Covid-19 Vaccination Advantages of Opting for an Active Pharmacovigilance Model
Background: To measure vaccination`s risks it exists the term “events supposedly attributed to vaccination or immunization” (ESAVI). ESAVI monitoring usually consist in passive surveillance based on voluntary notifications done either by beneficiaries or by health professionals. The spontaneous reports are scarce compared with active surveillance. Unfortunately; active methods performed by health service are expensive, laborious and unfeasible due to the few health personnel available. Objective: to evaluate the efficacy of an active method for ESAVI reports associated to COVID19- vaccines performed by university students. Methods: a research comparing two Pharmacovigilance methods for COVID-19-ESAVI was performed (passive vs active surveillance with participation of university students) from May to September 2021. Results: At the end of the study period, in Argentina 52.786.324 anti-COVID-19 vaccines were applied (1st dose 56, 86%; 2nd dose 43, 14%), and 102.358 ESAVIs were validated (1st dose 74, 75%; 2nd dose 23, 96%; other dose 0, 5%; No data 1, 24); 2, 16% among them were considered severe. Although female/male vaccination/ratio was similar (50.31% vs 49.67%), ESAVI were much more reported by females (72.8%). The active pharmacovigilance experience was performed by 933 studentsvolunteers. They contacted 56,824 vaccinated people; obtaining 39,952 “positive” calls (either “no events” or “potential ESAVI” results). The monthly contacts performed by students were 14,206±1124; among them, 1186±436 calls were “refused”, while in 3,032±741 cases existed wrong phone number. From 6.652 potential ESAVI reported; 1,037 were validated, which means 1.82% of vaccinated people contacted, certainly a better result than the 0.121%obtained by passive reports (p <0.0001). Conclusion: An active method of pharmacovigilance performed by health students was able to increase 15 times the validated ESAVI reports after COVID-19 vaccination.
Introduction
Medicines are essential keys to prevent and modulate the natural history of numerous diseases, and due to their use, a notable increase in life expectancy has been achieved at the population level during the last century. However, drugs are not free to generate harmful and unintended responses even in therapeutic doses, event called Adverse Drug Reactions (ADRs), which are recognized as a frequent clinical problem, an important cause of morbidity or mortality and of great negative impact on public health [1]. For this reason, at the same time that drugs are been registered, there are particular efforts to report their unwanted actions, following the WHO recommendation for constant monitoring of all drugs traded in a modality called “pharmacovigilance”. Pharmacovigilance (PV) is then a process that encompasses the monitoring, research, collection, analysis and evaluation of information provided by patients and health professionals on adverse effects related to health technology (drugs, vaccines, medical devices, etc.). These PV studies, also called post-marketing or phase IV studies, constitute the recommended methods to determinate the quality and safety of the drugs once they are already in the market [2].
Pharmacovigilance Methods
There are several methods for the development of pharmacovigilance activities. The ideal method does not exist, since it is nearly impossible to monitor the entire population and assess the different medications that each individual regularly takes (Table 1).
| Classic Methods | Type of Report |
|---|---|
| Pasives | - Spontaneous or anecdotal notification |
| - Voluntary notification (yellow card) | |
| Epidemio logical | - “Case-control” studies |
| - “Cohort” studies | |
| - Vital or morbidity, mortality and birth statistics. | |
| - Cross-sectional studies | |
| Intensive | -Intensive monitoring of hospitalized patients. |
| -Diagnosis of ADR from the hospital diagnosis. |
Table 1: Methods of Pharmacovigilance.
The classic spontaneous or voluntary notification methods are techniques in which the researcher (usually, members of the health care team) does not control the variables, but simply remains attentive on the use of drugs and the consequences of their use. The weaknesses of this method is that its depend on the willingness of the person to report, that it has little sensitivity, its monitoring is difficult, and it is generally associated with low quality of information and false alarms. Epidemiological methods are designed to determine the adverse reactions of drugs before or after their commercialization, and are generally carried out in a limited group of individuals.
Intensive methods are used in health institutions where data collection performed in a systematic way is available and where adverse effects of drugs can be collected without major problems. Unfortunately, because a great number of staff members are needed to develop a follow up of drug utilization at population levels, these active methods are usually unviable for the majority of the health systems.
Pharmacovigilance of Vaccines
Vaccines are drugs with certain characteristics that make them special for the specific protection against certain diseases. Immunizations are on the top among the most successful and cost-effective public health interventions of all time. As important as the benefit that vaccines provide, is to guarantee their safety, considering that these drugs, like any other medicines, can generate adverse events and that they are used by a large number of healthy people. The definition of Vaccine Pharmacovigilance (VPV) was generated in 2012 by the Council for International Organizations of Medical Sciences (CIOMS) [3], being defined as the “detection, evaluation, understanding and communication of adverse events that occur after immunization or problems related to immunization”.
These “Adverse Events Following Immunization” are defined as side event that occurs long after immunization and does not necessarily have a causal relationship with the use of the vaccine. The adverse event can be any unfavourable or unwanted sign, abnormal laboratory finding, symptom or disease. All of these signs or symptoms are called by different ways: Adverse Events following immunization (AEFIs), Vaccine Adverse Event Reporting System (VAERS); etc. For this same concept in the Americas region [4] the term “Event Supposedly Attributed to Vaccination or Immunization” (ESAVI) has been coined, and since the present research was performed in Latin-America, this will be the acronym use along this paper.
As any other drug, one of the most used systems in ESAVI monitoring is passive surveillance, which consists on the voluntary notification of these events, whose main utility is the detection of potential safety signals of a particular vaccine; allowing the identification of new risks, new information on little- documented risks, being easily accessible at a low-cost. The World Health Organization
(WHO) and the Pan American Health Organization (PAHO) have generated tools to support the implementation of pharmacovigilance systems both at the regional level and in the different countries of each region. One of these tools is an indicator that is used in passive surveillance to establish whether a vaccine reaches a minimum of safety. According to this indicator, if a country has a reporting rate of at least 10 ESAVI per 100,000 vaccinated (0.01%), it is considered that it has reached the minimum capacity threshold regarding vaccine safety [5].
In general, the regulatory authorities of each country are in charge of collecting the information from the ESAVI, and subsequently notifying it to the Uppsala Monitoring Center (UMC), which is a WHO Collaborating Center in Pharmacovigilance where VigiBase was installed. This base is the only database recognized by WHO Global Safety Notifications for Individual Cases. Each country enters its reports in their Vigi Flow system, validates them and connects their information with VigiBase for global consolidation [6]. From these data, it is possible to know the different expected events of each vaccine and collaborate in making decisions about the best immunization options In many Societies, it that not exist a “culture” of self-report. This problem should be added to the wrong feeling that health professionals have, believing that if they report an adverse event of the prescriptions they made, these data can harm them. Unfortunately, passive notification methods performed by patients and doctors achieve poor results with very few records in relation to the number of vaccines administered [7]. In order to evaluate the efficacy of an alternative surveillance method for ESAVI related to COVID-19 vaccines, the present study was started.
Materials and Methods
Type of study
Cohort observational study that compared two methods of pharmacovigilance of ESAVI data recruitment.
Period of Study
From 2nd of January to September 30th2021 (occasionally interrupted due to student`s vacations in July).
Groups of Study and Methodology
Two methods of pharmacovigilance of events related to COVID-19 vaccination were applied to people that received any kind of vaccine against SARCoV-2 virus in Argentina. One of these methods was based on the classical passive ESAVI reports (with occasionally active calls to certain patients), and the other method was based on a process of active routine calls to patients that received COVID-19 vaccination 3 or 4 weeks after their immunization, with a protocol of contact in order to explore data related to ESAVI (table 2).Due to the limited number of staff, it is usually difficult to opt for active pharmacovigilance by contacting each vaccinated person. To mitigate this limitation, the Ministry of Health of the Province of Buenos Aires made a collaboration agreement with the Chair of Pharmacology of the Faculty of Medical Sciences National University of La Plata, so that 1.000 advanced students were trained to carry out active surveillance either by telephone or social networks, in relation to the ESAVI detected during the study period. The number of ESAVI obtained in each state/district was compared with the number of the applied vaccines. This ratio was used has a measure of efficacy obtained by each method.
Students Training Process
All 1.000 students were separated in sub-groups of ten members in order to received training. The training process included how the conversation should be started; what questions should be asked and how to managed negative response or special situations. After the training, the students were assigned to one of the twelve regions that Buenos Aires State is divided. Each Region had several coordinators that monitored the calls and provided back up for special situations that might appeared.
ESAVI
For the present study, only the validate ESAVIs were taking into account. The validation was performed by the National Committee of Vaccination Security, depending on the National Ministry of Health in Argentina. This Committee studied each one of the notifications and confirmed it truthfulness (in severe ESAVIs the patients/families were always contacted). After the confirmation, this data was uploading to the international databases (VigiBase).
Vaccination
To determine the amount and type of vaccines applied in the study period in each province, the public database of open data of the Ministry of Health of the Nation (NOMIVAC) was used (available at:http://datos.salud.gob. ar/dataset/vacunas-contra-covid19-dosis-aplicadas-en-la- republica argentina/archivo/e4515c25-e1fd-4f02-b1c1- 5453c36eada6)
Data Management
All data obtained from calls was registered in a database especially developed for this project, based in the National
Formulary of ESAVI registration. In order to obtain much purer data, reports of patients residing in another district that vaccination or notification was carried out, were excluded from the analysis.
Data Analysis
Results obtained from the active surveillance experience performed by Buenos Aires State together with the National University of La Plata, were uploaded to database and then compared with the information extracted from other states of the country during the period of study. “R” software was used for the data analysis.
Results
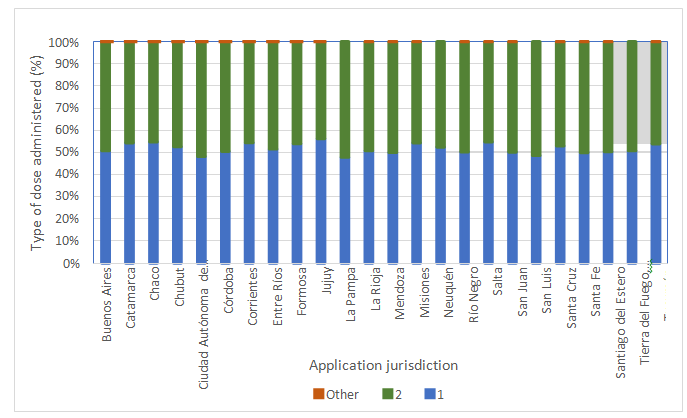
At the end of the study period, 52, 786, 324 anti- COVID-19 vaccines were applied in Argentina (of which 20,
166, 920 vaccines were applied in the state of Buenos Aires, 38.33% of the total country), destined for 29.978.754 people (11.498.789 from the state of Buenos Aires). After screening and exclusion of the failed reports, 102.358 ESAVIs were confirmed and validated. From this universe of ESAVI 74, 75% corresponded to the first dose, 23, 96% to the second dose,0,5% to other doses, and 1,24% with no information (Figure 1). The severe cases were 2, 16% (range 0-15.67). Excluding one of the States located in patagonian region that reported 15.67% of severe cases, the range of serious events in the country were 0% to 8, 62%. In Buenos Aires State, ESAVI considered severe were 1, 68%. These data allow calculating the vaccination/ESAVI average ratio, which was 193, 91 ESAVI per 100,000 vaccinated from the total vaccines applied; 189, 33 ESAVI from 100.000 vaccines administrated in Buenos Aires State and 194, 64 ESAVI due to vaccination given in the rest of the country.
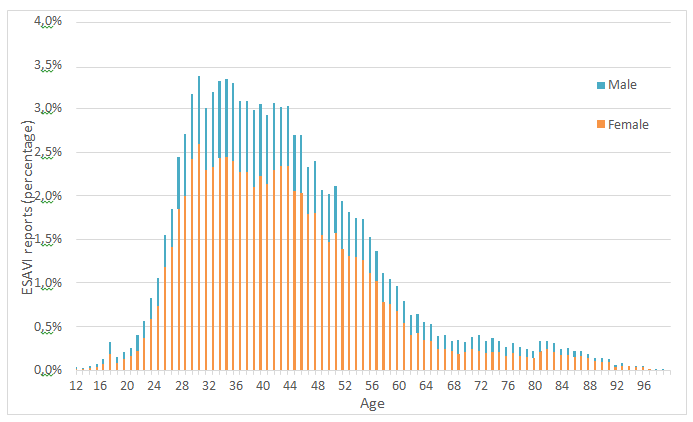
Although female/male ratio was similar in terms of vaccination (50.31% vs 49.67%), ESAVI were much more reported by females (72.8%) than males (27.2%) (Figure 2). The age plot shows a distribution skewed to the left. The average age of those who reported an ESAVI was 43 years old (SD=14, 05).50% of cases are in an age range between 32 (Q1) and 50 (Q3) years. In the case of women the average age is 42 (SD=13, 67), while among men is 44 (SD=15, 03).
Concerning to the number of vaccines administrated in each district and the percentage of ESAVI detected in relation to those vaccines, it can be said that there was a direct correlation between both parameters. (Table 2).
| VA in Argentina (n) | ESAVI Argentina (n) | ESAVI Argentina (%) | VA in Arg. without BA (n) | ESAVI Arg. without BA (n) | ESAVI Arg. without BA (n) | VA in BA (n) | ESAVI in BA (n) | ESAVI in BA (%) | VA in Study (n) | ESAVI in Study (n) | ESAVI Study (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 4,43,85,727 | 53,814 | 0.12 | 2,73,72,477 | 37,234 | 0.13 | 1,70,13,250 | 16,580 | 0.1 | 56,824 | 1,037 | 1.82 |
Table 2: Level of vaccination and ESAVI reported in each district.
VA: vaccines applied; ESAVI: Event supposedly attributed to vaccination or immunization; BA: Buenos Aires State; Arg.: Argentina Table 2: Level of vaccination and ESAVI reported in each district.
Concerning the study group, the results obtained shows that one thousand students were initially enrolled in the project. From them, 933 (93.3%) were still active by the end of the research. A total number of 56,824 calls were performed during the period, with an average of 14,206±1,124personal contacts with vaccinated persons per month (excepted for the period July 15th-August15th where the calls were interrupted due to student`s vacations).Of these monthly calls, 1,186±436 of the people refused to answer the questions from ESAVI formulary while 3,032±741 lack of response or had wrong number. That means that the positive contacts of the vaccinated people during the period were 39,952 (either stating that they had no events or confirming the existence of a potential event).
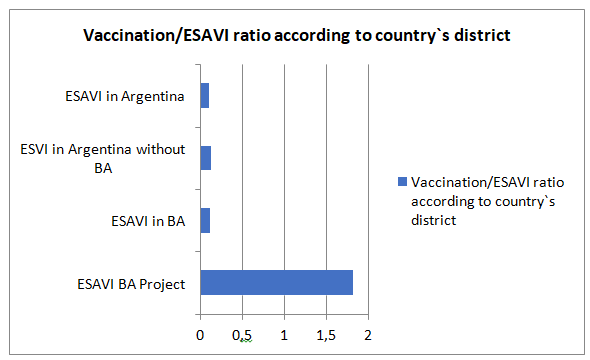
Noteworthy, if we just consider the 56,824 people vaccinated and contacted by the students during the study period, it could be established an overall number of 6,652 potential ESAVI reported. From them, 1,037 ESAVI were finally validated by the National Committee of Vaccination Security which means 1.82% of the total amount of people contacted after vaccination. From these events, only 38 (3.66%) were categorized as “severe” or “serious” while the other 999 were considered “non-serious”. Although there is no significant difference between the vaccine/ESAVI ratio obtained in Argentina versus the data obtained in Buenos Aires State when classic method was applied (0.121 vs 0.104% p 0.7), certainly, it was detected significant differences between vaccination/ESAVI ratio extracted from overall reports in Argentina vs. this same ratio obtained by the active method of reports extracted from our research. The ratio of “vaccines administrated/ESAVI reported” obtained from the active method of pharmacovigilance, highly increased the rate of notifications (1.82 vs 0.121 p < 0, 0001) (Figure 3).
Discussion
Pharmacovigilance has four major stages: detection, deduction, decision, communication/dissemination. However, “detection” is a key point, since it is the beginning of the process and the others steps will depend on this stage. Without detection it is not possible to develop the other phases. Most commonly detection stage employs observational/ pharmacoepidemiological methods like spontaneous reports, case series, cohort studies or case– control studies; which mean that either patient’s self- report or health professional reports are needed. However, these spontaneous reporting depends on country`s culture. Unfortunately, Latin-American countries do not in the habit of self-reporting. This low ratio of reports is due for many reasons, some of them are associated with people`s lack of time, lack of will and commitment, fear of being identified or due to the population discredit in their own health authorities and in how they can use the information properly [8]. On the other hand, health professional culture of reporting is low mainly due to the belief that it exist a potential risk in being personally involved with the ESAVI reported [9].
The present study was performed considering the amount of vaccines applied in the country; hence, the type of vaccine administrated was not analyze. This is because initially, when the study started, all vaccines applied were Sputnik V, but also because the focus was on ESAVI’s reporting methodology and not on the events themselves. However, a second study is now in process, concerning ESAVI according to the types of vaccines approved and used in the country: Astra Zeneca ChAdOx1 nCoV-19 vaccine -AZD1222- ; CovishieldChAdOx1 n CoV-19; Sputnik V; Moderna; Pfizer- BionTech; Sinopham; Cansino - Ad5-nCoV. Concerning this topic, it should also be noticed that Local Public Health authorities designated certain vaccines to a special population (i.e. Sputnik in elderly, Sinopham in children, Moderna in immunodeficient population; etc). This element might bias the results obtained, therefore the special study which is now taking place will be able to show the difference level of ESAVI according to the vaccine applied. When the classical form of reporting is considered, we can observe that in Argentina there is a lower rate of ESAVI reports compared to international data [10, 11, 12]. However, it should be noticed that the ESAVIs extracted from public database and then included in our study were already analysed, passed through a screening process, and then confirmed its validation by infectious experts; an aspect that must be considered as a distinctive aspect with respect to other publications. However, the comparison between the regular reports obtained by classical pharmacovigilance system in Argentina, versus the active model used in this research, showed statistical significant differences. The active call (system that contacts people and it does not expect for an spontaneous report) and personalized contact made to each vaccinated after a period of 3 to 4 weeks after receiving the vaccine, allows a net reminder of the events suffered, and a greater reporting rate, increasing the ESAVI rate by more than 15 times in relation to classic reports.
This type of active pharmacovigilance method is usually unfeasible for health authorities, either from a managing or economic point of view, since it will usually need a large staff, aspect the health systems usually do not have. However, in this experience, health sciences students were invited to participate, receiving training in exchange for their homework. This academic institutions/health authority relationship is symbiotic, since some of them obtain training and experience that will be useful for professional life; while the health system not only enhance its active pharmacovigilance system, but also is changing the culture of ESAVI reporting among future health professionals.
Conclusion
An active pharmacovigilance experience performed by the Staff of Ministry of Health with the help of university students from Health Careers was able to increase in 15 times the validated ESAVI reports after COVID-19 vaccination. This symbiotic interaction between Health and Educational public sectors helps to reduce the economic impact that usually have the active pharmacovigilance methods, and transforms it, in a viable option available to be adopt by other country`s authorities.
Conflicts of Interest
Authors declare no conflict of interest.
Acknowledgements
We acknowledge the support of GIS collaborative.
Funding
This manuscript was generated by the GIS collaborative, which has been supported by National University of La Plata and Ministry of Health of Buenos Aires, Argentina.
Interdisciplinary Health Group (GIS)
Coordinators: Ahumada G, Alnajjar H, Andreaccho S, Avalos T, Asurmendi A, Avellaneda JS; Azula C, Cerletti E, Conti A, Coppola M, Covacich MJ, de Caria G, Dragani C, Fernandez A, Fernandez M, Flessatti J , González L, Guillen T, Herrera G, Liso M, McAdden C, Montefusco F, Pareta L, Peñaloza M; Romero J, Russo C, Suarez A, Toyos J. Volunteers: Abait I.; Abraham Y.; Acosta SM.; Actis Caporale R.; Acuña M.; Adradas G. ; Albarrán A, Agnoli B; Aguado SB.; Agudo S.; Aguilera Churca A.; Aguirre Bengoa P.; Aires Granado C; Aizcorbe A.; Alarcón N.; Albacete A.; Albanese SV; Albarracin C.; Albino Huaman C.; Alcazar F.; Alcoba Espejo F.; Alcoser F.; Alderete R.; Ale V.; Alfonso L.; Almarás J.; Almeida C.; Alonso Andragnez A.; Alonso Citón L.; Alonso SA; Altuna M.; Alvarez H.; Alvarez I.; Alvarez S.; Alza Oppenheimer C.; Alzogaray MC.; Alzuet J.; Amieva A.; Andrade Colque G.; Andrade C.; Andrés L.; Andrieu V.; Angeli Barnetche C., Anselmino C.; Antonelli A.; Antonio Camatari J.; Anto- niuk L.; Antunez T.; Anze Quispe L.; Aragón Herrera N.; Arana F.; Arana J.; Araujo D.; Argañaraz K.; Argoti N.; Arizcuren P.; Arocena M.; Arrazola M.; Arrua S.; Arrufat MS.; Asprea Sarin J.; Astuti V.; Atoche Dominguez Z.; Aucachi G.; Ausili MB.; Avellaneda Gigena I.; Aversa C.; Avetta S.; Avila Sobrecasas JB.; Azcoiti Tomellini J.; Aznarán A.; Badano E.; Baier C.; Balatti V.; Balbin Fernandez A.; Baldoni A.; Baliño M.; Ballerino E.; Ballesteros L.; Barbosa Ferreira M.; Barragán I.; Barraza D.; Barrera K.; Barrientos C.; Barrion- uevo C.; Barrios J.; Barrios S.; Barros Flores Y.; Barth Soria S.; Barucco V.; Basal C.; Basanta C.; Bastone E.; Bazán F.; Bedon Cobeñas I.; Beguerie M. ; Bejger L. ; Bellavita MV. ; Bellido J.; Belvedere M. ; Benitez Y. ; Berdini M. ; Berenguer L. ; Bergna PI.; Bermejo Guerrero AP.; Bernaola L.; Berto C.; Bertolotti C.; Bessone V.; Bianchet J. ; Bianchi M. ; Billinger Macchiaroli S. ; Biloni ML. ; Bin Espósito AS.; Binaci A.; Biondi B.; Blanco C.; Blanco F.; Blasco M.; Blasetti I.; Bobadilla L.; Bonavita K.; Bonino IM.; Bordalecu Cam- podónico S.; Borgonovo A.; Borjes Gimenez S.; Boschetti AS.; Bovati F. ; Branca G.; Bravo Escobar V.; Bravo KA. ; Brime M.; Britez V.; Broquelaire M.; Bruno Anabella G.; Bruno I.; Bruzual M.; Bugatti JI.; Bulus M.; Burgos A.; Burguez Soca M.; Burrieza M.; Busso P.; Bustamante M.; Bustince M.; Caballé J.; Caballieri MP.; Cabero ME.; Cabezudo Witteveen MF.; Cabral Da Silva B.; Cabral V.; Ca- brera C.; Caceres FN.; Cáceres MD.; Cailotto A.; Calfin Aguirre G.; Calvis MA.; Calvo V.; Camilletti F.; Campillo T.; Campos P.; Campos DA.; Cancio JC.; Canzani MC.; Caplán E.; Capobianco N.; Capolongo MJ.; Caporale A; Capurro FL.; Caputo MA.; Caracino F.; Carballo PA.; Cardoza Ojeda A.; Cardozo Casariego C.; Carestia J.; Carestia M.; Cari Cubilla F.; Carlini M. ; Carrara I.; Carrasco CJ.; Carreras T.; Carriere MM.; Casais C.; Casal EI.; Casas MDC.; Cascini L.;Casella V.; Castagnari MS. ; Castagnetto L. ; Castellani CI.; Castelló G.; Castillo Conesa MC.; Castillo C.; Castillo GT.; Castro Alzueta V., Castro B., Castronuovo L.; Castrosin S.; Catalan T.; Caviglia L.; Cays- sials C.; Cea J.; Cedergren L.; Cepero JC.; Cercato FJ.; Cersosimo O.; Cervantes W.; Cesaretti Di Battista K.; Chaparro J.; Chechele S.; Ciancia D.; Ciancio F.; Cingolani C.; Cini N.; Cisneros M.; Clariana Ruiz O.; Cochet M.; Cohen Salama M.; Colavitte M.; Collazo A.; Colmenares JI.; Colonio Diaz A.; Colonna C.; Contarino L.; Conte J.; Conte Joscelyn T.; Coria Candela A.; Coriggiano A.; Cornicello JB.; Correa M.; Cortes N.; Cosenzo MJ.; Cosmic L.; Costanzo F.; Cot Martina A.; Crespo Escudero Whu A.; Crespo L.; Crespo SB.; Crocci CA.; Crubellati A.; Cuello T.; Cuervo CA.; Cuevas FA.; Cuyeu Telese Z.; Da Silva BP.; Dabadie Zinetti G; Dagand C; Dall’Orso R; Daroda P; Daza Brisa P; De La Cruz MdP; De La Fuente I; De Los Santos C; De Michelis P; Delucchi G; Denisienia MV; Derkacz VN; Dettler G; Di Girolamo M; Di Pietro D; Diaz Flores V; Diaz MA ; Díaz M; Díaz SA; Diaz V; Dini S; Disanti T; Dittlar C; Divitto L; Donoso Vidal B; Draghi J; Drews J; Duarte Talavera D; Dulbecco J; Dumón M; Dupuy L; Durante E; Echarren A; Echeverría C; Ech- everria MA; Eiros M; Elosegui E; Elpuerto C; Encalada HR; Encinas Ojeda J; Ercoli MS; Errecalde AC; Esayan MB; Escamez P; Es- cudero I; Eseiza JC; Espelet U; EspineL JF; Esteban N; Estefanía S; Etchegoyen V; Evangelista G; Eymeri J; Faga ML; Failchijes I;
10. Beatty AL, Peyser ND, Butcher XE, Cocohoba JM, Lin F, et al. (2021) Analysis of COVID-19 Vaccine Type and Adverse Effects Following Vaccination. JAMA Netw Open 4(12): e2140364.
11. Jeon M, Kim J, Oh CE, Lee JY (2021) Adverse Events Following Immunization Associated with Coronavirus Disease 2019 Vaccination Reported in the Mobile Vaccine Adverse Events Reporting System. J Korean Med Sci 36(17): e114.
12. Wu Q, Dudley MZ, Chen X, Bai X, Dong K, et al. (2021) Evaluation of the safety profile of COVID-19 vaccines: a rapid review. BMC Med 19(1): 173.
Fajre L; Farías Nanni P; Favarotto O; Federico Y; Fermoselle Zanetta A; Fernández Ayala J; Fernández Colque B; Fernandez MA; Fernandez AN; Fernández CL; Fernández I; Fernandez L.; Fernandez MB; Fernandez M; Fernandez YC; Ferrá F; Ferrari MG; Fer- reyra RA; Ferro R; Fiad Maria R; Figini Maria F; Figueroa C; Figueroa J; Fiorotto ML; Flores BR; Flores EG ; Forlino B; Fraietta F; Franchi MF; Franco B; Franco N; Funes V; Gabrielloni JI; Gagliarducci C; Galli J; Gamboa D; Garbuglia D; Garcia Morales D; García Orellana T; García Panizza M; Garcia Rojas M; Garcia Romero C; Garcia AA; García F; Garcia FM; García ML; Garcia ME; García SM; Garcia TJ; Garmendia P; Gasparini M; Gau L; Gauna C; Ghessi F; Ghigliotti E; Giangiobbe I; Giglio C; Gil MF; Gimenez A; Gimenez M; Giordano A; Gobato S; Godoy P; Goicoechea M; Goites C; Goldstein L; Gómez Centurión M; Gomez A; Gomez E; Gomez R; Gómez V; Gonald L; Gonzalez C; Gonzalez R; Gonzalez Todd H; Gonzalez E; Gonzalez E; Gonzalez M; Gonzalez MA; Gonzalez M; Gonzalez S; Goñi F; Gordon C; Goyenola GA; Gracia J; Grado D; Graef C; Greco J; Grillo D; Gronda A; Guaita C; Guaragnini L; Guerreiro Mar- tins M; Guevara Franco M; Guiglioni A; Guimarães Nascimento MA; Gutierrez Lea E P; Hadweh Cedeño F; Harismendi R; Harrand I; Harsanyi MJ; Hernández M; Hernández S; Herrera C; Herrera C; Herzfeld F; Hevia C; Hildebrandt C; Hiriart N; Hollmann M; Hourqueby T; Hoyos V; Huck F; Iannitto V; Ibañez Pongo C; Ibarra Mariana A; Iglesias D; Iglesias L; Ilari G; Inostroza Valdés G; Iriarte Bazzaro A; Iuorno G; Iurescia F; Jaime LA; Jalenga L; Jara IbañeZ R; Jensen S; Jorge Salazar Juarez López S; Kaiser R; Kama Daza A; Kautz Yanella H; Keem T; Knaupe A; Kociubinski I; Lamas A; Lamas V; Lambrecht S; Lanfranco L; Lanusse SP; Lanzavec- chia MJ; Lara TC; Larragueta V; Larrechart L; Larrosa MB; Lastra M; Lavezzo S; Lázaro L; Lazarte M; Lazcano G; Leal Oliveira C; Leal G; Leissa V; Leiva N; Lencina A; Leonardi ME; Leonardi V; Leopoldo NC; Lilli V; Linares N; Lisazo J; Lo Presti Guillén A; Lobo Santiago N; Loguercio V; Lopez Cafasso F; Lopez De Felice J; Lopez Erriest MI; Lopez Guerra MdP; Lopez Mendez Z; Lopez Feli- ciano S; Lopez Guillermo S; Lopez SM; López T; Lorente V; Losardo Brown K; Losert Vasquez A; Loza J; Lucarini V; Luciano MC; Luger MC; Mac Loughlin F; Machado Garcia N; Macías J; Madrid Sabillón K; Maggi M; Magi V; Magrassi R; Maier Gallardo M; Mal- donado Amaranta B; Mangini C; Mansilla Cabral M; Mansilla E; Marafuschi Phillips M; Marchi MC; Mardegan L; Marinangeli Be- ratz C; Marinelli MB; Marino P; Marques C; Marra V; Martin Barrenechea T; Martin M; Martinelli L; Martinez A; Martinez Artin F; Martínez Corti L; Martinez Sanchez J; Martinez AM; Martínez Al; Martinez Ar; Martinez C; Martinez F; Martinez IB; Martinez J; Martínez N; Martinez Siomara A; Martini NB; Martino JC; Massano M; Mastoy I; Mastrandrea B; Mata V; Mattar SN; Maulén F; Mauriño I; Mauto N; Mayer L; Medina Bazán V; Medina Gutierrez JJ; Medina MB; Meiriño A; Melo Souza J; Melone Y; Mendez F; Mendez G; Mendia Rodriguez MJ; Menéndez L; Mercuri R; Merlo MP; Merlotti AP; Meyer S; Meza MA; Meza R; Miguel F; Milone JP; Miñola M; Miquel T; Miranda C; Mixcan Purizaca K; Molina Vanegas A; Molina M; Mondino L; Montangie S; Montani Bistué MI; Montañez E; Montefusco R; Montero Perez L; Montes MA; Montiel J; Morales Caceres A; Morales C; Morales MA; Morano T; Mor- celle Gullo P; Moreira Nunes F; Moreno L; Moreno MJ; Morero A; Mossetto F; Mostafá E; Moureu A; Moyano Furiasse L; Mugnolo S; Mulder S; Muldon A; Muñ____oz Micaela A; Nahuelpan C; Nakayama Teles C; Nardo N; Narváez S; Negri T; Neme NM; Nic- colo Najera L; Nicolas C; Nicora, P; Nieva D; Nievas M; Niño Gomez P; Novelino B; Nuñez S; Obert K; Ochoa Deanes J; Ochoa J; Ochoa M; Ojeda RB; Ojeda T; Oliva M; Oliver N; Olivera D; Olivero J; Olivieri M; Ondarcuhu M; Ontivero R; Oporto LA; Orazi G; Orduna M; Orlandi V; Orozco Oses J; Ortega R; Ortiz Galindo F; Ortiz A; Ortiz J; Otero Isasis B; Otero J; Oviedo MR; Oxance ML; Oxandaberro F; Pachiorquevich S; Pacho S; Padelli Benassi P; Padron MS; Pagano A; Pal Masci D; Palazzesi MJ; Palazzo L; Palleres G; Palomino V; Panizo C; Panizzo Defelitto E; Parisi N; Parodi M; Pasapera Calcina YG; Pasi MG; Pasquale M; Patané L; Patrizi L; Pauleau Anibal W; Pazdera Guridi E; Pecoraro N; Pellegrini A; Peluso M; Pennini Guelfi R; Peña B; Peñaherrera Andrade C; Per- alta F; Perazzi A; Perazzo Crivaro T; Percaz De Rege A; Perdomo B; Pereira C; Pereyra MF; Perez C; Perez K; Pérez M; Pérgamo J; Pier B; Pin M; Pinilla V; Pinotti Lescano F; Piñeyro A; Ploza A; Pogonza C; Ponce de León MJ; Ponce S; Portilla D; Pozzer Pichinao Y; Prevettoni F; Puente G; Pueyo J; Pupco P; Puy L; Quincoces, M; Quiñones Barberon MA; Quispe Y; Raineri A; Ramírez Tedesco MB; Ramirez A; Raynoldi F; Raynoldi O; Regalia F; Reinoso R; Reser D; Reyes T; Ribeiro Souza L; Ricardo Chavez V; Ricon C; Rin- aldi MJ; Rios Garcia B; Ríos Miranda A; Ríos MB; Ripodas C; Rivarola F; Rivera Rocca R; Rivero Cajade ME; Robatto S; Robetto C; Rocchi N; Rodrigues De Souza J; Rodrigues Miranda Gonzaga P; Rodríguez Danas P; Rodriguez Garcia MB; Rodriguez Gini O; Ro- driguez Ocejo P; Rodriguez A; Rodriguez Be; Rodriguez BJ; Rohner F; Rojas Mistrangelo J; Rojas Ramos D; Roldan R; Roldán V; Romero Cañete C; Romero B; Romero J; Romia Oviedo A; Rosa Dominguez E; Rossi Buffarini R; Rossi Daiana Y; Ruggeri A; Rug- girello R; Ruiz Julia M; Rusconi F; Saavedra Fernandez A; Saavedra A; Sabadini Porto N; Sabalza B; Sacha N; Sacomani V; Salas G; Saldivar Agüero J; Saleh A; Salgueira J; Salgueiro F; Salles J; Salvatierra Rojas G; San Andres M; San Miguel A; Sanchez Nicolai A; Sanchez Solana A; Sande A; Santos Ortiz M; Sanz M; Sarasola M; Sarlingo E; Sarraude P; Sartirana J; Scarpinelli F; Scarpinelli JC; Scazzola F; Schell R; Schenholtz Y; Schwab M; Sciutto S; Scribano V; Seevald I; Seiguerman J; Sella L; Senta P; Sepúlveda M; Sere- marco M; Sersing Werner M; Servin Baudagna I; Sierra P; Sighel A; Signorio Rodríguez Franco MS; Silvetti F; Singano C; Sire N; Siscar C; Soares R; Sobota J; Solano Fonseca Holman Y; Sosa C; Sousa Miranda K; Souza J; Speranza G; Spiazzi A; Spinelli Carabajal L ; Spinelli M; Stancato Bossio S; Starna S; Stoeff Belkenoff MZ; Suarez R; Sullings Bances M; Sutin Freiman M; Talone F; Tambas- cio MI; Tapia Garzón N; Tapia ME; Tarazona Ortega G; Tarducci A; Telao JJ; Tellechea L; Tesouro L; Tipaina Nadir JC; Tiseyra A; Tolosa E; Torres A; Torrez L; Tosza Armitano T; Tozonotti J; Trombetti M; Tuesta Molero A; Uccelli ME; Urbina Guerrero C; Vac- caro Ch; Vaccaro L; Valderrama L; Valdez Khadijah R; Valenzuela Silva F; Vallejos A; Valluzzi V; Valverde Fernandez A; Vargas Gonzales J; Vargas Mamone A; Vasicek M; Vasquez Castro B; Vazquez Roncal JC; Vega Tonesi S; Vega D; Vega N; Vela Condori J;
Velázquez Pacheco L; Velzi A; Verbitchi V; Vercellino M; Vergniaud M; Verri V; Viamonte Millan F; Villa A; Villafañe F; Villarreal L; Vincen A; Vives P; Viviani L; Wall C; Wanderick Garcia D; Ward J; Wilkinson A; Xavier Frota Douglas D; Xavier R; Yaniz C; Zaballa L; Zamarripa B; Zambosco C; Zampini P; Zaracho JE; Zaratiegui C; Zeballos SM; Zieher M; Zoco JC; Zutas AP.
References
-
Sánchez I, Amador C, Plaza JC, Correa G, Amador R (2014) Clinical impact of an active pharmacovigilance system performed by a pharmacist on the reporting and under- reporting of adverse drug reactions. Rev Med Chile 142(8): 998-1005.
-
Betancourt LJ, Vigil JLG, Barnés CG, Santillán DH, Gutiérrez LJ (2004) Pharmacovigilance I. The beginning. Rev Méd IMSS 42(4): 327-329.
-
WHO (2021) Report of CIOMS/WHO working group on vaccine pharmacovigilance. Definitions and Applications of Terms for Vaccine Pharmacovigilance.
-
PAHO Pan American Health Organization (2007) Safe Vaccination: Training Modules, Module IV, technical and clinical aspects of the Events Supposedly Attributable to Vaccination or Immunization (ESAVI).
-
WHO (2018) Global Vaccine Action Plan. Secretariat annual report.
-
WHO (2000) Safety Monitoring Centre Safety. 2nd (Edn.), The Uppsala Monitoring Centre Sweden, pp: 30.
-
Shrestha S, Khatri J, Shakya S, Danekhu K, Khatiwada AP, et al. (2021) Adverse events related to COVID-19 vaccines: the need to strengthen pharmacovigilance monitoring systems. Drugs Ther Perspect 37(8): 376- 382.
-
Aspinall MB, Whittle J, Aspinall SL, Maher RL, Good CB (2002) Improving adverse-drug- reaction reporting in ambulatory care clinics at a Veterans Affairs hospital. Amer J Health Syst Pharm 59(9): 841-845.
-
Leghari Q, Chand S, Bushra R, Rizvi M, Khan M, et al. (2021) Exploration of Perception, Need and Barriers against Pharmacovigilance and Adverse Drug Reactions Reporting: Healthcare Professionals’ Insight. Journal of Pharmaceutical Research International 33(7): 78-86.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria