Knowledge, Perceived Risks and Factors Affecting the Utilization of Cervical Screening Services among Females in Owerri North LGA
Background: Globally, cervical cancer screening services involves procedures put in to prevent and checkmate complications in the cervix. Lack of cervical screening services can lead to cervical cancers, one of the leading causes of death in women, which begin in cells on the surface of the cervix. The objective of this study was to determine the knowledge, perceived risks and factors affecting the utilization of cervical screening services among females in Owerri North LGA. Methods: A descriptive cross sectional study was employed in this research. The multi-stage simple random sampling procedure was employed to obtain a sample size of 424 respondents and a self-administered semi structured questionnaire was used to gather data for this study. The Statistical Package for the Social Sciences (SPSS) was used in the analysis of the data gotten from the study. Results: The results of this study revealed that majority, 27.8% (118) of the women represented age groups between 25-34 and 45-49. For the level of knowledge of cervical screening services, most of the respondents 86.4% (366) demonstrated knowledge of cervical screening, while 13.6% (58) denied. The study also showed a good number of females, about 41.2% (175), agreed that it was risky to avoid uptake of cervical screening. Majority of the respondents reported demonstrated their approval to utilize cervix screening if offered a chance (85.9%), while 14.1% (60) denied based on results from level of knowledge of cervical screening. 19.3% (82) reported family/husband acceptance, 18.7% (79) said “distance to facility” as some of the factors affecting the utilization of cervical screening practice. Further results for the test of a statistically significant association between socio-demographic characteristics and level of knowledge of cervical screening services, age (p=0.010), parity (p=0.0008), level of income (p=0.0092) and level of education (p=0.0327) were associated with level of knowledge of cervical screening services. Conclusion: In conclusion, this study showed good knowledge of the perceived risks of cervical screening among the females but this did not translate to willingness to utilize screening and awareness campaigns must provide accurate information on cervical screening so that females can make informed choices was recommended by this study.
Introduction
Globally it has been revealed that cervical cancer screening services involves procedures put in to prevent and checkmate complications in the cervix [1]. Lack of cervical screening services can lead to cervical cancers which begin in cells on the surface of the cervix. As one of the leading causes of mortality among women, cervical cancer is the second most common cancer in women worldwide and the leading cause of cancer deaths among women in developing countries [1]. In addition, cervical cancer has relatively early onset, occurring primarily during reproductive ages, and is one of the 3 most common cancers among women under age 45 in most countries [2].
The mortality due to cervical cancer is high worldwide mainly because of absence of a functioning screening process and advanced stage of the disease at diagnosis (South African HPV advisory board, 2010). About 527,624 women are already diagnosed with cervical cancer and 265,672 die from the disease annually [3]. About; 87% all deaths from cervical cancer occurs in sub-Sahara African countries The age-standardized incidence rate for cervical cancer is much lower in developed countries at 5.0 per 100,000 compared to developing countries at 8.0 per 100,000 [4]. An important strategy towards the reduction of the incidence and mortality associated with cervical cancer is by increasing the screening rate of women that have not screened or those that screen infrequently [5]. Knowledge about cancer of the cervix and its screening is important in screening uptake. Women with low levels of knowledge about cervical cancer and its prevention are less likely to access screening services [6]. Female health workers have shown good knowledge of cervical cancer; however, cervical cancer screening attendance rates are still far from satisfactory in most countries [1, 4, 7, 8].
Despite its proven importance, rates of attendance for screening programs vary widely, and are considerably low [1, 9, 10, 11]. The low prevalence of early cervical cancer screening and limited access to its treatments largely attributed to differences in diagnosis and subsequent mortality from the disease among high and low income countries. For instance; the screening uptake for cervical cancer in the three developing regions was only 6%, 12%, and 8.3% in South Africa, Bhutan, and Nigeria respectively [12]. World Health Organization (2014) also opines that cervical cancer is largely a preventable disease. An important strategy towards the reduction of its burden in a developing country is by early diagnosis and management of the premalignant lesions of the disease; this would be achieved via screening of women at risk [13, 14]. Cervical cancer screening services among undergraduates in tertiary institutions is imperative and cervical cancer usually develops slowly, which means that most cases can be identified and managed when screening is performed regularly [15]. Cervical cancer knowledge is important because it is one of the most easily preventable forms of female cancers if early screening and diagnosis is made. Low awareness level about the disease and its risk factors, beliefs about the disease, poor access to preventive services, un-affordability of the service and current health service system can all affect decision to seek health care services for cervical cancer [16]. However, this research will provide findings on the knowledge, perceived risks and factors affecting the utilization of cervical screening services among females in Owerri North LGA.
Methods
Study Design and Setting
A descriptive cross sectional study was employed in this research on the knowledge, perceived risks and factors affecting the utilization of cervical screening services among females in Owerri North LGA. This study included every female adult aged 18 years and above in Owerri North LGA who gave in their consent for the study and caregivers who volunteered to provide vital information on the course of data collection relevant to the research at Owerri North LGA. The study excluded any woman at Owerri North who was attributed to be sick or admitted to the hospital, disabled or psychologically malnourished during the course of the study and any female adult aged 18 years and above whom refused to give in their consent from the study.
**Sampling Size**
The sample size was determined using the Yamene formula (1967) for sample size determination.
$$n = \frac{N}{1 + Ne^2}$$
- Where:
- $n$ is the desired sample size
- $N$ is the population size (29,711)
- $e$ is margin of error (0.05)
- Therefore,
$$n = \frac{N}{1 + Ne^2}$$
$$\frac{29,711}{1 + 29711^*(0.05)^2}$$
$$\frac{29,711}{75.2775}$$
$n = 394.686327$ ... 395
Furthermore, to account for 10% Non-Response Rate, (i.e. 90% response rate)
$n = n/expected response rate$
$$\frac{395}{0.90}$$
$n = 438.8888889$ ... 439.
i.e. the total sample size for the study would be 439.
**Sampling Technique**
A Multi stage sampling technique was adopted for this study on the knowledge, perceived risks and factors affecting the utilization of cervical screening services among females in Owerri North LGA.
- First stage: *Selection of Communities*. Three (3) Out of the Ten (10) Communities in Owerri North were selected by the researcher using simple random sampling via balloting to give every community an equal chance of selection.
- Second stage: *Selection of villages*. Two (2) villages each out of the total number of villages in the selected communities respectively would be selected via simple random sampling using balloting.
- Third stage: *Selection of Streets*, a total of Five (5) streets each in the selected Six (6) villages were selected via simple random sampling (balloting) which gave every street an equal chance of being selected.
- Fourth stage: *Selection of households*, a systematic probability sampling method was used to select each household in the selected streets which gave each household an equal chance of selection.
- Fifth stage: *Selection of Respondents*, the researcher selected female adults from each household or any one that was present at the time of study. They were selected until the minimum sample size was reached to ensure that the appropriate number respondents were obtained.
**Data Collection**
A self-administered semi structured questionnaire was used for the study on the knowledge, perceived risks and factors affecting the utilization of cervical screening services among females in Owerri North LGA. The Data tool (Questionnaire) consisted of Five (5) sections as follows:
- Section A: Consisted of information on the socio demographic Characteristics of females in Owerri North LGA.
- Section B: Consisted of questions on the level of knowledge of cervical screening services among females in Owerri North LGA.
- Section C: Consisted of Questions on the perceived risks of respondents.
- Section D: Consisted of questions to determine the level of utilization of cervical screening services among respondents.
- Section E: Consisted of questions to factors affecting the utilization of cervical screening services among respondents. The questions will be designed for easy apprehension by the respondents.
Reliability of the instrument was determined using test retest method. Copies of the questionnaire was given to females at Owerri West LGA which was outside the area of study by the researcher because this area for reliability testing shares similar characteristics with the Owerri North LGA that were used for the study. Chrombach alpha test was used to test for the reliability coefficient of the questionnaire and a reliability coefficient of 0.84 was obtained. Data was obtained the aid of Two (2) field assistants who were Hired and trained to aid the researcher in the data collection process. The purpose of the research was explained face to face to the respondents before distribution of the questionnaires to them.
**Data Analysis**
The Statistical Package for the Social Sciences (SPSS) was used in the analysis of the data gotten from the study. Results were expressed in percentages, frequencies, tables and charts (Descriptive Statistics). Chi square was used to Test the Hypothesis of the study (P=0.05).
Ethics
A letter of introduction and ethical clearance was obtained from the Department of Public Health Ethical clearance committee in Federal University of Technology Owerri (FUTO) before the research was conducted. The purpose of the research was explained to each respondent and verbal informed consent obtained from them before inclusion into the study. Also, anonymity of the respondents was assured and ensured. The confidentiality of the information they gave was also be maintained.
Results
Socio demographic Characteristics of respondents
From Table 1 below, it was posited that 27.8% (118) of the women represented age groups between 25-34 and 45-49, 19.9% (85) of the women were 35-44 years of age, 13.8% (59) were aged 50 years and above, and 10.8% (46) aged 15-24 years. 65.8% (280) of the women were of Igbo origin, 19.1% (81) reported ‘others’, 11.8% (50) Yoruba, and
3.4% (14) Hausa/Fulani. 65.1% (276) of the respondents were Christians, 21.9% (93) listed religions not included in the options but label ‘others’, 11.3% (48) Muslims and 1.8% (8) Traditional. 41.3% (175) of the women had a child, 32.2% (136) had two children, 23.5% (99) had 3 children and above, and 3.1% (13) had no children. Concerning the education level of the respondents, 37.5% (159) had attained secondary education, 27.5% (116) each for primary and informal education levels, and 7.7% (32) for women who earned tertiary education levels. Traders among the respondents totaled 34.0% (144), 28.7% (122) were students, 20.1% (85) ‘others’, 9.1% (39) identified as farmers, and 8.2% (35) civil servants. 40.7% (172) were not sure concerning monthly income satisfaction, 33.4% (142) were not satisfied, and 25.9% (110) of the women said “Yes”. 42.5% (180) of the respondents were married, 27.8% (118) single, 19.3% (82) separated, and 10.4% (44) widowed. When the women were asked about their household level of income, 21.1% (89) reported income above 100,000, 16.8% (71) between 2,000-10,000, 16.4% (69) earned from 11,000- 30,000, 15.0% (64) 1-1,000, 14.9% (63) listed ‘other’ income levels, 14.6% (62) earned figures from 61,000-100,000, and 1.3% (5) from 31,000-60,000.
| Characteristics | Frequency (n=424) | Percentage (%) |
|---|---|---|
| Age | - | - |
| 15-24 | 46 | 10.8 |
| 25-34 | 118 | 27.8 |
| 35-44 | 85 | 19.9 |
| 45-49 | 118 | 27.8 |
| 50 and Above | 59 | 13.8 |
| Total | 424 | 100 |
| Ethnicity | - | - |
| Igbo | 280 | 65.8 |
| Hausa/Fulani | 14 | 3.4 |
| Yoruba | 50 | 11.8 |
| Others | 81 | 19.1 |
| Total | 424 | 100 |
| Religion | - | - |
| Christianity | 276 | 65.1 |
| Muslim | 48 | 11.3 |
| Traditional | 8 | 1.8 |
| Others | 93 | 21.9 |
| Total | 424 | 100 |
| Number of Children (Parity) | - | - |
| 13 | 3.1 | |
| 1 | 175 | 41.3 |
| 2 | 136 | 32.2 |
| 3 and above | 99 | 23.5 |
| Total | 424 | 100 |
| Education level | - | - |
| Informal education | 116 | 27.3 |
| Primary | 116 | 27.5 |
| Secondary | 159 | 37.5 |
| Tertiary | 32 | 7.7 |
| Total | 424 | 100 |
| Occupation | - | - |
| Student | 122 | 28.7 |
| Farmer | 39 | 9.1 |
| Trader | 144 | 34.0 |
| Civil servant | 35 | 8.2 |
| Others | 85 | 20.1 |
| Total | 424 | 100 |
| Marital Status | - | - |
| Married | 180 | 42.5 |
| Single | 118 | 27.8 |
| Separated | 82 | 19.3 |
| Widowed | 44 | 10.4 |
| Total | 424 | 100 |
| Household level of Income | - | - |
| 1-1,000 | 64 | 15.0 |
| 2,000-10,000 | 71 | 16.8 |
| 11,000-30,000 | 69 | 16.4 |
| 31,000-60,000 | 5 | 1.3 |
| 61,000-100,000 | 62 | 14.6 |
| Above 100,000 | 89 | 21.1 |
| Others | 63 | 14.9 |
| Total | 424 | 100 |
Table 1: 0: Socio Demographic Characteristics of the Women.
Level of Knowledge of Cervical Screening Services among Females
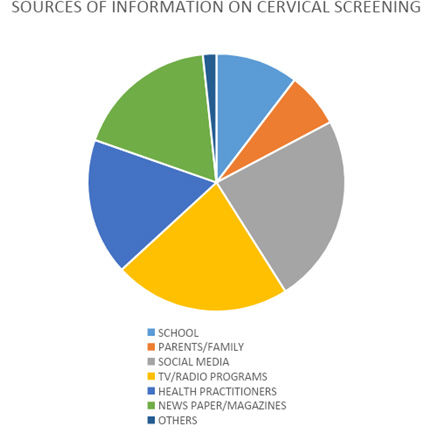
Demonstrated in Table 2 below, majority of the respondents 86.4% (366) demonstrated knowledge of cervical screening, while 13.6% (58) denied. For example, see (Figure 1) below, 23.8% (87) of the respondents reported ‘newspaper/magazines’ as their sources of information on cervical screening, 22.2% (81) said “Tv/radio programs”, 18.0% (66) reported social media, 17.2% (63) health practitioners, 6.9% (25) parents/family, 10.4% (38) school, and 1.7% (6) reported sources not listed but label ‘others’. 64.2% (272) of the respondents reported that they agree cervical screening is performed to ensure that the cervix is free from infection, while 35.8% (152) said “No”. Majority of the respondents affirmed cervical screening is diagnosed with Pap smear as well as other procedures (74.6%), while 25.4% (108) reported otherwise. When asked if digital cervix examination is an example of a cervical screening services, 65.5% (278) replied “Yes”, while 34.5% (146) reported ‘no’. Concerning cervical screening is performed among women mostly in developing countries, 62.3% (264) thought affirmative, while 37.7% (160) said “No”. The responses from the females in Owerri-west LGA concerning if cervical screening procedures if not adopted can cause possible onset of problems, 67.5% (286) replied “yes”, while 32.5% (138) reported “No”.
| Frequency (n=424) | Percentage (%) | |
|---|---|---|
| Have you heard about cervical screening? | ||
| Yes | 366 | 86.4 |
| No | 58 | 13.6 |
| Total | 424 | 100 |
| What is your source of information? | ||
| School | 38 | 10.4 |
| Parents/Family | 25 | 6.9 |
| Social Media | 87 | 23.8 |
| TV/Radio programs | 81 | 22.2 |
| Health Practitioners | 63 | 17.2 |
| Newspaper/Magazines | 66 | 18.0 |
| Others | 6 | 1.7 |
| Total | 366 | 100 |
| Cervical screening is performed to ensure that the cervix is free from infection | ||
| Yes | 272 | 64.2 |
| No | 152 | 35.8 |
| Total | 424 | 100 |
| Cervical screening is diagnosed with Pap smear as well as other procedures | ||
| Yes | 316 | 74.6 |
| No | 108 | 25.4 |
| Total | 424 | 100 |
| Digital cervix examination is an example of a cervical screening services | ||
| Yes | 278 | 65.5 |
| No | 146 | 34.5 |
| Total | 424 | 100 |
| cervical screening is performed among women mostly in developing countries | ||
| Yes | 264 | 62.3 |
| No | 160 | 37.7 |
| Total | 424 | 100 |
| Cervical screening procedures if not adopted can cause possible onset of problems | ||
| Yes | 286 | 67.5 |
| No | 138 | 32.5 |
| Total | 424 | 100 |
Table 2: 0: Level of Knowledge of Cervical Screening Services among Females.
Perceived Risks towards Cervical Screening Services
From Table 3 below, 41.2% (175) of the females, agreed that it is risky to avoid uptake of cervical screening, 19.0% (81) strongly agreed, 6.1% (26) were undecided, 9.6% (41) disagreed, and 24.0% (102) strongly disagreed. 35.1% (149) of the respondents agreed that each time they screened their cervix, it felt so unpleasant and predisposed them to infections, 36.5% (155) were undecided, 9.4% (40) disagreed, 15.1% (64) strongly disagreed, and 4.0% (17) of the women strongly agreed. 28.2% (120) of the women strongly agreed they had a perception of experiencing a discharge following screening, 21.4% (91) agreed, 17.8% (76) disagreed, 26.9% (114) strongly disagreed, and 5.7% (24) were undecided.
30.3% (128) were undecided that every time they examined themselves they could not determine abnormalities making it unlikely to notice infection onset, 26.4% (112) strongly agreed, 0.6% (3) agreed, 18.8% (80) disagreed, and 23.9% (101) strongly disagreed. Over half of the respondents ‘strongly disagreed’ that their friends always advised them against cervix screening, 23.8% (101) disagreed, 5.8% (25) remained undecided, 10.1% (43) agreed, and 6.2% (26) strongly agreed. When the women were asked if cervical screening was a waste of time to them 28.5% (121) agreed, 27.4% (116) undecided, 17.1% (73) strongly disagreed, 14.4% (61) disagreed, and 12.6% (53) strongly agreed.
| Frequency (n=424) | Percentage (%) | |
|---|---|---|
| It is risky to avoid _uptake of cervical screening | ||
| Strongly agree | 81 | 19.0 |
| Agree | 175 | 41.2 |
| Undecided | 26 | 6.1 |
| Strongly disagree | 102 | 24.0 |
| Disagree | 41 | 9.6 |
| Total | 424 | 100 |
| For me each time I screen my cervix it feels so unpleasant and predisposes me to infections | ||
| Strongly agree | 17 | 4.0 |
| Agree | 149 | 35.1 |
| Undecided | 155 | 36.5 |
| Strongly disagree | 64 | 15.1 |
| Disagree | 40 | 9.4 |
| Total | 424 | 100 |
| I have a perception of experiencing a discharge following screening | ||
| Strongly agree | 120 | 28.2 |
| Agree | 91 | 21.4 |
| Undecided | 24 | 5.7 |
| Strongly disagree | 114 | 26.9 |
| Disagree | 76 | 17.8 |
| Total | 424 | 100 |
| Anytime I examine myself I cannot determine abnormalities making it unlikely to notice infection onset | ||
| Strongly agree | 112 | 26.4 |
| Agree | 3 | 0.6 |
| Undecided | 128 | 30.3 |
| Strongly disagree | 101 | 23.9 |
| Disagree | 80 | 18.8 |
| Total | 424 | 100 |
| My friends always advise me not to screen the cervix | ||
| Strongly agree | 26 | 6.2 |
| Agree | 43 | 10.1 |
| Undecided | 25 | 5.8 |
| Strongly disagree | 229 | 54.0 |
| Disagree | 101 | 23.8 |
| Total | 424 | 100 |
| Cervical screening is a waste of time to me | ||
| Strongly agree | 53 | 12.6 |
| Agree | 121 | 28.5 |
| Undecided | 116 | 27.4 |
| Strongly disagree | 73 | 17.1 |
| Disagree | 61 | 14.4 |
| Total | 424 | 100 |
Table 3: 0: Perceived Risks towards Cervical Screening Services.
Level of knowledge of Cervical Screening
From Table 4 below, majority of the respondents reported demonstrated their approval to utilize cervix screening if offered a chance (85.9%), while 14.1% (60) denied. 40.7% (173) of the respondents could not remember if they had been advised by a physician to screen the cervix prior to the time of this investigation, 39.1% (166) reported ‘Yes”, and 20.1% (85) said “No”. 56.0% (237) of the respondents could also not tell if they had screened for cervical or any infection relating to the cervix before filling the questionnaire, 33.2% (141) replied “No”, and 10.9% (46) said “Yes”. 28.5% (13) of the respondents who reported ‘yes’ said they screened between 2-3 months ago, 27.4% (12) reported 4-6 months ago, 17.1% (8) said “6 months to a year”, 14.4% (7) reported longer than one year, and 12.6% (6) reported ‘in less than a month’. When they were asked concerning reasons for cervical screening, 28.5% (13) of the females each reported that they were presented with symptoms and as a result of cases in the family respectively, 27.4% (12) reported ‘for prevention’, and 17.1% (8) of the respondents just decided to go for the examination. 74.7% (34) of the females had never had an abnormal test result in cervical screening, while 25.3% (12) reported ‘Yes’.
| Variable | Frequency (n=424) | Percentage (%) |
|---|---|---|
| Will you utilize cervical screening if offered a chance? | ||
| Yes | 364 | 85.9 |
| No | 60 | 14.1 |
| Total | 424 | 100 |
| Has any physician advised you to screen the cervix before? | ||
| Yes | 166 | 39.1 |
| No | 85 | 20.1 |
| Cannot Remember | 173 | 40.7 |
| Total | 424 | 100 |
| Have you screened for cervicalor any infection relating to the cervix before? | ||
| Yes | 46 | 10.9 |
| No | 141 | 33.2 |
| Cannot Remember | 237 | 56 |
| Total | 424 | 100 |
| If YES when was that? | ||
| less than a month | 6 | 12.6 |
| 2-3 months | 13 | 28.5 |
| 4-6 months | 12 | 27.4 |
| 6 months to a year | 8 | 17.1 |
| longer than a year | 7 | 14.4 |
| Total | 46 | 100 |
| What was your reason for the cervical screening? | ||
| Presented with symptoms | 13 | 28.5 |
| cases in the family | 13 | 28.5 |
| For prevention | 12 | 27.4 |
| Just decided to go for the examination | 8 | 17.1 |
| Total | 46 | 100 |
| Have you ever had abnormal test result in cervical screening? | ||
| Yes | 12 | 25.3 |
| No | 34 | 74.7 |
| Total | 46 | 100 |
Table 4: 0: Level of level of knowledge of Cervical Screening.
Factors Affecting the Utilization of Cervical Screening Among Females
Table 5 below demonstrated the factors affecting the utilization of cervical screening practice among women in this survey. 19.3% (82) reported family/husband acceptance, 18.7% (79) said “distance to facility”, 13.8% (58) reported lack of information, 13.3% (56) financial constraints, 11.3% (48) behavior of health workers, 10.0% (42) cultural related factors, and 0.5% (2) said “religious factors”.
| Variable | Frequency (n=424) | Percentage (%) |
|---|---|---|
| Which of the following related as possible factors affecting your Utility of cervical screening | ||
| Family/Husband Acceptance | 82 | 19.3 |
| Cultural related factors | 42 | 10.0 |
| Distance to facility | 79 | 18.7 |
| Financial Constraints | 56 | 13.3 |
| Lack of Information | 58 | 13.8 |
| Religious Factors | 2 | 0.5 |
| Behavior of Health workers | 48 | 11.3 |
Table 5: 0: Factors Affecting the level of knowledge of Cervical Screening among Females.
Association between the level of knowledge of cervical screening services and the Socio demographic characteristics of females
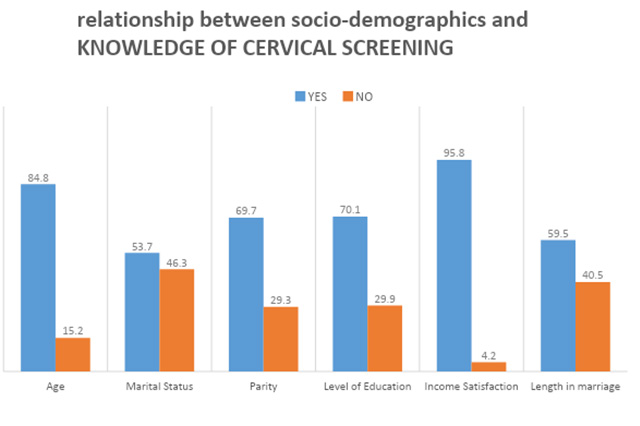
Table 6 below showed the results for the test of a statistically significant association between socio- demographic characteristics and level of knowledge of cervical screening services among females in Owerri-West Local Government Area, Imo State (see Figure 2 below). There was a statistically significant association between age of women and level of knowledge of cervical screening services (p= 0.010). Given the association between marital status of females and level of knowledge of cervical screening services among women in the study population (p=0.300), there was no significant association. On the hypothesis between number of children (parity) and level of knowledge of cervical screening services among women in primal population. There was also a statistically significant association (p=0.0008). Given the association between level of income of women and level of knowledge of cervical screening services in the study population, there was a statistically significant association (p=0.0092). There was a statistically significant association between level of education and level of knowledge of cervical screening services in the study population (p=0.0327). Finally, there was no statistically significant association between occupation and level of knowledge of cervical screening services in the study population (p=0.127).
| Socio Demographics | Level of knowledge of cervical screening services | X2 | P-value | Decision | |
|---|---|---|---|---|---|
| Yes (%) | No (%) | ||||
| Age | 84.8% | 15.2% | 12 | 0.010 | S |
| Marital Status | 53.7% | 46.3% | 2 | 0.300 | NS |
| Number of Children (Parity) | 69.7% | 29.3% | 3.33 | 0.0008 | S |
| Level of income | 95.8% | 4.2% | 8.57 | 0.0092 | S |
| Level of Education | 70.1% | 29.9% | 17 | 0.0327 | S |
| Occupation | 59.5% | 40.5% | 1.97 | 0.127 | NS |
Table 6: 0: Association between the Level of knowledge of cervical screening services and the Socio demographic characteristics o
Association between the utilization of cervical screening services and the knowledge of cervical screening services among females
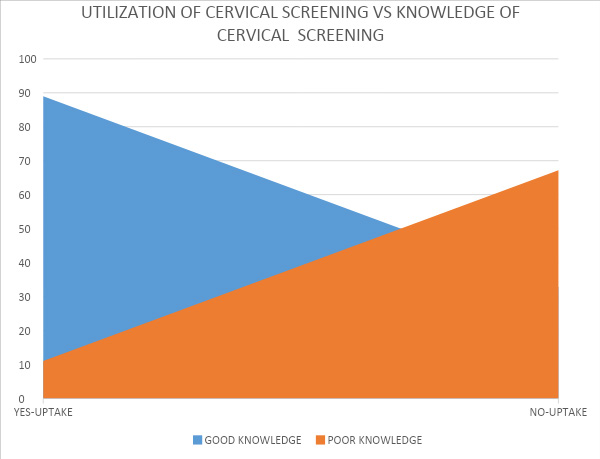
Table 7 below showed the results for the test of a statistically significant association between knowledge of cervical screening and utilization of cervical screening among female females. There was a statistically significant association between good knowledge and utilization of cervical screening among females (p= 0.00532) (see Figure 3 below).
| Utilization of cervical screening | Knowledge of cervical screening | X2 | P-value | Decision | |
|---|---|---|---|---|---|
| Good Knowledge (%) | Poor Knowledge (%) | ||||
| Yes | 89.0% | 11.0% | 0.2376 | 0.00532 | Sig |
| No | 32.8% | 67.2% |
Table 7: Association between the level of utilization of cervical screening services and the knowledge of cervical screening serv
Discussion
Based on the findings of this study on the socio demographic characteristics of the respondents, it revealed that 27.8%of the females were in the age range of 25-34 years. This finding goes in consistent with a statement in a publication by Oche, et al. [7] that females in a cervical survey conducted among participants in Benue, had a mean age of 30 years. Further findings of the study showed that the respondent’s majority were Christians (65.1%) and of Igbo origin (65.8%). This could be due to the fact that the study was conducted in the south-eastern part of Nigeria predominated by people of Igbo and Christian origin.
Findings from this study posited based on the level of knowledge towards cervical screening among females, ‘Yes’ responses received were 85.8% and 14.2% negative. This corroborates with previous findings on the knowledge of cervical screening. In the study, 23.8% of the females listed ‘social media’ as their source of information on cervical screening. This could be due to several media campaigns and awareness on cervical. Additionally, 53.0% of the respondents correctly affirmed family history of cervical is a risk for cervical screening strategies. This is however in contrast with a study by Ferlay, et al. [1], conducted in Uganda. From this study, it was revealed that 64.2% accepted that cervical screening is performed to ensure that the cervix is free from infection and 74.6% accepted cervical is diagnosed with Pap smear. A research article by Bruni, et al. [3] revealed figures which corroborate this finding. Further investigation showed that 35.8% did not agree. Ndikom CM, et al. [8] revealed figures which demonstrated otherwise. This could be due to lack of formal knowledge on cervical screening. The females also obliged that digital cervix examination is used for cervical screening (65.5%), and 62.3% of the respondents accepted that cervical screening is higher among women in developing countries. A survey conducted among women in Anambra suggested similar responses [1]. Concerning the perceived risks towards cervical screening, study showed that 41.2% of the females correctly ‘agreed’ that it was risky to avoid up taking cervical screening, the next common response included 19.0% of the female females who ‘strongly agreed’. Similar findings on the perceived risks of cervical screening among women in Sudan suggested that over half of the respondents ‘agreed’ to the importance of cervical screening. Additionally, a study by Awodele, et al. [9], conducted in an Ibadan medical facility revealed that 29.5% of the midwives in a survey emphasized the advantages associated with cervical screening uptake. The females 35.1% of the respondents agreed that each time they screened their cervix, it felt so unpleasant and predisposed them to infections, although further investigation revealed that 36.5% were undecided. A statement in a publication by Tarney, et al. [10] corroborates this finding but goes against an observation by NCI [11]. This study showed that 30.3% of the females were undecided that every time they examined themselves they could not determine abnormalities making it unlikely to notice infection onset. The reason for the prevalence of this reply could be due to lack of proper enlightenment on cervical screening among relevant population. 28.5% of the females ‘agreed’ that cervical screening was a waste of time to them. A study according to Tanturovski, et al. demonstrated similar figures concerning misconceptions on cervical screening [17].
85.9% of the females demonstrated their approval to utilize cervix screening if offered a chance. The points out the lackadaisical attitude towards cervical screening among respondents. Although 56.0% of the respondents could also not remember if they had screened for cervical or any infection relating to the cervix during this study, 33.2% reported otherwise. A study by Mlange, et al. [18] corroborates this finding. This study revealed that 74.7% of the females had never had an abnormal test result in cervical screening as supported by several studies [19].
The finding of the study revealed that the commonest factor affecting their utilization of cervical screening was ‘family/husbands acceptance’ (19.3%). This goes in consistence with a study by Behnamfar, et al. [20] on the utilization of cervical screenings. Another study goes contrary to this finding and suggests that 26.6% of women who underwent cervical screenings listed affecting factors such as financial constraints, followed by distance to facility [3]. Findings from this study regarding the association between Socio-demographic characteristics and utilization of cervical screening among females revealed that Age is significantly associated with utilization of cervical screening among females (p = 0.010). Study shows that older women groups utilized cervical screenings relative to younger groups. This goes in line with a study by Mwaka, et al. [21] which found age to be associated with utilization of cervical screening (p = 0.00271). Further investigation into the study demonstrated that marital status is also significantly associated with the utilization of cervical screening (p = 0.300) [22]. There was no significant association. This implies that women who wanted to utilize screenings did, irrespective of their marital status. Also, from the study among females in Owerri-west, it was posited that there was a significant association between number of Children (Parity) and utilization of cervical screening among females in the study population (p =0.0008). Considering the hypothesis between level of income of females and utilization of cervical screening, there a significant association (p =0.0092). This goes in consistence to a previous study by Tanturovski, et al. [17]. This informs that females with better level of income are more likely to utilize cervical screenings. This study also indicates that females with higher level of education were significantly involved in cervical screening than those with low levels of education. Females without any formal education level barely came in for screening. This indicates that more enlightened a patient is, the more possible they are to undertake cervical screenings. Hence level of education of females and utilization of cervical screening are significantly associated (p = 0.0327). A preceding study by Mlange, et al. [18] confirms this finding. Findings of this study showed an association between knowledge of cervical screening and utilization of cervical screening among female females (p= 0.00532). This implies that females who were well informed know the importance and would easily seek cervical screening as opposed to those who lacked information. A study by Ovalle, et al. [19] corroborates this finding.
Conclusion
In this study, it was discovered that age, educational level, level of income, marital status and knowledge were all related with utilization of cervical screening among the females. Findings from this study establish that even though a number of females showed considerable knowledge of cervical screening, several others are deficient of relevant information and is a challenge. Overall, study showed good knowledge of the perceived risks of cervical screening among the females but this did not translate to willingness to utilize screening. This study emphasizes that there is a need for the state health system to address the perceived factors affecting cervical screening utilization where it may, encourage awareness campaigns and implement health policies to support utilization of cervical screening among females in Owerri-west.
The study recommends that awareness campaigns must provide accurate information on cervical screening so that females can make informed choices. Also, emphasis must be made on the importance and effectiveness of cervical screening and treatment when detected. Thus, information is important, but must be combined with prescriptive information about how to take preventive action. Accessibility to screening facilities must as well be improved and policies, implemented, to accommodate low income earners and encourage cervical screening.
References
-
Ferlay J, Shin HR, Bray F (2010) Estimates of Worldwide Burden of Cancer in 2008: GLOBOCAN 2008. International Journal of Cancer 127(12): 2893-2917.
-
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, et al. (2012) Estimated Cancer Incidence, Mortality And Prevalence Worldwide 10 In 2012 V1.0. IARC, Lyon, France.
-
Bruni L, Barrionuevo-Rosas L, Albero G, Serrano B, Mena M, et al. (2017) Human Papillomavirus and Related Diseases Report: Ico HPV Information Centre.
-
Bruni L, Barrionuevo-Rosas G, Albero U (2014) Human Papillomavirus and Related Diseases in Kazakhstan Tech. Rep., Ico Information Centre on HPV and Cancer (HPV Information Centre), Barcelona, Spain, Summary.
-
Dim CC (2012) Towards Improving Cervical Cancer Screening in Nigeria: A Review of the Basics of Cervical Neoplasm and Cytology. Nigerian Journal of Clinical Practice 15(3): 247-252.
-
Nwozor CM, Oragudosi AL (2013) Awareness and Uptake of Cervical Cancer Screening Among Women in Onitsha, South-East, Nigeria. Greener Journal of Medical Sciences 3(8): 283-288.
-
Oche MO, Kaoje AU, Gana G (2013) Cancer of the Cervix and Cervical Screening: Current Knowledge, Attitude, and Practices of Female Health Workers in Sokoto, Nigeria. International Journal of Medicine and Medical Sciences 5(4): 184-190.
-
Ndikom CM, Ofi BA (2012) Awareness, Perception And Factors Affecting Utilization Of Cervical Cancer Screening Services Among Women In Ibadan, Nigeria: A Qualitative Study. Reproductive Health 9(11).
-
Awodele AA, Adeyomoye DF, Awodele V, Kwashi IO, Awodele ADC, et al. (2011) A Study on Cervical Cancer Screening amongst Nurses in Lagos University Teaching Hospital, Lagos, Nigeria. Journal of Cancer Education 26(3): 497-504.
-
Tarney C, Han J (2014) Postcoital Bleeding: A Review on Etiology, Diagnosis, and Management. Obstetrics and Gynecology International 2014: 192087.
-
National Cancer Institute (2014).
-
Dhendup J, Tshering U (2014) Harrison’s Principles of Internal Medicine. Editors of Previous Edition. In: Harrison TR (Ed.), 17th (Edn.), New York, Mcgraw-Hill Medical, USA, pp: 608-609.
-
Urasa M, Darj E (2007) Knowledge of Cervical Cancer And Screening Practices of Nurses at a Regional Hospital In Tanzania. African Health Sciences 11(1): 48-57.
-
Arulogun OS, Maxwell OO (2012) Perception And Utilization Of Cervical Cancer Screening Services Among Female Nurses in University College Hospital, Ibadan, Nigeria. Pan African Medical Journal 11: 69.
-
Siegel D, Naishadham N, Jemal A (2012) Cancer Statistics, Ca: A Cancer Journal for Clinicians 62(1): 10-29.
-
Yu F, Murugiah MK, Khan A, Mehmood T (2015) Meta- Synthesis Exploring Barriers to Health Seeking Behaviour among Malaysian Breast Cancer Patients. Asian Pacific Journal of Cancer Prevention 16(1): 145-152.
-
Tanturovski D, Zafirova E, Stojovski M, Basheska N, Jovanovska V (2013) Impact of socio-demographic factors on the delayed diagnosis and advanced stage presentation of patients with invasive cervical cancer in Macedonia. Makedonska akademija na naukite i umetnostite. Oddelenie za medicinski nauki 34(3): 71- 78.
-
Mlange R, Matovelo D, Rambau P, Kidenya B (2016) Patient and Disease Characteristics Associated With Late Tumour Stage At Presentation Of Cervical Cancer in Northwestern Tanzania. BMC 16.
-
Ovalle WK, Nahirney PC (2013) Illustrations. In: Frank H Netter (Ed.), Contributing Illustrator, Joe Chovan. Female Reproductive System, Netter’s Essential Histology. 2nd (Edn.). Philadelphia, Pa: Elsevier/Saunders, pp: 416.
-
Behnamfar F, Azadehrah M (2015) Factors Associated With Delayed Diagnosis of Cervical Cancer in Iran - A Survey in Isfahan City. Asian Pacific Journal of Cancer Prevention 16(2): 635-639.
-
Mwaka AD, Garimoi CO, Were EM, Roland M, Wabinga H, et al. (2016) Social , Demographic And Healthcare Factors Associated With Stage At Diagnosis of Cervical Cancer: Cross-Sectional Study in a Tertiary Hospital in Northern Uganda 6(1): 1-10.
-
Saghari S, Ghamsary M, Marie Mitchell A, Oda K, Morgan WJ (2015) Annals of Epidemiology Sociodemographic Predictors of Delayed-Versus Early-Stage Cervical Cancer in California. Contributions Sec Med Sei 34(3): 71-78.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria