A Family Doctor’s Clinical-Epidemiological Diary in Spain of the Times of Covid-19. February 24 to March 15: Is Covid-19 A Lottery?
Since outbreak of coronavirus disease 2019 (COVID-19) started in late December in China, there are many scientific articles that have been published about this virus. However, data and qualitative research are lacking. In this sense, a diary written by a family doctor in Spain during the COVID-19 pandemic is presented, which can constitute a qualitative clinical-epidemiological database and a tool to estimate effects. The diaries are not only a literary variant, but can be a method of qualitative and quantitative research, as well as reflection. Here will be presented, in several chapters, the first-person account of the work experience of a family doctor, who for clinical and epidemiological purposes resembles the naturalist and ethnographer, carrying his “field notebook.†It may be that experience may not be like being in the hospital emergency room or wards or in Intensive Care Units. His practice is in a health center in Toledo (capital of Castilla La Mancha, Spain), with a surgery that has a list of 2000 patients over the age of 14, and he treats an average of 30-35 patients every day in 8-hour work days. But, of course, that was under normal circumstances, before the times of COVID-19. This is “Chapter 1 (from February 24 to march 15): is COVID-19 a lottery?â€, that collects the annotations of the beginning of the outbreak which was believed impossible that a problem of medical interest in Spain would become.
Introduction
Diaries are not only a literary variant, but can be a method of investigation and reflection [1, 2]. Diary method is a qualitative (and quantitative) study tool. What is a diary of the family doctor/general practitioner)? It is a first-person account of the work experience, documented through regular and sincere entries, which the reader can later analyze through recurring patterns or the most relevant events [3, 4, 5], as well as the symptoms or experiences regarding diseases and infections [6]. In addition it is usefulness as Thesis an educational tool [7], for evaluation [8], and regarding clinical and epidemiological evolution of various diseases and epidemics [9, 10, 11]. Personal diary narration includes an autobiography but shows the environment in which it is written, which describes the ordinary, but at the same time deep and turbulent events. A family doctor’s diary refers us to the invaluable value of the particular to understand the general [12, 13].
In December 2019, a cluster of pneumonia cases emerged in Wuhan City, Hubei Province, China, with common exposure to a wholesale seafood, fish, and live animal market. On January 7, 2020, the Chinese authorities identified as a causative agent of the outbreak a new virus of the Coronaviridae family that was later named SARS-CoV-2. The genetic sequence was shared by Chinese authorities on January 12. The disease caused by this new virus has been named by international consensus COVID-19. The International Health Regulations Emergency Committee declared the outbreak as a Public Health Emergency of International Importance at its meeting on January 30, 2020. Subsequently, the WHO recognized it as a global pandemic on 11 March 2020, and it continues to spread affecting many countries and territories around the world [14, 15, 16]. Its figures are rapidly changing, and when this is written, as of April 24, 2020, the pandemic has infected more than 2,700,000 people and killed more than 190,000 worldwide; The United States has more than 870,000 cases, followed by more than 219,000 in Spain, and more than 189,000 in Italy, which have overtaken China in the total number of COVID-19 cases [17].
In recent months, an increasing amount of information on different aspects of COVID-19, is being published [18]. But, despite the excess of quantitative biomedical information, qualitative data and research are lacking. In this context, a diary written by a family doctor in Spain during the COVID-19 pandemic is presented, which can constitute a qualitative clinical-epidemiological database and a tool to estimate effects.
Method
Within the broad spectrum of naturalistic research, diary studies are “first-person case studies.” Diary studies can be valuable investigative procedures. Diary studies have certain advantages, among others, the following [19]: 1) The author-researcher can recognize and study different factors and variation of data and attitudes across the diary. 2) They can show evidence of the incredible diversity of situations. 3) From the diary we can contemplate factors identified as important and that the researcher could have considered as not worthy of study. 4) His technique is simple.
The field diary is classified as an unsystematized personal recording instrument in which it is recorded facts, data, and the experiences of the observer or other individuals. Annotations allow the observer to record and review their emotions [3, 4, 5]. A personal diary (or life diary/ field diary) is a subgenre of biography and specifically of autobiography. This “diary of the times of the covid-19” is a text that, in a fragmentary way and with the registration of the date, the author, family doctor of a health center in Toledo (Spain), writes the narration of personal experiences, some meditations and events that affect him. The diary refers to the brief time frame of the “COVID-19 era that the author had to live from his position as family doctor.
It may be that his experience is similar to that of other doctors; perhaps not those who are working in hospital emergencies or hospital wards or in intensive care units (UCI). The author realizes that, compared to other medical colleagues, he is in a privileged position: he has not to treat patients on the brink of life and death or decide whether to intubate or accept them into the ICU, etc. But the uncertainty is disturbing in all problems. Further, there is the greatest daily concern: the possibility of contracting infection [20, 21]. The Family Doctor surgery has a list of 2000 patients over the age of 14 (in Spain, family doctors care for patients over the age of 14), it is in a health center in a peripheral neighborhood of Toledo (capital of Castilla La Mancha, Spain), and which has about 20,000 predominantly young inhabitants, and each day he treat an average of 30-35 patients, with very varied health problems, in 8 hours of work. But, of course, that was under normal circumstances, before the “times of COVID-19.” This Diary will have the following chapters, that although they are separate texts for easy reading, and represent three different stages of the COVID-19 epidemic, they are a single “times of COVID-19” story:
- Chapter 1: February 24 To March 15: Is Covid-19 A Lottery?
- Chapter 2: March 16-31: The Big Bang
- Chapter 3: April 1 To 31: Some Good News And Hope By The End
Chapter 1: From February 24 to March 31: Is Covid-19 a Lottery?
February 24, 2020
At home. After 4 days of vacation in Lombardy (Italy). My wife and I had it planned months ago. It is true that I knew that there was an outbreak of COVID-19 [22] with more than 76,000 cases reported in mainland China and 1,875 cases in locations outside of mainland China, as well as more than 2,000 associated deaths worldwide. In Spain, the Health Authority spoke for the first time of suspected cases of COVID-19 on January 25, 2020; however it was confirmed that they had given negative. The first infected was confirmed on the 31st of that month (an imported case). On February 10 there was another case also imported. The Health Authority affirmed on February 23: “In Spain there is neither a virus nor is the disease being transmitted” [23].
China is very far from Spain: the distance from Wuhan
(China) to Toledo (Spain) is 9921 km! But... the European Center for Disease Prevention and Control warned on January 18 that Wuhan Airport had six direct weekly flights to Paris, three to London and another three to Rome ... [24].
Now I have come home to Toledo after the 3 day trip to Bergamo, Lake Como and Milan. The plane from Madrid to Milan left an hour late, but otherwise everything was normal (maybe even the delay), but when I arrived at the Orio al Serio Airport in Bergamo, they made me check with thermometers without contact to detect fever, and the operators who carried it out wore personal protective equipment. I was shocked to see these people dressed as in biological threat movies. On the 25th I was in Lecco, Varenna and Bellagio. Lake Como with the Alps in the background was beautiful. But I started seeing people with masks... The truth is that I was surprised. I had not seen that before. From the 22nd, already in Milan, television continuously showed scenes of COVID-19 patients in the town of Condongo. So, I learned that a group of cases had been detected, starting with 16 confirmed cases in Lombardy on February 21, an additional 60 cases on February 22; the first deaths in Italy were reported the same day. There are 50,000 isolated people [25].
My visits in Milan on February 23, to the Basilica of San Ambrosio, Duomo..., I could not do them calmly, thinking about the coronavirus. The number of people with masks increased every hour, in the subway, on the street… I tried to buy masks in the pharmacy and there was no existence; Finally, I arrived in Spain. At Madrid airport there was no control, no people with masks. I am already at home in Toledo. I have escaped the virus..., I have left the virus behind... At home I wonder if I should quarantine before joining the consultation. I watch my temperature: I don’t have fever; no other symptoms. Except maybe that I feel kind of dizzy. I imagine it is stress, anxiety. I look on the Internet for the recommendations of the Spanish Health Authority for people who come to Spain from areas at risk of COVID-19: As a general guideline, at the present time it is not being recommended neither by international organizations nor by the Ministry of Health the quarantine of people returning from risk areas, nor are extraordinary control measures being carried out at the entry points [26].
From Milan to Toledo there are more than 1,500 km; it is far... It is much closer than Wuhan..., but still far... The first registered patient in Spain with COVID-19 was known on January 31. He was a German patient and was infected, presumably, by contacting in Germany. Nine days later, another case of COVID-19 was detected in Palma de Mallorca. But it was not until February 24 when the virus spread to the Iberian peninsula, detecting the first cases in Madrid, Catalonia and Valencia.
Am I aware that as the COVID outbreak consumed the city of Wuhan in China, new cases of the virus may start to spread like sparks thrown by a fire? Maybe some of those cases can land thousands of miles away [27].
February 25
I am in my surgery. It is 7 AM. I am preparing the consultation that I will begin at 8 AM. I have 40 patients cited. Although I do not tell anyone, I am somewhat afraid of the COVID-19 outbreak...
The consultation has gone as usual: I had two kidney colic, a 66-year-old man and a 46-year-old woman; a 74-year-old man with a surgical wound dysfunction after eventroplasty; a 29-year-old woman “again with cystitis”; a 63-year-old man with benign prostatic hypertrophy; a 34-year-old man who jumped supporting the right heel 3 days ago; a 65-year-old woman with hallux valgus; a 77-year- old man with sialoadenitis; a 36-year-old woman to control a normal pregnancy; a 39 year old woman with couple problems; a 27-year-old woman with multiple and numerous hyperpigmented papulas; several patients with low back pain, one male with multimorbidity to control diabetes mellitus, hypertension, hypertrophic cardiomyopathy, stroke, hepatic steatosis..., one patient with insomnia, and another with chronic cough. There has been a male with diarrhea, and three patients aged 36, 76 and 14 with acute respiratory infections. Aren’t they COVID-19 (fever, cough, and shortness of breath)? Am I sure I had no cases? [28, 29]. I wonder if the outbreak of COVID-19 from China was a surprise case, or not so surprise [30, 31, 32, 33].
26 of February
I have attended 36 patients. I have started to ask about trips to China or Italy in acute respiratory infections. But the consultation was uneventful: Atopic dermatitis, bronchial asthma, atrophic vaginitis, ototubaritis, allergic rhinitis, sciatica, gonarthrosis, 4 patients to control hypertension, valvulopathy in a 59-year-old woman, oral candidiasis in a diabetic patient, pruritus, cystitis, tenosynovitis, 2 diabetes mellitus, hypothyroidism, psoriasis, pregnancy, anxiety due to work situation... And... 2 upper respiratory tract infections that had not traveled to China or Italy.
I read the new: In Spain, on February 25, the “third case”, also imported, was detected. However, on February 26, today!, the first native infected person was known, a 62-year- old man who had not traveled to any risk area. “The virus has been circulating in Spain for several days and we had not detected it,” explained the head of the infectious diseases department of a large hospital [34].
Since when can the virus be circulating in the community?
A week, a month, two months ago...? [35].
February 28th
It seems to me that we all think that we are safe from the virus; that we are far from Italy and China, and that the outbreak cannot occur here... It would be very difficult for us “to win the lottery”...
I have been monitoring my temperature for almost a week, and I am asymptomatic, but worried about whether I am doing the right thing... I am normally doing the consultation. Everything is normal there. At least I think so.
41 patients: low back pain, allergic rhinitis and chronic rhinitis, seborrheic dermatitis, headache, psoriasis, desire for pregnancy, hypertension, osteoarthritis, eyelid stye, acne, asthma, dyspesia, osteoporosis, dysmenorrhea, unspecified arthralgias, asthenia, candidiasic vaginitis, depression, cytology request…, an 81-year-old man with multimorbidity (Crohn’s disease, hiatus hernia, esophagitis, hypertension, coronary heart disease, glaucoma, dysthymia, insomnia...).
And 7 respiratory infections: 29-year-old man with dyspnea and wheezing, 51-year-old woman with cough, 20-year-old woman with cough, 18-year-old man with cough, 55-year-old woman with cough and odynophagia, 46-year-old woman with “flu”, and 33-year-old woman, nurse, who has had respiratory infection for 15 days with cough, dyspnea, fever, headache that she describes as “diffuse cranial cushioning and dizzy” She was sent to the emergency department and a chest x-ray was performed without pulmonary infiltrates. It is considered a nonspecific clinic with respiratory symptoms without complications radiological.
Are there many respiratory cases? Could any of these be COVID-19? Could these respiratory or digestive symptoms correspond to COVID-19? I have no answer. I can only wait and see. Polymerase chain reaction (PCR) tests are not being done, except occasionally in hospital.
The number of affected increases to fifty in Spain [34]. Are they all imported cases? I think about what I would do if I were infected: how would I do insulation at home? I’d be in a room… maybe the bedroom… and I’d have to bring a table for the laptop… plus that room is next to a bathroom. Luckily the house is big and there are two bathrooms.
February 29
Today is Saturday and I did not make the consultation, but since I am nervous, I ended up calling the Primary Care Management and the Local Epidemiology Service by phone. They are kind; It seems to me that they smile condescendingly... They advise me to measure my temperature... and not to mention my trip to Milan to my colleagues at the Health Center so as not to generate anxiety.
Tomorrow a cardiology resident joins my practice, who must undergo an apprenticeship in family medicine. Should she really be incorporated? I call her on the phone. and I advise her to delay joining for a week. So, it would be 15 days from my trip to Milan.
I read the news: The first person to die from the disease in the United States had been a man in the vicinity of Seattle on February 29. Is COVID-19 infection now starting in the United States or has the coronavirus been around for some time? [36].
March 1st
A case. In my region, Castilla-La Mancha, the first positive case for COVID-19 has been registered. This is a 62-year-old man, seriously ill, with pneumonia. In Spain the positive cases rise to 83, who have had contacts in northern part of Italy, where the largest European outbreak continues.
Today is Sunday... I will see tomorrow in the consultation... I am restless.
March 4
When I returned from Milan I thought I had escaped the virus… I had moved away from Milan, and therefore from the outbreak, and I was safe! But no, I was wrong! The virus followed in my footsteps; it’s here too. And I can’t escape.
In Spain, the “first death” was known today: a 69-year- old man who had died on February 13 and in whom COVID-19 had been detected in a subsequent autopsy. It was assumed that “obviously there was some kind of community transmission” [37].
I speak with the Coordinator of the training of resident doctors. The cardiology resident who should rotate with me this month will join next Monday. The question I ask myself is the suitability of your rotation right now. I propose to postpone the rotation.
36 Patients: There is a first visit of a 59-year-old woman with hypertension, diabetes and stroke, a 63-man with multimorbidity and polypharmacy, a 37-year-old woman with arthritis, a 56-year-old man with meralgia paresthetica and hypertension, a woman of 82 with hypertension... and... Other patients with: dental phlegmon, pregnancy, asthenia, anticoagulation controls with warfarin, depression, vertigo, anxiety, dyspepsia, vaginitis...
What about respiratory infections?: a 29-year-old man with a cough and odynophagia, a 41-year woman (pediatric nurse in the hospital), with a cough; her son with cold; Both have been in Valencia (area with coronavirus cases, but not declared at risk); Pediatrician advised the isolation of his son at home; I do same advice, isolation 14 days at home. And a 57-year-old man with a cough, a 20-year-old woman with a cough, another 55-year-old woman also with a cough, an 18-year-old man with a cough from 15 days and fever, a 71-year-old woman with a morning cough, a man 38 years old with flu syndrome.
In total, 8 respiratory infections from 36 patients (22%). We are in winter. Today, March 4, COVID-19 cases rise to 12 in Castilla La Mancha. They are few. It is difficult for us to win the lottery..., fortunately. But, I am afraid that I might miss a diagnostic of COVID-19... There is still no PCR test.
March 9
26 cases, two cured in Castilla-La Mancha. In Spain: 911 infected and 25 dead. Today, the Ministry of Health had to change the scenario on which he was working to contain the epidemic, moving to a level of reinforced containment, and in a coordinated manner, the Community of Madrid decided to close all educational activity in the region [38, 39]. I wonder how a developed country that has never tackled an epidemic in the last hundred years will act to manage this viral outbreak.
37 visits: sciatica, gastroenteritis, tension headache, hair loss and iron deficiency, hypertension, osteoartritis, vertigo, dermatitis, urinary incontinence, cataract, coronary heart disease review... And a 76-year woman with cough, and a 75-year-old man also with a cough.
I start putting on masks. There are not in the center, but I keep two (that I ordered a year ago, and did not get to use, when I had to attend several times to a patient with bacilliferous tuberculosis). I will have to reuse them for quite a few days...
I have a 63-year-old patient admitted to hospital for atypical pneumonia or COVID-19? The boundaries between SARS-CoV-2 pneumonia and atypical pneumonia caused by other agents, such as Legionella pneumophila, Mycoplasma pneumoniae, influenza A and B, rhinovirus, respiratory syncytial virus, Histoplasma capsulatum and Coccidioides immitis, can be diffuse. I have a suspicion that patients affected or even killed by COVID-10 may be “hidden.” The key would be to increase rapid diagnostic tests for COVID-19. Many times with the pure clinic it will not be possible to recognize it, because the symptoms can be very nonspecific to differentiate between one agent and another [40]. Perhaps there will come a time when every respiratory clinic will be labeled, without PCR, as COVID-19
March 12
2,671 infected and 63 deaths in Spain. Castilla-La Mancha registered the first positive case for coronavirus on March 1 and the first died is today, March 12.
I begin to reproach the patients who consult in person, when the reason for the visit is trivial: they do not realize the situation of the COVID-19!
38 visits. The morning is complicated... 7 respiratory infections... and some it seems to me that it could be COVID-19: 51-year-old woman with a cough without fever, a 32-year-old woman with a fever, cough, general malaise, from 3 days after traveling to Albacete. I speak with Epidemiology Service; they tell me to act like a normal flu. However, I advise isolation at home and use of a mask. That did not indicate it until now in cases of influenza ...; Another 51-year-old woman with a cough without fever or general involvement; a 69-year-old man with exacerbated COPD; a 29-year-old woman with a cough and sore throat for 2 days, without fever or contacts or travel (but her partner traveled, although he is asymptomatic); a 63-year-old man with cough and dyspnea from 2-3 days and his brother with coronavirus pneumonia (doubtful) remained at his house until 10 days ago ... In addition, he says that there is an outbreak of cases in the prison where he works. I speak to Epidemiology Service again…, but it is not clear what to do!; other 35-year-old woman with a dry cough in intense episodes and odynophagia, without fever... And a 40-year- old man with a cough apparently from the beginning with angiotensin-converting-enzyme inhibitor 20 days ago. (Well, this case is different! I’m sure?).
Can there be infections in presymptomatic stages of the disease? COVID-19 could be much more than a respiratory disease? [41]. I think that 10% of cases can be overlooked in the initial diagnosis only by symptoms [42].
March 13
41 patients. I begin to try patients not to come personally to the consultation and some respiratory patients already call by phone instead of coming to the consultation.
There was a 49-year-old man with a cough, another 33-year-old man with a cough, another with odynophagia, another 58-year-old man who followed rhinorrhea and odynophagia, a 69-year-old man who “became ill by changes in temperature”, a woman 71 years old with cough without expectoration or fever and discreet dyspnea, for 7-10 days, and with roncus in both bases upon auscultation... I send her to the emergency department... I receive a call from a patient: He says that “he has been work in an office in Madrid, where other person who was there, was contact of cases of COVID-19; he has been at home since yesterday when he started with a fever.” I see a 37-year-old woman who says that “in the school where she works there are several cases” (unconfirmed), and yesterday she started with cough without fever. A 37-year-old man contacted with a case of coronavirus at his company; yesterday started with fever and from his company’s medical service sent him to home. Today continues with fever and discreet respiratory distress. I call the Epidemiology Service again; they are very busy; they cannot cope with all the queries they receive. They tell me to decide in my opinion... Another 36-year-old man with a cough, and he works in Madrid...
There have been 10 respiratory infections...
Yesterday in In Castilla-La Mancha: 115 cases. First deceased. Today 194 cases. Five deceased. Spain declares a state of alarm and anticipates 10,000 infected.
The reason is that Spain has already exceeded 4,200 positive cases, according to the latest update from the Spanish Ministry of Health. And 120 deaths have been recorded. The Prime Minister says that “very tough weeks await us. We cannot rule out that in the next few days we will reach the figure of 10,000 affected.” Today, March 13, the daily growth of cases in Spain is over 42%. Are we reaching the peak?
Why do some people have mild disease and others severe and even die with COVID-19? Mortality rates are higher in older people and with more comorbidities, but there are cases with horrible results, including death, in young, healthy people. That is a great variation. Some people suffer from mild illnesses, and others die, despite having very similar initial characteristics. That is why COVID-19 feels like a game of chance. Like the lottery, would it be, for example, the probability that the prize will be awarded only 0.001% (one in 100,000)? There is little chance that it will touch us... But in a study in China, thirty percent of those who died had no comorbidities at all [43]. The law of averages tells us that it is probable that the next patient is not COVID-19, nor that I am infected... But that does not matter too much when the decision is left to the lottery [44].
Conclusion
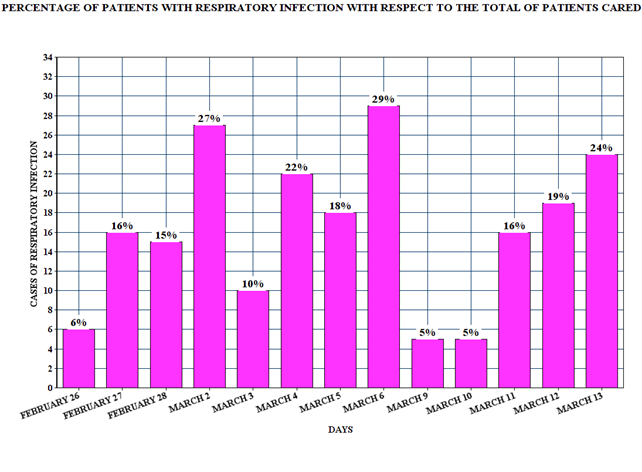
That outbreak that occurred in such distant places is already here. It was arrogant to think that the virus was left behind, elsewhere. We were not prepared. “We have won the lottery.” Is this wave going to carry us away? I don’t know how I will work in the surgery. What will happen to the outbreak? How will it affect us? What will I have to do next? I fear for myself and for how I should handle patients. I do not feel well. I am insecure and concerned. I have never experienced this. I have no guides or maps to move around in this territory. I have drawn a figure (Figure 1) with the percentage of respiratory infections over the total number of patients seen each day. Are we at the peak of the new infection curve? How will this affect the organization of my consultation?
References
-
Travers C, Schneider J, Perry-Young L, Wilkinson S, Scales K, e al. (2019) Using a Reflective Diary Method to Investigate the Experiences of Paid Home Care Workers Caring for People With Dementia. Home Health Care Management & Practice 32(1): 10-21.
-
Hodge B (2013) The Use of Symptom Diaries in Outpatient Care. Fam Pract Manag 20(3): 24-28.
-
Bowling A (2000) Research methods in health. Investigating health and health services. Diary methods. Buckingham. Philadelphia Open University Press.
-
Fernando MC, Friedeman ML, Jiménez LD, Chaparro Díaz L (2008) Researcher’s personal diary as research tool. Av enferm 26(2).
-
Elliott H (1997) The use of diaries in sociological research on health experience. Sociological Research Online 2(2).
-
Thomas SJ, Agulto L, Hendrickx K, Erpicum M, Tomashek KM, et al. (2018) Dengue illness index—A tool to characterize the subjective dengue illness experience. Plos Neglected Tropical Diseases 12(10): 0006593.
-
Munro JG (1984) Computer analysis of the student log diary: an aid in the teaching of general practice and family medicine. Med Educ 18(2): 75-79.
-
Bunce AE, Gold R, Davis JV, McMullen CK, Jaworski V, et al. (2014) Ethnographic process evaluation in primary care: explaining the complexity of implementation. BMC Health Services Research 607: 1-10.
-
Defoe D (2020) A Journal of the Plague Year. The Project Gutenberg Ebook. Text file produced by Tokuya Matsumoto.
-
Schillinger L (2020) What We Can Learn (and Should Unlearn) From Albert Camus’s The Plague. Literary Hub.
-
Guevara E (2003) The Motorcycle Diaries.
-
Heath I (1999) The general and the particular: the relevance of James Joyce to general practice. Scand J Prim Health Care 17(2): 67.
-
Báez-Montiel BB, Gutiérrez-Islas E, Bolaños-Maldonado M, Samarín E, Turabián JL (2014) The odysseys of Ulysses. A study of tales in a normal working day of the family doctor in Paraguay, Mexico, Peru, and Spain. Aten Primaria 46(2): 68-76.
-
(2020) WHO Director-General’s remarks at the media briefing on 2019-nCoV on 11 February 2020.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
Chua F, James DA, Desai SR, Barnett J, Kouranos V, et al. (2020) Monitoring the COVID-19 epidemic in the context of widespread local transmission. Lancet Respir Med 8: 1-3.
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
López Á (2020) Science is publicized openly against the coronavirus. Academia Española de Dermatología y Venereología.
-
Martínez DJ (1997) The dairy as a research instrument of the teaching-learning processes of foreign languages. Universidad de Deusto.
-
Tregoning J (2020) Coronavirus diaries: hello from home. Nature.
-
Ouyang H (2020) I’m an E.R. Doctor in New York. None of Us Will Ever Be the Same. A Covid diary: This is what I saw as the pandemic engulfed our hospitals. The New York Times.
-
World Health Organization (2020) Coronavirus disease 2019 (COVID-19) situation report–34. Geneva, Switzerland: World Health Organization.
-
Turabian JL (2020) The epidemiological hypothesis of “the trojan horse”: were hospitals the main vectors of the exponencial beginning of coronavirus disease 2019 (COVID-19) in spain and other countries?. Epidemol Int J 4(3): 1-6.
-
Ansede M (2020) Genetic analysis suggests that the coronavirus was already circulating in Spain in mid- February. El País.
-
(2020) First two died in Italy from Coronavirus, where there are 50,000 isolated people. Europa FM.
-
Ministerio de Sanidad de España (2020) Recommendations for people arriving in Spain from areas at risk of coronavirus disease (COVID-19).
-
Baker M, Fink S (2020) Solving the Mysteries of Coronavirus with Genetic Fingerprints. The New York Times.
-
Jernigan DB (2020) Public Health Response to the Coronavirus Disease 2019 Outbreak–United States, February 24. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report (MMWR).
-
Chen N, Zhou M, Dong X, Ju Q, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in wuhan, china: A descriptive study. Lancet 395(10223): 507-513.
-
Drosten C, Gunther S, Preiser W, Werf SVD, Brodt HR, et al. (2003) Identification of a Novel Coronavirus in Patients with Severe Acute Respiratory Syndrome. N Engl J Med 348: 1967-1976.
-
Peiris J, Lai ST, Poon LLM, Guan D, Yam LYC, et al. (2003) Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 361(9366): 1319-1325.
-
Song Z, Xu Y, Bao L, Zhang L, Yu P, et al. (2019) From SARS to MERS, Thrusting Coronaviruses into the Spotlight. Viruses 11(1).
-
Wit ED, van Doremalen N, Falzarano D, Munster VJ (2016) SARS and MERS: recent insights into emerging coronaviruses. Nature Reviews Microbiology 14(8): 523-534.
-
Annex: Chronology of the 2020 coronavirus disease pandemic in Spain.
-
Chiu A, Armus T (2020) Autopsies find first U.S. coronavirus death occurred in early February, weeks earlier than previously thought. The Washington Post.
-
Sandoval PXD (2020) The first deaths in the United States from covid-19 occurred weeks earlier than previously thought. The Silicon Valley County coroner confirms the coronavirus in a deceased on February 6, 23 days before the first official victim. El País.
-
Medina MA (2020) Chronology of the coronavirus epidemic in Spain in just a month and a half. El País.
-
Arroyo J, Huertas J (2020) Coronavirus: Spain moves to a scenario of “reinforced containment”. Redacción médica.
-
(2020) Madrid: coronavirus forces schools, institutes and universities to close. Redacción Médica.
-
Toche T (2020) Casos de neumonía atípica y COVID-19 causan controversia en México. Medscape.
-
Otto MA (2020) Unusual Presentations of COVID-19: ‘Our Ignorance Is Profound’. Medscape.
-
Chow EJ, Schwartz NG, Tobolowsky FA, Zacks RLT, Frazier MH, et al. (2020) Symptom Screening at Illness Onset of Health Care Personnel With SARS-CoV-2 Infection in King County, Washington. JAMA.
-
Xie J, Tong Z, Guan X, Du B, Qiu H (2020) Clinical Characteristics of Patients Who Died of Coronavirus Disease 2019 in China. JAMA Netw Open 3(4): 205619.
-
Wilson FP (2020) Like Russian Roulette: Why HCPs Are So Scared of COVID-19. Medscape.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria