A Family Doctor’s Clinical-Epidemiological Diary in Spain of the Times of Covid-19. Chapter 3. April 1 to 31: Some Good News and Hope by the End
Since outbreak of coronavirus disease 2019 (COVID-19) started in late December in China, there are many scientific articles that have been published about this virus. However, data and qualitative research are lacking. In this sense, chapter 3 (April 1-31) of a diary written by a family doctor in Spain during the COVID-19 pandemic is presented, which collects the annotations from the plateau period of new cases and declining growth rates of the epidemic. In the family medicine consultation, the usual organizational guidelines have been modified, maintaining an initial triage and telephone consultations for almost all patients. In addition there is: 1) a reduction of new cases, but without disappearing; 2) an increase in consultations to follow up verified and possible cases, verified or possible contacts, and sick leave related to these cases; 3) Rare, non-respiratory symptoms and biopsychosocial consequences of COVID-19 are beginning to be seen (dermatological, arthritis, anosmia, truncated duels, anxiety, financial problems); 4) maintenance of a large increase in consultations for anxiety secondary to COVID-19; and 5) a practically total stoppage of important new diagnoses other than COVID-19. The medical work has been less satisfactory, full of uncertainty and risks. However, some good news and hope by the end: the epidemic shows clear reductions in new cases, and COVID-19 is probably an immense opportunity for hope and improvement.
Introduction
The experience of being a family doctor is similar to that of being an ethnographer who carries out a qualitative study [1, 2, 3]. The work of the family doctor as a naturalist is supported by the “field diary” tool [4]. A field diary is a data collection instrument used especially in research activities. After recording the data, the information is subjected to Thesis evaluations and interpretations. The data collected through the field diary are of various kinds: memories, ideas, fragments of conversations, diagrams, data, figures, etc. The collected has an objective nature, but the diary is itself subjective. A good field diary enables statistical formulation, diagnosis, prognosis, and situational assessments. Similarly, it’s sequentially allows the planning of future activities necessary for research development [5, 6].
Pneumonia of unknown cause detected in Wuhan, China
was first reported to the WHO Country Office in China on 31 December 2019. The outbreak was declared a Public Health Emergency of International Concern on 30 January 2020. On 11 February 2020, WHO announced a name for the new coronavirus disease: COVID-19 [7]. Since December, 2019, COVID-19 has spread globally, and as of the writing of this article, April 30, 2020; it has infected more than 3 million people and causing more than 200,000 deaths [8, 9, 10]. In this context, despite the excess of quantitative biomedical information that is sometimes contradictory or confusing, qualitative data and research are the exception [11, 13]. In this way, a diary written by a family doctor in Spain during the COVID-19 pandemic is presented; this can constitute a qualitative clinical-epidemiological database and a tool to estimate effects.
Methods
The diary method is a qualitative (and quantitative) study tool. The methodology of this diary has been previously described [14, 15]. A field diary is a method of non-experimental scientific research. The diary is a personal writing in which there can be a narrative, description, account of events, incidents, emotions, feelings, conflicts, observations, reactions, interpretations, reflections, thoughts, hypotheses and explanations, among others. It can be full of quick, spontaneous, self-critical notes and with a certain autobiographical nuance, where there is evidence of one’s own events and those of the environment. In short, it constitutes a place from where writing can be used for [16]:
- Reflect and think in writing about lived experiences.
- Document and systematize the experience.
- Carry out experimentation tasks, since it allows making comparisons, establishing relationships between the information, establishing conclusions and making decisions about the next steps of experimentation.
This “diary of the times of the covid-19” is a text that, in a fragmentary way and with the registration of the date, the author, family doctor of a health center in Toledo (Spain), writes the narration of personal experiences, some meditations and events that affect him. The diary refers to the brief time frame of the “COVID-19 era” that the author had to live from his position as family doctor. The Familiy Doctor surgery has a list of 2000 patients over the age of 14 (in Spain, family doctors care for patients over the age of 14), it is in a health center in a peripheral neighborhood of Toledo (capital of Castilla La Mancha, Spain), and which has about 20,000 predominantly young inhabitants, and each day he treat an average of 30-35 patients, with very varied health problems, in 8 hours of work. But, of course, that was under normal circumstances, before the “times of COVID-19.” This Diary have the following chapters, that although they are separate texts for easy reading, and represent three different stages of the COVID-19 epidemic, they are a single “times of COVID-19” story:
Chapter 3: April 1 To 31: Some Good News And Hope By The End
April 1st
A medical colleague from the health center is positive COVID-19; it started with diarrhea and myalgias and the polymerase chain reaction (PCR) was positive. However, she was not treating respiratory patients and consultations were by telephone... But with her was a family medicine resident who also made guards at hospital... I imagine that the vector of infection was that resident doctor and the hospital... [17]. Spain is the country with the highest number of infections among healthcare personnel, 20% of those infected belong to this group, compared to 10% in Italy and 3% in the USA [18].
In Castilla la Mancha there are 7,047 positive cases and 774 deceased to date. The trend of the epidemic in Spain is descending, but 204,178 people have already been infected and have caused the death of at least 22,282; the number of daily deaths today rises to 430 patients, with 3,968 positive cases more than in the last 24 hours, representing an increase in infections that remains at around 2%.
I put on a cloth gown... although all the consultations are by phone and in the waiting room there are only very few patients go by to control warfarin. I had not won a gown to pass the consultation for 20 years! I was doing the consultation without any medical uniform. Also now I wear a mask all the time...
I have 32 patients on my agenda for the day. They are all telephone consultations. There are various “normal” queries: A 32-year-old man with possible bleeding hemorrhoids, a 26-year-old woman with facial herpes simplex impetiginization, a 57-year-old woman with chronic nasopharyngitis, a 14-year-old man with allergic rhinitis, a male 49-year-old with asthma, a 56-year-old man “who only wants an acetaminophen recipe to have at home”, a 29-year- old woman with renal colic, a 44-year-old woman with low back pain and sick leave, a woman 58 years old and another 70 for hypertension control, a 37-year-old woman, who reports that she is “dizzy again”, another 33-year-old woman, pregnant, a 66-year-old man with gout...
And cases related to COVID-19, among which there are three new cases of respiratory infection, and the rest are follow-ups and related problems: A woman of 54 with anxiety; she works in a kitchen and says that there are “several positives people”; asymptomatic, but very worried about being able to infect her husband (he has COPD), a 44-year-old man with a fever of 38º, cough, malaise and general pain, headache, and asthenia; he says that in his work (assembler of metal structures) there are several colleagues with symptoms of COVID-19, but none has been tested, a 62-year-old woman on the 12th day of evolution of COVID-19 (with PCR performed), and presenting with weakness, headache, persistent anosmia, and insomnia; She says that is very ill because cannot sleep; no fever for 5 days; her husband admitted to the hospital for COVID-19 pneumonia, a follow-up of a 31-year-old man with contact with a (theoretical) case of COVID-19 in the work, a 33-year- old man with a bronchial asthma clinic; no fever; despite salbutamol he has wheezing and dyspnea at night. The cases of respiratory infection continue to be considered all of them COVID-19 “possible”, since PCR is not performed. Can there be some criteria that guide COVID-19 diagnostic in respiratory infections when PCR is not done? [19].
The COVID-19 crisis is dominating our lives... I have a cat at home, “Trotsky”. As soon as I get home, he comes to greet me, and then follows me everywhere; more like a dog than a cat! If I catch COVID-19 and I have to isolate myself at home, how will I deal with Trotsky? It it makes me uneasy to know that the CDC recommends that dogs and cats also follow social distancing guidelines [20]. Does that imply that “Trotsky” should be wearing a mask (and gloves...) and keeping distance from other cats...?
April 2
In Spain, with 950 deaths recorded this date is the hardest since the beginning of the crisis. The deceased reached 10,003 and the registered cases, 110,238. However, these have three consecutive days slowing down the rate of increase. In Castilla La Mancha there are 7,682 positive cases and 854 deaths.
Another PCR test from the nurse working with my patient list is also negative. She is practically asymptomatic. She will join work tomorrow. I find the negativity (twice) of the PCR strange given its symptoms and the epidemiological context... But I have to keep in mind that our sense of urgency to do something may shut down the decision-making process prematurely, before exploring reasonable alternatives [21].
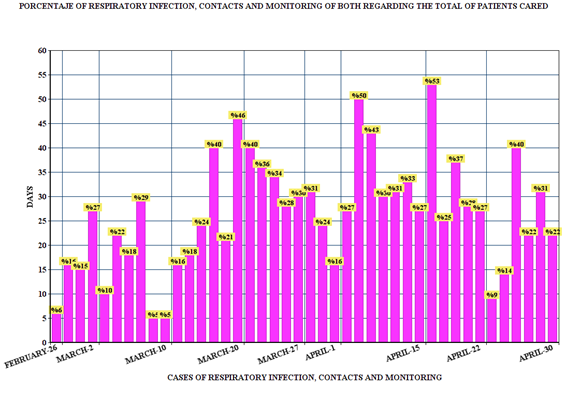
I have 30 patients with telephone consultation (Figure 1). I am seeing patients with an already evolved clinic from previous days, continuations of sick leave also from previous days, and two new cases of respiratory infection:
A 61-year-old man who had been admitted to the hospital 5 days ago has died; He had been seen in the emergency department 15 days ago due to a fever of 38.5ºC and a one-day headache, without respiratory symptoms, with normal chest X-ray and discharged with antibiotic therapy and aerosols; he returned to the emergency room for persistent fever without reaching 39ºC, headache and progressive dyspnea from the previous day, despite treatment. No cases of COVID-19 at home. PCR was positive. His medical record included hypertension, type 2 diabetes, moderate COPD, and obesity. He was on enalapril treatment. Bilateral pneumonia was verified. In its evolution, it became secondary respiratory failure, with desaturation despite a reservoir, tachypnea, nervousness, and in poor general condition. He was evaluated by the ICU, ruling out invasive mechanical ventilation. He was exitus 12 days after the onset of symptoms.
I return home at the end of my day. I am tired and still feel strange, I have to drive 30 km. I see the fields next to the river Tagus full of yellow flowers and the trees of a deep green colour… We are in spring. Life is re-emerging as every year ..., but I do not feel reborn and vital like other springs. It is a strange, oppressive time ... And yet the yellow fields are beautiful ... How satisfied am I to be a doctor working with COVID-19 patients during the pandemic?
April 3
Another extension of the mandatory confinement is announced until April 26 at the moment. There are 8,523 positive cases and 916 deaths in Castilla La Mancha.
At 7 AM my computer does not connect to the internet server! I am lost because I do everything by phone and with the computer... I look at the connections... It was the cable of the telephone disconnected... we used it so much... so; the cable must have been pulled...
There are 20 patients with telephone consultation: a few for reasons not related to COVID-19: phlegmon, dermatitis, anxiety, polyposis nasal, rheumatoid arthritis, plantar fasciitis...
And the majority, with 3 new cases of respiratory infection, they are especially a follow-up of previous cases, and anxiety problems (will the epidemic of COVID-19 be followed by an epidemic of anxiety? [22]; and sick leave related to COVID-19:
A 32-year-old male, nurse, asthmatic, with positive COVID-19 PCR, who continues his sick leave, a 62-year-old woman, with COVID-19 confirmed with PCR, who is better, without cough or fever, but insomnia and night headache;
epigastric pain attributed to treatment with amoxicillin prescribed in the hospital, a 51-year-old woman who is better, although slight cough and nasal congestion persists with anosmia and dysgeusia, a 29-year-old woman, no fever for more than a week, who is well , without cough or dyspnea, a 40-year-old woman, on the 17th day of evolution, who reported symptomatic improvement, afebrile for 4 days, but persisted anosmia, ageusia and myalgias; she is a worker in a nursing home with contact with COVID-19, a 41-year- old man with a slight cough and slight general malaise and headache, a 50-year-old woman with anxiety about COVID-19 due to being working in the administrative area of the hospital, a 24-year-old woman whose co-worker is in isolation on suspicion of COVID-19, a 50-year-old man with a cough and several cases of COVID-19 at work, and a 48-year- old woman who wants a request for an X-ray of chest due to fear of COVID-19 pneumonia, although she is asymptomatic … However, patients may have normal chest radiographs and have COVID-19; Physicians should not reassure patients with normal chest radiography [23].
April 8
In Castilla La Mancha 11,788 positive cases and 1,255 deaths. In Spain: 146,690 infected; 14,555 dead and 48,021 recovered. I receive the data of those affected by COVID-19 confirmed with PCR, in the area of the health center (a neighborhood of 20,000 inhabitants): 98 positive and 6 deceased. On my patient list (2,000 patients): 4 positives. Probably in my patient list there are 20 times more positive, and the same regarding the neighborhood: it could be 2,000. Obviously, all patients with symptoms remain untested, except those who go to the hospital with severe symptoms or are admitted [24].
I have 35 patients with telephone consultation.
There are three new cases of respiratory infection / contact and many follow-ups: a 56-year-old woman who reports being better, no fever for more than 5 days, without dyspnea at any time, although he continues with some cough and myalgia persists, a 38-year-old man on the 14th day of evolution, with persistence of some dry cough, anosmia and ageusia, a woman 62 years old, better of the evolution of COVID-19 who cries... “she is depressed by her husband who remains hospitalized with significant deterioration and cannot go with him .., a 60-year-old man who complains of a headache “for having a cold”..., a 53-year-old man -year-old hospital warden, who asks to be discharged from work, after a cure confirmed with PCR, a 40-year-old woman who says she has been taking care of her mother (who was seen in the hospital’s emergency department) and who has had a low fever for 2 or 3 days, without other symptoms, a 71-year-old woman with odynophagia and myalgia, a male of A 31-year-
old woman who refers to “contact with a case”...
In addition, other queries not directly related to COVID-19: anxiety, hypertension, your dog’s bite, dental pain, possible Bartholino cyst, hypercholesterolemia, dyspepsia… April 14th. After Easter In Castilla La Mancha there are 14,329 positive cases and 1,714 deaths. In Spain 172,655 infected, 18,056 dead and 67,504 recovered.
There have been several holidays for Easter. I have been confined at home following government regulations ... In any case; I know I am lucky... I was able to go out, despite the fact that it rained for several days, to my small patio at home where there are four trees; a fig tree, a palm tree, a cypress and a quince tree... This situation started not long ago, but it seems like a century to me... Yesterday April 13 was the first day of returning to work for non-essential activities in Spain.
The medical partner admitted with COVID-19 who did a “cytokine storm” is better... she could be discharged this week [25].
I have put on a cloth cap and gown, as well as a mask... They pass me a protective gown that I keep for the future...; It is disposable, and I only have that... Although in reality I am not currently treating patients face to face, with some exceptions, and never with respiratory symptoms. I find it difficult to decide the appropriate level of protection and to be able to follow it correctly. “It’s better to be lucky than to do it well” [26].
I speak with the Coordinator of the health center and I thank him for not including me in the respiratory care shift following a precautionary principle according to which older doctors are being reassigned to non-contact tasks with respiratory patients [27]. But, I have doubts for the near future, when face-to-face visits begin, not by phone. Since there may be non-respiratory symptoms as the only manifestation of COVID-19, and asymptomatic and pre- symptomatic can be contagious. I ask about the rules on the protective equipment recommended for the doctor, when attending patients not specifically with the COVID-19 clinic [28, 29, 30, 31].
I receive an email with the list of patients with a positive test result for COVID-19 belonging to my health center, which with updated data as of April 13, 2020, are 113 positive with 8 deceased. Of which 6 are from my surgery, with 2 deceased.
There are 60 patients with telephone consultation. There are many more queries than my average! But I understand that it is partly due to the previous holidays. Among the consultations related to COVID-19, there are 3 new cases of respiratory infection, and follow-up of the previous ones:
A 62-year-old woman with COVID-19 calls me to tell me that her husband of 68 has passed away. He had diabetes mellitus, dyslipidemia, and hypertension; he was not on treatment with Angiotensin-converting – enzyme inhibitors or angiotensin-receptor blockers. For 15 days, she presented dry cough without dyspnea, and loose stools; Right upper lobe pneumonia, with an acceptable initial clinical situation, but he presented frank respiratory deterioration with progression of the pulmonary infiltrate, requiring, after objectifying hyper inflammation data, pulses of corticosteroid therapy, and after persistent respiratory failure, tocilizumab and ventilatory support with BiPAP were inserted and high flow (30 l / min); due to the bad evolution, immunoglobulins and anakinra were inserted, with a bad final evolution, dying; he had been repeatedly evaluated by the ICU that rejected his admission.
In addition, I mainly attend follow-ups of possible COVID-19 that started days ago, and three new cases. Men present more biological pathology, but women (caregivers of their children, the elderly and the rest of the family, and also frequently social-health workers) will present greater and more lasting psychosocial problems [32].
I make a face-to-face consultation: a 35-year-old man with dermophicosis of the beard. In addition, other non-COVID-19 consultations by phone: various allergic rhinitis, hearing loss and occasional dizziness, cystitis, anxiety, hypothyroidism, urinary incontinence, dermatitis, insomnia... It has been a hard day. The sky is covered with black clouds and a light rain falls as I drive home… but on the green and yellow expanses of the fields, precious patches of red poppies are appearing.
April 20th
There are 16,796 positives and 2,021 deceased in Castilla La Mancha. The same level of increase is not being seen in the cases that existed previously. In Spain, the death toll drops to 399. I receive the list of patients with a positive test result for COVID-19 from the health center: 126 positives (out of 20,000 inhabitants: 1%), and 8 deaths (8 out of 126 positive tests: 6%). In my consultation 6 positives (out of 2000 patients: 0.3%), and 2 deceased -two males- (out of 6 positives: 33%).
Three doctors have died in 24 hours in Castilla-La Mancha. The nurse on the afternoon shift, who went back to work without having had a PCR before, will not come today; the PCR came back positive and now she is told to remain in isolation at home for five weeks waiting for her COVID-19
test to turn negative to return to work. We still do not know almost anything about immunity [33].
Despite everything, my colleagues and I asked the Directorate to do the test [34]. But I understand the complex context of the tests, including the problem of their validity, but the truth is that the fact that we still do not do diagnostic tests for possible cases, confuses the diagnosis and alters the true incidence rate [35, 36, 37, 38, 39, 40].
I attend 40 patients (by phone). I don’t see any new case of respiratory infection. I am not seeing for days the same level of increase in cases that I had seen previously. Many calls are for follow-up and continuations of work sick leave by COVID-19:
A 40-year-old woman who has been in quarantine due to contact with possible COVID-19 for 15 days, and who “as it is being observed more ... takes her temperature 3 times a day and has 37.3ºC, and spent 2 days with throat discomfort, and then 2 days with loose stools ..., another woman who takes discharge from work after being asymptomatic (presented fever, cough and diarrhea), a 34-year-old woman who also takes discharge from work after being asymptomatic, another 31-year-old woman also discharged, who says that “she is like a rose,” several phone calls to monitor her progress and maintain her sick leave: 6 due to anxiety over COVID-19...
And a few other calls were for reasons not related to COVID-19: a 53-year-old woman recently diagnosed with Hodking lymphoma, an 80-year-old woman with low back pain and paresthesias in the hands and feet, a continuation of sick leave in a woman pregnant, toothache, hypertension...
April, the 21st
Castilla-La Mancha registered the first positive case for coronavirus on March 1 and the first died on 12 of that same month. Today, it faces 17,045 positive cases “detected” and 2,075 deceased “registered”. Lack of diagnostic tests remains the fundamental problem in a crisis that is improving in health centers. However, the nursing homes, with 750 deaths, have entered an escalation that does not stop, since the positives are 3,960 in 218 centers [17].
Perhaps, the difference is that the cases at the beginning of the outbreak were mainly respiratory presentations (and to a lesser extent digestive), but now non-typical or non- respiratory presentations appear [41].
I have 39 telephone inquiries.
Some queries for problems other than COVID-19: Insomnia, tension headache, low back pain, miscarriage, dental pain, vasovagal syncope, a burn when making fritter...
Two consultations for new respiratory infections: A 69-year-old man with a slight cough with expectoration (and a history of COPD), and a 31-year-old man who spent a couple of days with deep cough and dyspnea, was now better (Should patients have a pulse oximeter at home to identify patients who deteriorate earlier?) [42].
And most of them were follow-ups of cases of respiratory infections with and without PCR done, and contacts with proven or possible cases: A 54-year-old woman in follow-up for anxiety due to COVID-19 and on sick leave, a 40-year- old man on his 29th day of evolution, who presented pneumonia with undetectable PCR, and still reports asthenia in convalescence, a 32-year-old man on the 18th day from symptoms onset that he is asymptomatic, another 44-year- old man with 21 days of onset, who presented dyspnea with minimal effort, but reported improvement over previous days, a 53-year-old man on day 20 from the onset of symptoms, with a dry cough and slight diarrhea, a 60-year-old man with a positive COVID-19 PCR, and who continues to have a headache with a cough, a 41-year-old COVID-19 woman who was asymptomatic, another 62-year-old woman also COVID- 19 positive with grief due to the death of her husband in the hospital due to COVID-19, a 40-year-old man with 14 days of evolution and only with ageusia and anosmia; she works in a nursing home, a 55-year-old woman who presented a clinic compatible with COVID-19 for 1 month, asymptomatic, another 26-year-old woman who is asymptomatic on her 17th day of evolution, and who was treated with azithromycin... (Throughout the world, therapeutic management of SARS- CoV-2 has been largely supportive, and to date, no specific therapy has been scientifically proven to reduce mortality) [21].
April 24
In Spain, the daily deceased drop to 367, the lowest number in a long time. The contagion figures remain at 2%, but a month ago we were at 35%. In Spain, more than 34,000 health personnel have been infected (more than 16% of all infections). In Castilla La Mancha: 18,053 positives and 2,255 deaths (832 in nursing homes) [17].
I have 29 patients with telephone consultations. With a new case of respiratory infection, follow-up of previous cases and problems and sick leave related to COVID-19. Perhaps, the difference is that the cases at the beginning of the outbreak were mainly respiratory presentations (and to a lesser extent digestive), but now non-typical or non- respiratory presentations appear [41]:
A follow-up of a 45-year-old man on day 31 of evolution who still reports headache, and comments that he had skin lesions on the hands that he describes as “between blisters and chilblains” of 1-2 weeks of evolution [43].
And to a lesser extent, other problems not related to COVID-19: rhinoconjunctivitis-asthma, hypertension, dental pain, type 2 diabetes...
April 27
There are 19,286 positives and 2,365 deceased in Castilla La Mancha. The Spanish Health Authority has changed its criteria several times in its reports. In any case, the evolution is clearly downward and gives us hope. But although the virus recedes, there are still infections and we do not know where [44].
I have 30 patients for telephone consultation. On many occasions, in addition to those who make an appointment, many patients call me directly (sometimes several times a day!): cystitis, arthritis, arthralgia, malleolar edema, plantar fasciitis, allergic rhiniconjunctivitis, control for prostate cancer, hypertension, low back pain, nail dystrophy, type 2 diabetes...
I have 4 patients with anxiety related to COVID-19, for fear of returning to work.
There is a new case of respiratory infection and 9 patients in follow-up contact who are still asymptomatic (one of them says: “what worries him most is not having a job”; another patient says that she cannot be in isolation because she has her three children with her”).
I have several patients requesting a test for COVID-19. And again, possible cases of COVID-19 with unusual symptoms [41]:
- A 38-year-old man with hip pain after presenting dry cough, ageusia and anosmia in mid-April.
- A 36-year-old man with swollen interphalangeal joints of hands with itching or slight pain on movement, from a couple of days coinciding with a slight cough (arthritis, dermatitis?).
- A 46-year-old woman with an itchy papule-vesicular rash that left crusts on the external aspect of the ankle, anterior region of both legs and anterior aspect of the foot, reappearance of light cough with occasional expectoration and low-grade fever (Initially she presented cough, anosmia, fever with a maximum number of 37ºC); she says that the disease “goes in stages ... at first cough ... then general pain like the flu but less cough and without fever ... and now the skin ...” (she has a brother with COVID-19 pneumonia). This patient seems to be right: COVID-19 is a much longer disease, with ups and downs, compared to the typical cold or flu [45].
And some case of confusion in the diagnosis: a 44-year- old woman, with difficulties with the Spanish language, who started 20 days ago with a fever of 38º, was considered COVID-19, but after the appearance of abdominal pain, and the chest X-ray normal, an abdominal pelvic CT scan showed uncomplicated acute colonic diverticulitis.
April 29
In Spain 2,144 infected more. The rate of new infections up to 1% from 0.6% recorded yesterday. In Castilla La Mancha 277 confirmed new infections [46].
I have 16 patients. The volume of the clinic has dropped significantly. All inquiries are by phone. There is no new case of respiratory infection. The consultations are follow-up and many to give the medical “discharge”.
Some patient whose non-COVID-19 diagnosis and treatment had been delayed or paralyzed [47], already resumed: A 63-year-old woman who received first cycle of chemotherapy for newly diagnosed Hodgkin lymphoma during the “COVID-19 times”, and is doing very well, without fever.
And they begin to become more frequent than consultations on other topics no-COVID-19; a 63-year- old man with ulcerative colitis, an 81-year-old woman with chronic atrial fibrillation, a 45-year-old woman with decompensated autoimmune primary hyperthyroidism “due to all the stress of COVID-19”, a 35-year-old man years with sleep apneas, warfarin controls ...
But I still do not know the true incidence of the epidemic, which is possibly more widespread than current data suggested [48].
Conclusion
The decisions were made in Spain late, perhaps thinking that COVID-19 would not affect us, but the epidemic advanced more than expected and the health system exploded. In the family medicine consultation, the usual organizational guidelines have been modified, maintaining an initial triage and telephone consultations for almost all patients. It is seen that, during the month of April 2020, there is: 1) a reduction in new COVID-19 cases, but without disappearing; 2) an increase in consultations to follow up verified and possible cases, verified or possible contacts, and work leave related to these cases; 3) Rare non-respiratory symptoms and consequences of COVID-19 are beginning to be seen (dermatological symptoms, arthritis, truncated mourning’s, anxiety, financial and social problems); 4) maintenance of large number of consultations for anxiety secondary to COVID-19; and 5) a practically total paralysis of important new diagnoses other than COVID-19 (in the period from the first of March to the end of April, there is only one important diagnosis other than COVID-19 was done: a Hodgkin lymphoma whose diagnosis and treatment were delayed; no diagnostic tests were performed, nor were there any other new cases of any other major disease.
Anyway, some good news and hope by the end: the epidemic shows clear reductions in new cases, and it must be remembered that the human being has survived over the years in difficult situations which have always been a vector of impulse in the birth of large companies that knew how to find new ideas and opportunities. COVID-19 is probably a huge opportunity for hope and improvement.
References
-
Gannik DE (1995) Situational disease. Fam Pract 12(2): 202-206.
-
Turabian JL , Perez Franco B (2001) Actividades Comunitarias en Medicina de Familia y Atención Primaria. [Community Activities in Family Medicine and Primary Care]. Madrid: Díaz de Santos.
-
Turabian JL, Perez FB (2016) The Family Doctors: Images and Metaphors of the Family Doctor to Learn Family Medicine. New York. Nova Publishers
-
Turabian JL (1995) Cuadernos de Medicina de Familia y Comunitaria. Una introducción a los principios de Medicina de Familia. Notebooks of Family and Community Medicine. An introduction to the principles of Family Medicine. Madrid: Díaz de Santos.
-
Valverde Obando LA (1991) The field daily. Revista Trabajo Social.
-
University of Southern California (2020) Organizing Your Social Sciences Research Paper. Writing Field Notes.
-
WHO (2020) The Global Outbreak Alert and Response Network (GOARN) marks its 20th anniversary.
-
Kim JY, Choe PG, Oh Y, Oh KJ, Kim J, et al. (2020) The first case of 2019 novel coronavirus pneumonia imported into Korea from Wuhan, China: implication for infection prevention and control measures. J Korean Med Sci 35(5): 61.
-
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA.
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
Xiong Y, Peng L (2020) Focusing on health-care providers’ experiences in the COVID-19 crisis. Lancet Glob Health.
-
Liu Q, Luo D, Haase JE, Guo Q, Wang XQ, et al. (2020) The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Health.
-
Aviv R, Baird RP, Bilger B, et al. (2020) Twenty-four hours at the epicenter of the pandemic. The New Yorker.
-
Turabian JL (2020) A family doctor’s clinical- epidemiological diary in spain of the times of COVID-19. CHAPTER 1. February 24 to March 15: is COVID-19 a lottery?. Epidemol Int J.
-
Turabian JL (2020) A family doctor’s clinical- epidemiological diary in spain of the times of COVID-19. CHAPTER 2. MARCH 16-31: The Big Bang. Epidemol Int J.
-
Ospina DP (2016) El diario como estrategia didáctica. Universidad de Anrioquia.
-
Turabian JL (2020) The epidemiological hypothesis of “the Trojan Horse”: were hospitals the main vectors of the exponencial beginning of coronavirus disease 2019 (COVID-19) in Spain and other Countries? Epidemol Int J.
-
Güell O (2020) Spain is the country with the most infections among healthcare personnel. El País.
-
Turabian JL (2020) Clinical-Epidemiological Characteristics That May Help the General Practitioner to Consider Covid-19 Diagnosis in Acute Respiratory Infections When Diagnostic Tests Are Not Accessible. Epidemol Int J 4(2): 000143.
-
CDC (2020) Confirmation of COVID-19 in Two Pet Cats in New York.
-
Zagury OI, Schwartzstein RM (2020) Covid-19- A Reminder to Reason. N Engl J Med.
-
Turabian JL (2020) Implications on mental health by the coronavirus disease 2019 (COVID-19) pandemic: The role of general practitioner. Archives of Psychiatry and Mental Health.
-
Lewis R (2020) Normal Chest X-ray Doesn’t Rule Out COVID-19. Medscape.
-
Turabian JL (2020) Micro-Impact of the Pandemic by Covid-19 in the General Medicine: Clinical and Epidemiological Reflections from the Situation in Spain March 2020. Epidemol Int J 4(2): 000141.
-
Jose RJ, Manuel A (2020) COVID-19 cytokine storm: the interplay between inflammation and coagulation. Lancet Respiratory Medicine.
-
Ouyang H (2020) I’m an E.R. Doctor in New York. None of Us Will Ever Be the Same. A Covid diary: This is what I saw as the pandemic engulfed our hospitals. The New York Times.
-
Salisbury H (2020) Who is vulnerable? BMJ 369: m1572.
-
WHO (2020) Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages: Interim guidance.
-
McCarthy M, Rivolta G. (2020) Covid-19: If we can’t protect our workers, we can’t protect our patients. BMJ Opinion.
-
Robertson JFR, Stewart M, Kendrick D, Sewell HF (2020) Covid-19: Protect health and social care workers and refer their deaths to the coroner. BMJ.
-
Gandhi RT, Lynch JB, del Rio C (2020) Mild or Moderate Covid-19.
-
Turabian JL (2020) Sex and gender biopsychosocial differences in coronavirus disease 2019 (COVID-19): men have more biological problems, but women suffer more long-term serious psychosocial consequences and with more implications for population. Journal of Women’s Health Care.
-
Johnson K (2020) COVID-19 antibody tests proliferate: what do they show?. Medscape.
-
Angell SY (2020) State of California- Health and Human Services Agency California Department of Public Health.
-
Editorial (2020) COVID-19: endgames. The Lancet Infect Dis 20(5): 511.
-
US Food and Drug (2020) Important Information on the Use of Serological (Antibody) Tests for COVID-19- Letter to Health Care Providers.
-
Offord C (2020) How (Not) to Do an Antibody Survey for SARS-CoV-2. The Scientist.
-
Mallapaty S (2020) Will antibody tests for the coronavirus really change everything? Nature.
-
Paakkari L, Okan O (2020) COVID-19: health literacy is an underestimated problem. Lancet Public Health.
-
Zimmer K (2020) What Do Antibody Tests For SARS- CoV-2 Tell Us About Immunity? The Scientist.
-
Otto MA (2020) Unusual Presentations of COVID-19: Our Ignorance Is Profound. Medscape.
-
Johnson K (2020) COVID-19: Home Pulse Oximetry Could Be Game Changer, Says ER Doc. Medscape.
-
Casas CG, Català A, Hernández GC, Jiménez PR, Nieto DF, et al. (2020) Classification of the cutaneous manifestations of COVID‐19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol.
-
Linde P (2020) More than 114,000 people have been hospitalized in Spain for the coronavirus. El País.
-
Scudder L (2020) After Battling Flint Water Crisis, Pediatrician Faces a Fight With COVID-19. Medscape.
-
Consejería de Sanidad de Castilla La Mancha.
-
Cotelo J (2020) COVID-19 forces a paradigm shift in the management of breast cancer. Medscape.
-
Crist C (2020) WebMD Poll: 93% With COVID-19 Symptoms Didn’t Get Test. Medscape.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria