 7 per day (IQR 6-10) for 2018-2019 and 2019-2020 respectively to only 1 per day (IQR 1-3) (p value < 0.001). Overall, hospitalizations due to lower respiratory tract infections (LRTI) were more common than upper tract infections (URTI). The incidence of all respiratory viruses decreased significantly during the COVID-19 pandemic, with no hospitalizations due to influenza virus and only 1 patient with respiratory syncytial virus (RSV). In addition, there was a significant decline in respiratory viral and bacterial co-infections during the 2020-2021 seasons (p value < 0.001). Conclusion: There was a significant decline in the burden of respiratory diseases in children during the COVID-19 pandemic. Possible etiologies include epidemiological factors such as mask wearing, social distancing and recurrent lockdowns, as well as closure of schools and kindergartens, in addition to biological factors such as viral interference. A herd protection effect of adults and older children wearing masks may also have had an impact.
Introduction
Every winter, pediatric outpatient clinics and hospital wards are over flooded with children who suffer from infectious respiratory diseases such as RSV bronchiolitis, influenza A and B infections and many other respiratory pathogens causing upper and lower respiratory tract infections in the pediatric population [1, 2].
RSV is the leading cause of acute lower respiratory infections in children. By the age of 1 year, 60–70% of children have been infected. Hospitalization rate is as high as 2%–3%. In Israel, most RSV cases are reported from the beginning of November to the end of February [3]. Influenza affects an average of 20–30% of the pediatric population annually [4]. Influenza season in the northern hemisphere begins in December, peaks at January, and extends to February [5].
The COVID-19 pandemic, originated in Wuhan province, China, in December 2019 had spread all over the world with increasing and alarming morbidity and mortality. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has already infected over 100 million people and resulted in over 2.1 million deaths globally [6]. The accumulating knowledge concerning this pandemic, as well as previous epidemiological and public health data has led to the development of widespread infection prevention strategies including mandatory wearing of surgical masks, hand sanitation and social distancing. In an attempt to control the spreading disease, the Israeli government has imposed three nationwide quarantine orders (14th March - 9th May 2020, 18th September-17th October 2020 and recently 8th January-7th February 2021) meaning closure of all educational facilities and airports, limitations on travelling and a significant reduction in out-of-house employment as well as cancellation of all social events.
Globally speaking, such measures have raised questions regarding how the current 2020-2021 winter season would look like in terms of respiratory infectious illnesses other than COVID-19 related disease. Several assumptions were made based on expert opinion and data from the southern hemisphere, which foresaw a significant reduction in respiratory diseases’ related hospital admissions [7, 8, 9]. The aim of this novel study is to assess the number and profile of hospitalizations due to respiratory diseases before and during the pandemic, specifically during the winter season, as opposed to the same time in previous years.
Methods
This retrospective observational study was conducted at Schneider Children’s Medical Center, the largest, university affiliated, tertiary pediatric hospital in Israel. We analyzed electronic medical records (EMR) of children 0-18 years old, hospitalized due to respiratory diseases in all three general wards. The study period was the winter months of November 1st 2020 to January 31st 2021 (season 3) as compared to the same period in the years 2018-2019 (season 1) and 2019- 2020 (season 2), relying on the fact that no COVID-19 cases were recorded in Israel before February 2020.
We used the hospital database and filtered the search according to ICD-9 codes for “pneumonia”, “wheezing”, “asthma”, “viral infection”, “bronchiolitis”, “dyspnea or tachypnea”, “RSV”, “influenza”, “adenovirus” as well as hospitalizations due to COVID-19. Each case was reviewed by the researchers and demographic, clinical and microbiological data was collected. Upper respiratory tract disease was defined when the main complaints were nasal discharge with or without coughing [10] as well as stridor. Lower respiratory tract disease was defined when there were wheezing or increased breath sounds over the lungs, signs of inflammation over the lung parenchyma in chest x-ray [11], as well as new hypoxemia in room air. Bacterial pneumonia was defined as respiratory symptoms, fever above 37.5°C or a history of fever at home, and a radiological diagnosis of pneumonia (defined as a confluent area of consolidation) [12]. Co-infection was defined as a diagnosis of bacterial pneumonia together with the isolation of a viral pathogen. Identification of a microbiological pathogen was made using Polymerase Chain Reaction (PCR) from nasal secretions or bacterial sputum cultures. We use AllplexTM RV essential assay kit, for screening 7 major viral pathogens of respiratory infections (Adenovirus, Influenza A, Influenza B, Human Metapneumovirus, Parainfluenza, RSV, Human rhinovirus A/B/C).
Our hospital’s policy during the pandemic includes screening of SARS-COV-2 for all pediatric admissions even without fever or respiratory complaints. We have included hospitalizations associated with COVID-19 but made the distinction between admissions due to COVID-19 respiratory related symptoms as opposed to admissions due to other pediatric causes with a positive PCR for COVID-19. Re-admission under what was suspected to be the same infectious disease was considered to be one hospitalization. If the child was admitted due to a different respiratory disease, we considered it as a separate admission. In addition, children hospitalized in our pediatric intensive care unit due to severe respiratory disease, are transferred to the general pediatric ward for further care once they are clinically stable, so they are a part of the patient cohort. The primary outcome was the number of admissions per day due to respiratory diseases during the study period compared to the previous two paralleled seasons. The secondary outcomes were a comparison of the clinical and microbiological characteristics of hospitalized children in the COVID-19 era with the same period in previous years.
Statistical Analysis
Continuous variables with normal distribution are shown as mean ± standard deviation (SD), continuous variables with non-normal distribution or ordinal variables as median and interquartile range (IQR) and categorical data as sum and percentage. Univariate comparison between groups was performed with appropriate tests. Specifically, nominal variables such as sex and pathogen isolation per admission were compared via Pearson’s Chi-square test; continuous variables that fulfilled parametric criteria were compared via Student’s T-test; and ordinal and continuous non- parametric variables such as daily respiratory admissions were compared via Man-Whitney U test.
We designed a regression model to assess the risk of daily respiratory admissions during the winter season of the Covid-19 pandemic (Nov. 2020-Jan. 2021) in comparison with the same period during the two years prior to the pandemic season. Incidence rate ratio (IRR) was calculated via negative binomial regression, due to the over dispersed nature of our outcome-daily respiratory admissions. Risk for daily respiratory admissions during winter season of the Covid-19 pandemic is presented as IRR and 95% confidence interval (CI). Analysis was performed using IBM® SPSS software version 24. Significance was set as p-value ≤ 0.05. The study protocol was approved by our institutional review board committee.
Results
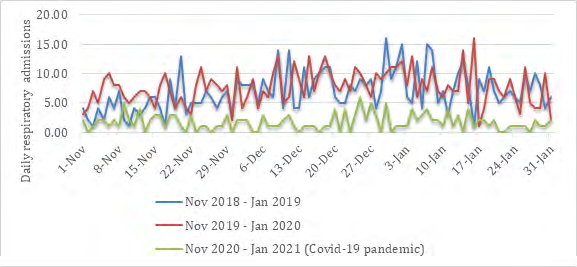
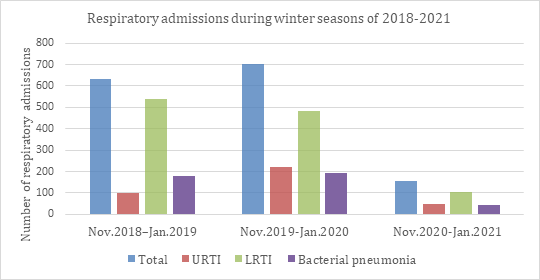
During the study period, there were 1488 respiratory disease related hospitalizations in the three general pediatric wards (632 in 2018-2019, 701 in 2019-2020 and 155 in 2020-2021); 58% were males (Table 1). Total respiratory admissions declined by 75.5% and 77.9% during the COVID-19 pandemic season in comparison with the winter seasons of 2018-2019 and 2019-2020, respectively. Daily respiratory admissions also declined significantly in comparison with the two prior winter seasons; median [and IQR] daily respiratory admissions were 6 [4, 5, 6, 7], 7 [6, 7, 8, 9, 10], and 1 [1, 2, 3] during winter seasons of 2018-2019, 2019-2020, and 2020-2021, respectively (Figures 1&2).
| Season #1 (Nov.2018-Jan.2019) N=632 | Season #2 (Nov.2019-Jan.2020) N=701 | Season #3 (Nov.2020-Jan.2021) N=155 | p-value #1 vs. #2 | p-value #1 vs. #3 | p-value #2 vs. #3 | Total N=1,488 | |
|---|---|---|---|---|---|---|---|
| Sex (male); n(%) | 364 (57.6%) | 396 (56.5%) | 103 (66.5%) | 0.684 | 0.044 | 0.023 | 863 (58.0%) |
| Age (years); median [IQR] | 1.00 [0.33-2.17] | 1.17 [0.50-2.58] | 1.58 [0.92-3.92] | 0.022 | <0.001 | <0.001 | 1.17 [0.5-2.5] |
| Daily respiratory admissions; median [IQR] | 6 [4-9] | 7 [6-10] | 1 [1-3] | 0.018 | <0.001 | <0.001 | 6 [3-8] |
| URTI; n(%) | 102 (16.1%) | 219 (31.2%) | 50 (32.3%) | <0.001 | <0.001 | 0.805 | 371 (24.9%) |
| LRTI; n(%) | 538 (85.1%) | 484 (69.0%) | 106 (68.4%) | <0.001 | <0.001 | 0.873 | 1,128 (75.8%) |
| Adenovirus; n(%) | 69 (10.9%) | 70 (10%) | 8 (5.2%) | 0.578 | 0.031 | 0.059 | 147 (9.9%) |
| HMPV; n(%) | 25 (4%) | 3 (0.4%) | 1 (0.6%) | <0.001 | 0.039 | 0.72 | 29 (1.9%) |
| Influenza; n(%) | 63 (10.0%) | 186 (26.5%) | 0 | <0.001 | <0.001 | <0.001 | 249 (16.7%) |
| RSV; n(%) | 285 (45.1%) | 240 (34.2%) | 1 (0.6%) | <0.001 | <0.001 | <0.001 | 526 (35.3%) |
| Parainfluenza; n(%) | 35 (5.5%) | 29 (4.1%) | 7 (4.5%) | 0.232 | 0.612 | 0.831 | 71 (4.8%) |
| Rhinovirus; n(%) | 1 (0.2%) | 11 (1.6%) | 19 (12.3%) | 0.006 | <0.001 | <0.001 | 31 (2.1%) |
| Sars-cov-2; n(%) | 0 | 0 | 4 (2.6%) | - | - | - | 4 (0.3%) |
| Bacterial pneumonia (total) | 177 (28.0%) | 193 (27.5%) | 43 (27.7%) | 0.847 | 0.948 | 0.958 | 412 (27.8%) |
| Respiratory co-infections | 91 (14.4%) | 142 (20.3%) | 7 (4.5%) | 0.005 | 0.001 | <0.001 | 240 (16.1%) |
Table 1: Respiratory admissions during winter season of two years prior to and one year during Covid-19 pandemic; Univariate anal
Negative binomial regression showed a significant decrease in daily admissions during the covid-19 pandemic season. The Incidence Rate Ratio (IRR) for daily admissions due to respiratory complaints during the covid-19 pandemic season in comparison with the two prior winter seasons was 0.235, (95% CI 0.174-0.318) (p value < 0.001). Median age at admission was 1.0 years old during 2018-2019 (Interquartile range - IQR 0.33-2.17), 1.17 years during 2019-2020 (IQR 0.5-2.58) and 1.58 years (IQR 0.92-3.92) for 2020-2021 (years 2020-2021) (p value < 0.001).
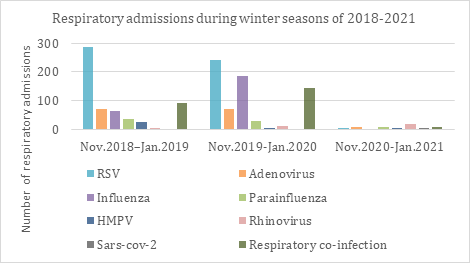
Hospitalizations due to lower respiratory tract infections (LRTI) were more common throughout the studied periods. There were 538 LRTI admissions in 2018-2019 (85.1%), 484 in 2019-2020 (69%) and only 106 in 2020-2021 (68.4%). Microbiological analysis revealed a statistically significant decrease in incidence of all viruses in 2020-2021 compared to previous seasons. Rhinovirus was introduced into the general pediatric viral respiratory PCR panel in our hospital in the season of 2019-2020, so it was only possible to compare seasons 2 and 3 in this aspect. Rhinovirus’ prevalence was the only one to have increased during the pandemic. Influenza virus infections were more common in season 2 (p value < 0.001) compared to season 1, with no hospitalizations due to the virus in season 3. Even though there was an absolute decline in the number of hospitalizations due to bacterial pneumonia during season 3 compared to season 1 and 2 (177 and 193 vs. 43, respectively), their relative percentage of respiratory admission did not change during the study periods. Interestingly, there was a significant decline in the percentage of bacterial and viral co-infections (p value < 0.001) (Figure 3).
Allover there were four hospitalizations due to a respiratory disease attributed to COVID-19, the clinical picture in three of them was of LRTI and one of URTI.
Discussion
We report a significant decline in pediatric hospitalizations due to respiratory illnesses during COVID-19 pandemic. There was a decline in all respiratory viruses except for rhinovirus. In temperate climates in the northern hemisphere, outbreak of bronchiolitis typically begins in November, peaks in January-February, and ends in the early spring [13]. Surprisingly, even during the peak season there was no isolation of influenza virus and only one isolation of RSV in our hospital. We assume that the drop in hospitalizations due to respiratory diseases is primarily due to epidemiological factors such as facemasks wearing and adherence to hand hygiene; recurrent lock downs and closure of schools and kindergartens. As vacation days and holidays were the same in all the three winter seasons, we assume it is not a relevant factor affecting the number of hospitalizations.
The high transmission rate and epidemic nature of respiratory tract viruses implies that effective public health measures could reduce transmission of these viruses and have a substantial role in their prevention [14]. Facemasks are important in reducing transmission of respiratory viruses. In general, facemasks are recommended for prevention of diseases transmitted via respiratory droplets (>5 micrometer), which are emitted mostly while coughing or sneezing, and do not spread over long distances [15, 16]. Soon after the beginning of the COVID-19 pandemic, the Center for Disease Control and Prevention (CDC) recommended that people older than 2 years should wear masks in public settings, with emphasis on teachers, staff, and students [17]. RSV is a highly contagious virus and is transmitted mainly via direct contact with respiratory droplets. Strict hand hygiene, including frequent hand washing or alcohol- based hand solutions are recommended for transmission prevention [18]. The dramatically decline in RSV isolations during COVID-19 pandemic raises the question whether RSV prevention precautions should include not only contact but also droplet precautions.
Johnson et al. assessed in vivo the efficacy of surgical masks and N95 respirator to filter influenza virus particles in patients with laboratory confirmed acute Influenza. They found that surgical masks and respirators were equally effective in filtering influenza, and no virus particle could be detected by RT-PCR in any participant of their study [19]. In contrast, a comprehensive review of eight trials which examined effectiveness of masks in preventing transmission of respiratory viruses concluded that surgical masks did not decrease the risk for respiratory illness [20].
Indoor crowded places during rainy seasons or cooler months might facilitate transmission of viruses. Furthermore, bronchiolitis is believed to spread in nurseries and schools. As an example, avoidance of large crowds in day-care settings may decrease the risk of RSV infection. We assume school and nurseries’ closure due to the COVID-19 pandemic have had a significant, maybe greater impact on the transmission of other viruses in addition to its impact on SARS-CoV-2 itself.
A Brazilian study described the impact of social isolation due to COVID-19 pandemic on the seasonal incidence of respiratory illnesses. They found an average monthly reduction of 38 hospitalizations with a diagnosis of respiratory diseases in the period of social isolation [21].
Even though most pediatric respiratory illnesses occur among children before the age of five years, children in this age group present behavioral and technical challenges in wearing face masks correctly, and for prolonged yet necessary periods of time. Thus, other factors mentioned before, such as lock downs, social distancing and closures of kindergartens, schools and airports were probably more pivotal to the decline in respiratory diseases. Another possible reason for this decrease could be the herd effect of masks worn by adults, older siblings and close contacts, which are assumed to be more cooperative and persistent in their mask wearing and social distancing.
An interesting question is how these epidemiological factors influenced bacterial pneumonias. There is emerging evidence indicating that viral and bacterial infections act synergistically in many cases, and increase the severity of community acquired pneumonia [22]. Influenza virus for example, using several mechanisms such as destruction of respiratory epithelium, decreased muco-ciliary velocity and transient immunosuppression can set the stage for secondary bacterial infections [23, 24, 25]. Thus, the decline in viral infections mitigates the reduction in both bacterial pneumonias, and in viral and bacterial co-infection cases observed during the 2020-2021 season.
Several other intriguing observations arise, including the relative increase in upper versus lower tract infections during 2020-2021 compared to 2018-2019, but without an increase compared to 2019-2020 (Figure 3). This can be explained by the fact that while respiratory infections were scarcer during the 2020-2021 season, there was a relative persistence of viruses typically causing more upper respiratory symptoms such as parainfluenza and rhinovirus. The question why these viruses “prevailed” and influenza and RSV did not, is a fascinating one. The relative high prevalence of rhinovirus during COVID-19 portrayed in our study was also described by Poole, et al. [26]. One possible explanation is that rhinoviruses are non-enveloped, making them moderately resistant to soaps and sanitizers and more stable on surfaces, thus allowing greater transmission between children. Additionally, there is greater asymptomatic transmission of rhinoviruses, which would allow them to circulate more freely [27]. Wu, et al. showed that previous rhinovirus infection suppresses subsequent influenza infection. Possible mechanisms for this phenomenon include direct blockade of viral entry receptors for one virus by another virus, viral competition for host cell resources, and viral induction of innate or adaptive immune responses that protect against a related or distinct virus [28]. This raises the question whether COVID-19 by itself or with “the help” of rhinoviruses, via viral interference, could mitigate the dramatic decrease in other viral infections generally, and influenza virus specifically.
The main limitation of the study is its retrospective nature. It describes the respiratory illnesses in only one center in a hospital setting and does not necessarily represent the situation in community clinics. Nevertheless, as the largest pediatric center in Israel, we assume our results are very much a reflection of hospitalizations in other medical centers as well. The Israeli center of disease control (ICDC) reports every week about the respiratory viral isolations. As to the week ended January 30th, 2021, no influenza activity has been identified in the community, and the downward trend of influenza-like illness were low [29].
Conclusion
During the COVID-19 pandemic there was a dramatic decline in hospital admissions due to pediatric respiratory illnesses, as reflected by only one isolation of RSV and no isolation of influenza during a period of four months. We observed a concomitant significant decrease in the prevalence of HMPV, parainfluenza and adenovirus infections, with an increase in the prevalence of rhinovirus isolations. These findings may be explained by various epidemiological factors such as social distancing, recurrent lock downs, facemask wearing as well as viral interference.
References
-
Izurieta HS, Thompson WW, Kramarz P, Shay DK, Davis RL, et al. (2000) Influenza and the rates of hospitalization for respiratory disease among infants and young children. N Engl J Med 342(4): 232-239.
-
Iwane MK, Edwards KM, Szilagyi PG, Walker FJ, Griffin MR, et al. (2004) Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics 113(6): 1758-1764.
-
Pacheco PO, Justicia Grande AJ, Calle IR, Tenreiro CR, Sly P, et al. (2018) Respiratory Syncytial Virus Seasonality: A Global Overview. J Infect Dis 217(9): 1356-1364.
-
Fraaij PL, Heikkinen T (2011) Seasonal influenza: the burden of disease in children. Vaccine 29(43): 7524- 7528.
-
Muscatello DJ (2019) Redefining influenza seasonality at a global scale and aligning it to the influenza vaccine manufacturing cycle: A descriptive time series analysis. J Infect 78(2): 140-149.
-
Coronavirus disease (COVID-2019) situation reports. World Health Organization.
-
Jones N (2020) How COVID-19 is changing the cold and flu season. Nature 588(7838): 388-390.
-
Yeoh DK, Foley DA, Minney Smith CA, Martin AC, Mace AO, et al. (2020) The impact of COVID-19 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin Infect Dis 72(12): 2199-2202.
-
Brusselen DV, Troeyer KD, Haar ET, Auwera AV, Poschet K, et al. (2021) Bronchiolitis in COVID-19 times: a nearly absent disease?. Eur J Pediatr 180(6): 1969-1973.
-
Wald ER, Guerra N, Byers C (1991) Upper respiratory tract infections in young children: duration of and frequency of complications. Pediatrics 87(2): 129-133.
-
Kesson AM (2007) Respiratory virus infections. Pediatric Respir Rev 8(3): 240-248.
-
Atkinson M, Lakhanpaul M, Smyth A, Vyas H, Weston V, et al. (2007) Comparison of oral amoxicillin and intravenous benzyl penicillin for community acquired pneumonia in children (PIVOT trial): a multicentre pragmatic randomised controlled equivalence trial. Thorax 62(12): 1102-1106.
-
Meissner HC (2016) Viral Bronchiolitis in Children. N Engl J Med 374(1): 62-72.
-
Papadopoulos NG, Megremis S, Kitsioulis NA, Vangelatou O, West P, et al. (2017) Promising approaches for the treatment and prevention of viral respiratory illnesses. J Allergy Clin Immunol 140(4): 921-932.
-
MacIntyre CR, Chughtai AA (2015) Facemasks for the prevention of infection in healthcare and community settings. BMJ 350: 694.
-
Siegel JD, Rhinehart E, Jackson M, Chiarello L (2007) 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am J Infect Control 35(10): 65-164.
-
(2021) Considerations for Wearing Masks- Help Slow the Spread of COVID-19. CDC.
-
Smith DK, Seales S, Budzik C (2017) Respiratory Syncytial Virus Bronchiolitis in Children. Am Fam Physician 95(2): 94-99.
-
Johnson DF, Druce JD, Birch C, Grayson ML (2009) A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis 49(2): 275-277.
-
Chou R, Dana T, Jungbauer R, Weeks C, McDonagh MS (2020) Masks for Prevention of Respiratory Virus Infections, Including SARS-CoV-2, in Health Care and Community Settings: A Living Rapid Review. Ann Intern Med 173(7): 542-555.
-
Nascimento MS, Baggio DM, Fascina LP, do Prado C (2020) Impact of social isolation due to COVID-19 on the seasonality of pediatric respiratory diseases. PLoS One 15(12): 0243694.
-
Yun KW, Wallihan R, Juergensen A, Mejias A, Ramilo O (2019) Community-Acquired Pneumonia in Children: Myths and Facts. Am J Perinatol 36(02): 54-57.
-
Cawcutt KA, Kalil AC (2017) Viral and bacterial co- infection in pneumonia: do we know enough to improve clinical care?. Crit Care 21(1): 19.
-
Metersky ML, Masterton RG, Lode H, File TM, Babinchak T (2012) Epidemiology, microbiology, and treatment considerations for bacterial pneumonia complicating influenza. Int J Infect Dis 16(5): 321-331.
-
Pittet LA, Stoodley LH, Rutkowski MR, Harmsen AG (2010) Influenza virus infection decreases tracheal mucociliary velocity and clearance of Streptococcus pneumoniae. Am J Respir Cell Mol Biol 42(4): 450-460.
-
Poole S, Brendish NJ, Tanner AR, Clark TW (2020) Physical distancing in schools for SARS-CoV-2 and the resurgence of rhinovirus. Lancet Respir Med 8(12): 92- 93.
-
Vandini S, Biagi C, Fischer M, Lanari M (2019) Impact of Rhinovirus Infections in Children. Viruses 11(6): 521.
-
Wu A, Mihaylova VT, Landry ML, Foxman EF (2020) Interference between rhinovirus and influenza A virus: a clinical data analysis and experimental infection study. Lancet Microbe 1(6): 254-262.
-
(2021) Respiratory viruses in Israel Surveillance Report, Week 4. Israel Center for Disease Control.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria