A Longitudinal Study of SARS-CoV-2 Secondary Infection Risks in Family Members: Psychosocial Factors May be More Important than Biological Ones
Background: The factors of why some people get SARS-CoV-2 and others do not, after a primary case in families remains questionable. Objective: To analyze some of the possible risk factors for contracting COVID-19 within families after there is a primary case. Methodology: An observational, longitudinal and prospective study to analyze data of variables considered possible risk factors collected of 132 people in 39 families with at least one polymerase chain reaction (PCR) confirmed COVID-19 primary case, was conducted from March 15 to December 15, 2020, in a center of general medicine in Toledo (Spain). The Relative Risk (Incidence among the exposed population / Incidence among the population not exposed) for possible risk factors as predictors of secondary transmission were calculated. Results: 39 families with 92 people were included with a primary case, of which 70 were sick (PCR positive) and 22 were healthy (PCR negative and asymptomatic). Age
Introduction
The proportion of risk factors for transmission and community spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), among household and non- household contacts remains unclear. Carriers of SARS-CoV-2 occurred more frequently in middle-aged people who had close contact with infected relatives [1]. About half of adults with coronavirus disease 2019 (COVID-19) report they had no known close contact with an infected individual in the 2 weeks prior to their illness; among those who reported close contact with an infected person, that person was most often (45% of cases) a family member [2].
Household members who are older, have underlying medical conditions, or share a bed or vehicle with the index case appear to be the most susceptible to infection [3, 4, 5]. Children are probably less at risk of becoming infected [6]. However, your stool samples and nasopharyngeal swabs may remain positive for SARS-CoV-2 for more than two weeks after resolution of symptoms, although its role in transmission has not yet been established [7].
The number of people infected with COVID-19 receiving treatment at home is increasing every day. On many occasions, despite the fact that they must be hospitalized, due to the impossibility of ensuring the care of children, infected parents are receiving medical treatment at home [8]. Taken together, it can be said that currently the transmission of COVID-19 within families and close contacts accounts for most of the epidemic growth [9]. In China, more than 70% of person-to-person transmission of SARS-CoV-2 occurred in families. Household transmission in the presymptomatic or early symptomatic period of COVID-19 is a driver of epidemic growth and any measure aimed at reducing this can flatten the curve [9].
Decisions on the continued need for control measures to contain the spread of SARS-CoV-2 are based on information about the number of people who test positive for SARS- CoV-2 and factors of individual risk. But surveillance systems generally are not based on family samples and are not longitudinal in design. Furthermore, important questions remain about home transmission. Research should be conducted to identify the determinants of transmission in the home and the optimal strategies to isolate cases and protect household contacts. These strategies will be particularly important for those most at risk of adverse outcomes, including ethnic minority communities, people from low-income households, and those living in urban areas with overcrowded housing [10].
In this context, this article which is part of a set of research studies on COVID-19 in families, aims to study secondary cases in families to looking for some information on why some people have COVID-19 and others remain healthy after a primary case. In this way, some of the possible risk factors for contracting COVID-19 were studied within families, after there is a primary case, and these variables are compared between secondary cases (polymerase chain reaction [PCR] positive) and non-diseased cases (PCR negative and asymptomatic), calculating relative risks (RR).
Materials and Methods
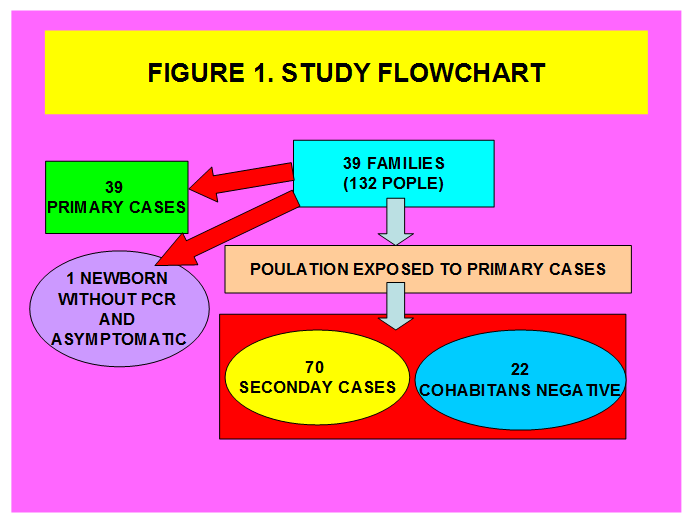
An observational, longitudinal and prospective that analyzes data of variables considered possible risk factors collected of 132 people in 39 families with at least one PCR confirmed COVID-19 case, was conducted from March 15 to December 15, 2020, in a general medicine office in Toledo, Spain. PCR was performed on all family contacts/cohabiting after a primary case was declared in the family. The data was accumulated as part of a set of studies in 39 families with COVID-19, and in part the methodology has already been published [11].
Diagnosis of COVID-19
The diagnosis was confirmed with PCR oropharyngeal. The cases included symptomatic cases and asymptomatic carriers. Information on COVID-19 patients and their contacts was registered in the system used by medical services in the consultation and a progressive follow-up was carried out until the end of the study.
Diagnosis of Healthy Partners
Healthy partners were defined as such by presenting a negative PCR and being asymptomatic.
Outcome of Interest
The outcome of interest was to study some of the possible risk factors for contracting COVID-19 within families, after there is a primary case, seeking information on why some people have disease and others remain healthy. In this sense, the variables collected were compared by calculating the RR as the Incidence among the exposed population / Incidence among the population not exposed to possible risk factors, in the sick (positive PCR) and non-ill (negative PCR).
The RR assumes the strength of the association; The RR expresses to the clinician the excess risk that a patient has for being exposed to the risk factor, and also serves to identify people at high risk, but does not measure the probability that someone with the risk factors will acquire the disease. The RR was interpreted as follows [12]:
- From 0 to 0.5: effective protection factor
- From 0.6.0.8: certain benefit
- From 0.9 to 1.1: not significant
- From 1.2 to 1.6: weak risk
- From 1.7 to 2.5: moderate risk
- Greater than 2.5: strong risk
Household Contacts
Household contacts were defined as people who shared a residence with the COVID-19 index case. We defined family members as those who had lived with primary cases in a house 4 days before and for more than 24 hours after the primary cases developed illness related to COVID-19. Families with secondary transmission were defined as those where some or all of the family members become infected within one incubation period (2 weeks) of symptom onset of the primary case. The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [13]. Contacts were quarantined shortly after the index case was diagnosed, thereby reducing the risk of transmission (a provision not available in all circumstances).
Collected Variables
Data on the index case and close contacts were extracted from the medical records of the general medicine practice under study. For the family members of the primary case the following variables were collected: age, sex, chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non-reversible pathological alteration, requires special training of the patient for rehabilitation, and/or can be expected to require a long period of control, observation or treatment” [14, 15, 16], classified according to the International Statistical Classification of Diseases and Health -Related Problems, CD-10 Version: 2019 [17], social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [18, 19], summarizing their groups in two: skilled and unskilled workers, students , problems in the family context and low income household based on the genogram and in the experience of the general practitioner for their continuity of care and knowledge of the family (genogram is a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that “complex” genograms present families with psychosocial problems) [20, 21, 22, 23, 24], belonging to an ethnic minority, and the number of family members.
For the primary cases, the following variables were collected: presence of symptoms (only cough and diarrhea, as they are symptoms of greater risk of infection) or being asymptomatic, and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate≥30 breaths/ min; pulse oxygen saturation ≤ 93% with room air at rest; arterial partial pressure of oxygen/oxygen concentration ≤ 300 mmHg); to simplify comparison, moderate and severe cases were counted together.
Sample
A convenience sampling was used. The families participating in the study were chosen because they had their members in the same consultation and all medical information was available.
Sample Size
Sample size was calculated for cohort studies, with a two-sided confidence level (1-alpha) of 95, a power (% probability of detection) of 80, a ratio of controls per case of 3, a hypothetical proportion of cases with 40% exposure and a hypothetical proportion of controls with 10% exposure. These parameters give a sample of 68 individuals, 17 cases and 51 controls (Kelsey) [25].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test when necessary, for percentages (according to the number the expected cell totals), and the Student t test for the mean.
Results
39 families with 132 cohabitants were included, whose members were seen in the same consultation and all medical information was available. Family size was 3.38 + -0.96 members (arithmetic mean + -standard deviation). There were 92 family members, of which 22 had negative PCR (22/92 = 24%), one newborn who did not have PCR and was asymptomatic, and 70 secondary cases with positive PCR (Figure 1). The age in years (arithmetic mean and standard deviation) and the range was 38.89 + -15.41 (Range: 12- 67) in the patients, and 32.45 + - 20.93 (Range: 1-89) in the healthy ones (t = 1.68266. p = .047679. Significant at p <.05).
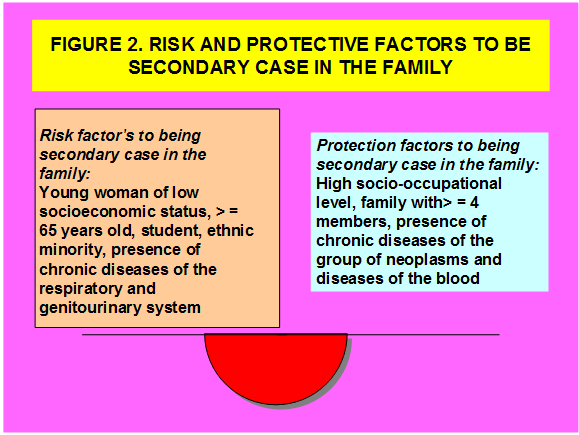
The comparison between the variables studied and their Relative Risk (RR) in cases and non-cases are presented in Tables 1-3. The following risk factors for secondary infection were found in families: Age <45 years, being a woman and being a member of a low-income household, were the only variables that showed a weak and statistically significant risk; Age>65 years, being a student, being an ethnic minority, the presence of chronic diseases of the Respiratory system and Genitourinary, also showed a weak risk, but not statistically significant. The high socio-occupational level was a protective factor and statistically significant against secondary contagion in families. The larger family size (Family with> = 4 members) was a factor of certain protective benefit but not statistically significant. The presence of chronic diseases of the Neoplasm group showed some protective benefit, and the diseases of the blood were an effective protection factor, but the latter two were without statistical significance. Regarding the characteristics of the primary case, the presence of cough and being asymptomatic were factors of certain protective benefit to become a secondary case in the family, but without statistical significance (Figure 2).
| Positive Secondary Cases (Sick; N = 70) | Negative Partners in Families (Healthy) (N=22) | Statistical Significance | Relative Risk (Rr) | |
|---|---|---|---|---|
| -Woman | 51 (73) | 9 (41) | X2= 7.5318. p= .006062. Significant at p < .05. | 1.4 (CI 95%: 1.08, 1.89); Weak risk |
| > = 65 years | 6 (9) | 0 | Fisher exact test = 0.3296. NS | 1.3 (CI 95%: 0.72, 2.48); Weak risk |
| < 45 years | 52 (74) | 10 (45) | X2= 6.3317. p= .01186. Significant at p < .05. | 1.4 (CI 95%: 1.05, 1.87); Weak risk |
| -Workers with some type of specialization | 20 (29) | 20 (91) | x2= 12.1205. p= .000499. Significant at p < .05 | 0.5 (CI 95%: 0.79, 0.37); Effective protection factor |
| -Students | 27 (39) | 4 (18) | X2= 3.1148. NS | 1.2 (CI 95%: 0.94, 1.64); Weak risk |
| -Ethnic minority | 23 (33) | 4 (18) | X2= 1.7386. NS | 1.2 (CI 95%: 0.87, 1.61); Weak risk |
| -Low income household | 23 (33) | 2 (9) | X2= 4.7777. p= .028831. Significant at p < .05. | 1.3 (CI 95%: 0.99, 1.73); Weak risk |
| -Complex family | 12 (17) | 3 (14) | X2 with Yates correction= 0.0033. NS | 1.1 (CI 95: 0.16, 7.11); Not significant |
| -Family with > = 4 members | 38 | 17 | X2= 3.6788. NS | 0.8 (CI 95%: 1.04, 0.62); Certain protective benefit |
| -Presence of chronic diseases | 24 (34) | 8 (36) | X2= 0.0319. NS | 1 (CI 95%: 1.61, 0.6); Not significant |
Table 1: ** Comparison of the Variables Studied Between Positive Secondary Cases (Sick; N = 70) and Negative Partners in Families
( ): Denotes percentages of total in patients (positive PCR) and in healthy (negative PCR and asymptomatic) NS: Not significant at p< .05. CI: Confidence Interval Table 1: Comparison of the Variables Studied Between Positive Secondary Cases (Sick; N = 70) and Negative Partners in Families (Healthy; N = 22).
| Positive Secondary Cases (Patients) (N=70) | Negative Partners (Healthy) (N=22) | Statistical Significance | Relative Risk (RR) | |
|---|---|---|---|---|
| -II Neoplasms | 1 (1) | 1 (7) | Fisher exact test = 0.3176. NS | 0.6 (CI 95%: 18.95, 0.02); Certain protective benefit |
| -III Diseases of the blood | 0 | 1 (7) | Fisher exact test= 0.1728. NS | 0 (CI 95%: Infinity, 0); Effective protection factor |
| -IV Endocrine | 21 (31) | 2 (14) | X2 with Yates correction= 0.9244. NS | 1.1 (CI 95%: 0.86, 1.53); Not significant |
| -V Mental | 10 (15) | 3 (22) | Fisher exact test statistic= 0.6885. NS | 0.9 (CI 95%: 2.08, 0.41); Not significant |
| -VI-VIII Nervous and Senses | 6 (9) | 2 (14) | Fisher exact test = 0.6215. NS. | 0.9 (CI 95%: 5.03, 0.16); Not significant |
| -IX Circulatory system | 5 (8) | 1 (7) | Fisher exact test = 1. NS | 1 (CI 95%: 0.97, 1.05); Not significant |
| -X Respiratory system | 3 (5) | 0 | Fisher exact test = 1. NS | 1.2 (CI 95%: 0, Infinity); Weak risk |
| -XI Digestive system | 5 (7) | 1 (7) | Fisher exact test = 1. NS | 1 (CI 95%: 1.99, 0.41); Not significant |
| -XII Diseases of the skin | 3 (5) | 1 (7) | Fisher exact test = 0.5393. NS | 0.9 (CI 95%: 1.99, 0.41); Not significant |
| -XIII Musculo-skeletal | 8 (12) | 2 (15) | Fisher exact test = 0.6813. NS | 1 (CI 95%: 1.43, 0.64); Not significant |
| -XIV Genitourinary | 5 (7) | 0 | Fisher exact test = 0.5812. NS. | 1.2 (CI 95%: 0.49, 3.09); Weak risk |
| TOTAL*= | 67*(100) | 14*(100) | - | - |
Table 2: ** Comparison of Chronic Diseases between Cohabitants with Positive Secondary Cases (Sick; N = 70) and Negative Cohabita
( ): Denotes percentages of total in patients (positive PCR) and in healthy (negative PCR and asymptomatic) *Patients could have more than one chronic disease. The percentages are over the total of chronic disease NS: Not significant at p< .05. CI: Confidence interval Table 2: Comparison of Chronic Diseases between Cohabitants with Positive Secondary Cases (Sick; N = 70) and Negative Cohabitants (Healthy; N = 22) In Families.
| Positive Secondary Cases (Patients) (N= 70) | Negative Partners (Healthy) (N=22) | Statistical Significance | Relative Risk (RR) | |
|---|---|---|---|---|
| -Cough | 40 (57) | 17 (77) | X2= 2.8777. NS | RR=0.8 (CI 95%: 1.07, 0.63); Certain protective benefit |
| -Diarrhea | 4 (6) | 2 (9) | Fisher exact test= 0.6266. NS | RR=0.9 (CI 95%: 1.24, 0.74); Not significant |
| -With gravity | 15 (21) | 5 (23) | X2 with Yates correction= 0.028. NS | RR= 0.9 (CI 95%: 1.24, 0.78); Not significant |
| -Asymptomatic | 7 (10) | 4 (18) | Fisher exact test= 0.4501. NS. | RR=0.8 (CI 95%: 1.48, 0.45); Certain protective benefit |
Table 3: ** Comparison of Characteristics of Primary Cases In Secondary Cases (Sick; N = 70) and Negative Cohabitants (Healthy; N
( ): Denotes percentages of total in patients (positive PCR) and in healthy (negative PCR and asymptomatic) NS: Not significant at p< .05. CI: Confidence interval Table 3: Comparison of Characteristics of Primary Cases In Secondary Cases (Sick; N = 70) and Negative Cohabitants (Healthy; N = 22) In Families.
Discussion
Most people with COVID-19 receive care at home, increasing the likelihood of exposure for household members; however, less attention has been paid to family members [26]. Sometimes COVID-19 feels like a game of chance; like Russian roulette [27]. There are numerous reports where very close cohabitants with similar characteristics, including twin brothers with the same body mass index and cardiovascular risk, who work and live together, who share dietary habits, who would have been infected with SARS- CoV-2 from the same person, who had the same viral load at diagnosis and who were treated by the same doctors, had a very different evolution of the disease [28]. The reasons for the different clinical paths are a mystery. Additional research (genetic, epigenetic, metabolic, immunological, and microbiological) is expected to improve understanding of the pathophysiological mechanisms of COVID-19. In addition, there are several reasons why risk factors can vary over time; the behavior and contact patterns of subgroups change over time; adherence to prevention measures may decrease more over time among subgroups with a low risk of hospital admission and death related to COVID-19, than among those who are more vulnerable; and subgroups of people who have been disproportionately affected in a first wave of SARS- CoV-2 infection may have acquired sufficient immunity [29].
Factors beyond Genetic Variants that Contribute to COVID-19
One line of study is the search for genes that could explain why some people are victims of coronavirus infection, while others escape relatively unscathed or have few or no symptoms [30]. Previous research has discovered genetic variants that can alter a person’s chances of contracting an infectious disease. The most famous example is a mutation in the CCR5 gene, which offers protection against HIV. It has also been shown that variants in the human leukocyte antigen genes, which influence the body’s immune response, may explain why some people spontaneously clear hepatitis C infection, while others remain chronically ill [31, 32]. Variants of five key genes responsible for antiviral immunity and lung inflammation have been found to be associated with severe COVID-19. While there is no guarantee that when a gene is found, targeting that gene will result in therapeutic efficacy. What genetic studies do is help to finding very specific starting points for further research. There are likely many other factors beyond these genetic variants that contribute to the severity of COVID-19 disease. Part of the answer is in the genes, but it is unlikely that a single element is completely responsible for the development of COVID-19. It is more likely to be a combination of factors, which can include genetics and age, obesity, gender, and other characteristics [33].
Superpropagation Events: The Importance of Biopsychosocial Factors
A “superspreader” refers to an unusually contagious organism infected with a disease. There is growing evidence that SARS-CoV2 has substantial transmission heterogeneity and that super-spread events have driven much of the local epidemics with consequent implications for mitigation strategies. The factors that contribute to overpredation are not fully understood and are probably multiple [34], including biological factors (characteristics possibly related to viral load), behavioral and social factors (certain people have a large number of contacts in relation to the general population), hazardous facilities (for example, confined spaces with poor ventilation), and what are called “opportunistic” situations (large events with many contacts), or temporary increases in transmissibility (such as occurs when speaking or singing in voice aloud). It has been considered that 70% of those infected do not infect anyone and 20% infect a single person, so only 10% participate in the epidemic process and transmit SARS-CoV-2 to several people [35, 36].
In one study, analyzing contact tracing data from 1,038 laboratory-confirmed cases of SARS-CoV-2 infection in Hong Kong between January and April 2020, the authors estimated that 80% of cases were seeded by only 19% of infected people; on the contrary, most of the patients failed to infect even one other person. Most of the contactor-infected transmission pairs identified (92 of 169) involved household contacts [37]. Thus, preliminary evidence points to SARS- CoV2 over-spread events that occur predominantly in closed environments with poor ventilation where people are very compact and exposed for prolonged periods, particularly with face-to-face contact (> 10 minutes) [38].
Age
Although the elderly are more likely to suffer serious complications, thousands of young and previously healthy people have died from the disease [32]. Young adults, particularly those 17 to 24 years old, were a major early driver of the rise in positivity rates in the second wave. For example, the estimated percentage of people who tested positive was more than six times higher in those aged 17 to 24 than in those aged 70 and over at the end of September 2020 [29]. Older people (≥60 years) have been reported to be the most susceptible to domestic transmission of SARS- CoV-2. Compared with the older group (≥60 years), the risk of infection at home was reported to be lower in the younger group (<20 years) and among adults aged 20 to 59 years [4]. Likewise, slightly greater differences in susceptibility have been reported between older (≥60 years) and younger contacts [39].
We also found that the mean age of the sick (secondary cases) at home was higher than in the non-sick (negative PCR) (38.89 + -15.41 in the sick, and 32.45 + - 20.93 in healthy ones; t = 1.68266. P <.05). Being > = 65 years old was shown to be a weak risk (RR = 1.3; 95% CI: 0.72, 2.48; NS.). But being <45 years of age also represented a weak risk of being a secondary case in families (RR = 1.4; 95% CI: 1.05, 1.87; X2 = 6.3317. P <.05).
Sex
Female contacts have been reported to be slightly more susceptible than male contacts [39]. On average, women tend to have milder disease than men. Men are more likely to have serious complications [32]. Women also face a greater burden of chores and care at home [40, 41]. In our study, being a woman represented a weak risk of being a secondary patient in the family (RR=1.4; 95% CI: 1.08, 1.89; p<.05).
Chronic Diseases
Although people with pre-existing conditions like heart disease are more likely to suffer serious complications, previously healthy people have died from the disease [32]. In a study in China, thirty percent of those who died had no comorbidities at all [42]. Regarding certain specific chronic diseases, asthma per se does not increase risk, perhaps because patients do not express substantial amounts of angiotensin-converting enzyme receptor 2 (coronavirus gateway); instead, there is growing evidence that patients with chronic obstructive pulmonary disease are at a moderately higher risk of a severe course of COVID-19, as are those with pulmonary fibrosis.
People who are obese or suffering from diabetes are particularly susceptible to severe cases of COVID-19 [43]. Diabetes may be an independent risk factor for the rapid progression and poor prognosis of COVID-19 through several known pathways and a possible new one: direct damage to the pancreatic islets [44, 45]. We did not find that the presence of chronic diseases in general showed a significant RR to become a secondary case in families. The presence of chronic diseases of the Respiratory system (RR = 1.2; 95% CI: 0, Infinity) and Genitourinary (RR = 1.2; 95% CI: 0.49, 3.09), showed a weak risk, but not statistically significant. And the presence of chronic diseases of the Neoplasm group showed a certain protective benefit (0.6 (95% CI: 18.95, 0.02), and the diseases of the blood being an effective protection factor (0; 95% CI: Infinity, 0), but also without statistical significance; in this regard, it can be thought that certain chronic diseases are valued as elements of greater risk, and thus motivate the family to increase preventive measures.
Ethnic minorities, people from low-income households, overcrowded housing and socio-occupational level Ethnic minority communities, people from low-income households, and those living in urban areas with overcrowded housing are at increased risk of adverse outcomes [10]. But, on the other hand, it has been reported that household overcrowding was not a significant factor [9]; there was also no connection between the risk of infection and the number of all people living in the same household. Has been communicated that secondary risk of infection for people living in the same household increased from 15% (one-person households) to 44% (2 people), 35% (3 people), and 18% (4 People; p <0.001); here the researchers expected higher values [46].
Lower socioeconomic status is associated with an increased risk of contracting COVID-19 [47]. In addition, it has been shown that preventive behaviors are associated with educational and economic level [48]. We found that being a member of a low-income household showed a weak and statistically significant risk for becoming a secondary patient in the family (RR = 1.3; 95% CI: 0.99, 1.73. P <.05). The high socio-occupational level was a protective factor against secondary contagion in families (RR = 0.5; 95% CI: 0.79, 0.37. P <.05). Belonging to an ethnic minority also posed a weak risk of become secondary ill in the family (1.2; 95% CI: 0.87, 1.61), but not statistically significant. But being a “complex family” was not a significant risk (1.1; CI 95: 0.16, 7.11). The larger family size (family with> = 4 members) was a factor of certain protective benefit (RR = 0.8; 95% CI: 1.04, 0.62) but not statistically significant.
Relationship with Variables of the Index Case
The greater severity of the disease in the index case has been reported to be an increased risk of transmission, which ranged from 0.3% in asymptomatic contacts to 6.2% in severe / critical case contacts. In Guangzhou, China, secondary infection rates increased with the most severe disease in index cases and were very low with asymptomatic index cases [49]. In Wuhan asymptomatic individuals were much less likely to infect others than symptomatic cases [39].
When the index case patients had expectoration, they were associated with almost five times the risk of secondary transmission (14% vs 3% for the index cases without expectoration [49, 50]. The risk of home transmission was 18 times higher with frequent daily close contact with the primary case, and four times higher if the primary case had diarrhea [9]. The lack of symptoms that could facilitate transmission (sneezing / coughing) may explain the low transmission rate of asymptomatic cases despite similar viral loads. However, super-spreader events have been associated with presymptomatic individuals [49, 51]. In our study, the presence of cough (RR = 0.8; 95% CI: 1.07, 0.63) and being asymptomatic (RR = 0.8; 95% CI: 1.48, 0.45) in the primary case were factors of certain protective benefit, but without statistical significance, to become secondary case in the family. Again it can be hypothesized that knowledge of this risk leads families to increase their preventive measures, which makes risk a protective factor.
Study Limitations
Some limitations of our study must be taken into account:
- Genetic analyzes of the infected were not carried out and the identification of the viral strain that circulated among them was not carried out, so that the transmission and causal extension of the infection from index cases to other family members, was only presumptive based on in the timing of onset of symptoms and / or dates of PCR, in a situation of community transmission [52, 53].
- The detection of antibodies against SARS-CoV-2 was not carried out systematically, so it cannot be excluded that a healthy family member had previously had the disease.
- On the other hand, children may develop symptoms of COVID-19 and specific antibodies against SARS-CoV-2, but never test positive for the virus in a standard PCR test, which can confuse the results [54].
- The sample of included families was not a probabilistic sample; it was a convenience sample (the families participating in the study were chosen because their members were treated in the same consultation and all medical information was available). However, there are no logical reasons to think that the current research sample was different from the ideal, randomly selected sample (from the entire population), nor that there might be under- or over-represented people in the sample.
Conclusion
Our results suggest that there are biological, psychological and social factors (associated with being a young woman or older than 65 years, of low socioeconomic status, student, ethnic minority, presence of chronic diseases of the respiratory and genitourinary system) that increase the risk and that probably they reduce the motivation to comply with preventive measures to become a secondary case in families. Other biological, psychological and social factors (associated with occupational specialization, larger family size, presenting chronic diseases of the groups and neoplasms and of the blood, primary case with cough or asymptomatic) may have a preventive effect and complying with the public health advice for prevention and so, to avoid being a secondary case in families, probably by increase knowledge and motivation.
Public health councils recommend isolation of PCR- positive household members, but this can be difficult, especially in small apartments with shared facilities. Motivation to overcome these difficulties may be greater in larger families and with members with chronic diseases that can increase risk, such as neoplasms and blood diseases. The effective possibilities of doing isolation and the motivation for it, may be lower in young people, students or with low occupational level and ethnic minorities. In addition, the presence of certain diseases or known risk factors (cough in the index case, larger family size, etc.) may pose an added risk or, on the contrary, may be factors to more strictly comply with preventive measures. In summary, our results suggest that psychosocial factors (associated with the female gender, being young, ethnic minority, low socioeconomic and employment status, and related knowledge, beliefs and behaviors) are probably most important vs. biological ones (age, sex, and chronic diseases).
References
-
Wang Y, Liu Y, Liu L, Wang X, Luo N, et al. (2020) Clinical Outcomes in 55 Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Who Were Asymptomatic at Hospital Admission in Shenzhen, China. J Infect Dis 221(11): 1770-1774.
-
Tenforde MW, Rose EB, Lindsell CJ, Shapiro NI, Files DC, et al. (2020) Characteristics of Adult Outpatients and Inpatients with COVID-19-11 Academic Medical Centers, United States, March-May 2020. MMWR Morb Mortal Wkly Rep 69(26): 841-846.
-
Wu J, Huang Y, Tu C, Bi C, Chen Z, et al. (2020) Household Transmission of SARS-CoV-2, Zhuhai, China, 2020. Clin Infect Dis 71(16): 2099-2108.
-
Jing QL, Liu MJ, Zhang ZB, Fang LQ, Yuan J, et al. (2020) Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infect Dis 20(10): 1141-1150.
-
Li W, Zhang B, Lu J, Liu S, Chang Z, et al. (2020) Characteristics of Household Transmission of COVID-19. Clin Infect Dis 71(8): 1943-1946.
-
Dattner I, Goldberg Y, Katriel G, Yaari R, Gal N, et al. (2020) The role of children in the spread of COVID-19: using household data from Bnei Brak, Israel, to estimate the relative susceptibility and infectivity of children. MedRxiv.
-
Mao LJ, Xu J, Xu ZH, Xia XP, Li B, et al. (2020) A child with household transmitted COVID-19. BMC Infect Dis 20(1): 329.
-
Maeda KY, Honda C, Motegi RI (2020) Development of a Family-Friendly System for Japanese Parents Infected With COVID-19. Asia Pac J Public Health.
-
Wang Y, Tian H, Zhang L, Zhang M, Guo D, et al. (2020) Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Global Health 5(5): 002794.
-
Haroon S, Chandan JS, Middleton J, Cheng KK (2020) Covid-19: breaking the chain of household transmission. BMJ 370: 3181.
-
Turabian JL (2021) Rapid antigenic tests to detect asymptomatic covid-19 infections. Arch Community Med Public Health 7(1): 017-20.
-
Rey Calero (1989) Epidemiological method and community health. Madrid: Interamericana. McGraw- Hill.
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The C.V. Mosby Company.
-
Gill M (2017) Augmented care: An alternative model of care for people with chronic disease. Int J Care Coord 20(1-2): 5-7.
-
Larranaga AC, Vetrano DL, Onder G, Gimeno Feliu LA, Santaliestra CC, et al. (2016) Assessing and Measuring Chronic Multimorbidity in the Older Population: A Proposal for Its Operationalization. J Gerontol A Biol Sci Med 72(10): 1417-1423.
-
(2009) International Statistical Classification of Diseases and Health-Related Problems. ICD-10 Version. WHO.
-
Royal Collage of General Practitioners (1986) The Classification and Analysis of General Practice Data. Ocasional Paper 26.
-
Donaldson RJ, Donaldson LJ (1983) Essential Community Medicine. Lancaster: MTP Press.
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Turabian JL, Minier Rodriguez LE, Jove Rc, Rodriguez Almonte FE, Castro AV (2016) The Patient Companion in the Consultation of Family Medical Practice is an Indicator of Hidden Family Problems. Arch Fam Med Gen Pract 1(1): 1-6.
-
Watts C, Shrader E (1998) How to do (or not to do)… The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy and Planning 13(4): 459-464.
-
McIlvain H, Crabtree B, Medder J, Stange KC, Miller WL (1998) Using practice genograms to understand and describe practice configurations. Fam Med 30(7): 490- 496.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci 3(1): 186-191.
-
Open Source Epidemiologic Statistics for Public Health.
-
Little P, Read RC, Amlot R, Chadborn T, Rice C, et al. (2020) Reducing risks from coronavirus transmission in the home-the role of viral load. BMJ 369: 1728.
-
Wilson FP (2020) ‘Like Russian Roulette’: Why HCPs Are So Scared of COVID-19. Medscape.
-
Remaly J (2020) Two Twins, Different COVID-19 Trajectories. Medscape.
-
Pouwels KB, House T, Pritchard E, Robotham JV, Birrell PJ, et al. (2020) Community prevalence of SARS-CoV-2 in England from April to November, 2020: results from the ONS Coronavirus Infection Survey. Lancet Public Health 6(1): 30-38.
-
Castineira EP, Clohisey S, Klaric L, Bretherick AD, Rawlik K, et al. (2020) Genetic mechanisms of critical illness in Covid-19. Nature.
-
Duggal P, Thio CL, Wojcik GL, Goedert JJ, Mangia A, et al. (2013) Genome-wide association study of spontaneous resolution of hepatitis C virus infection: data from multiple cohorts. Ann Intern Med 158(4): 235-245.
-
Broadfoot M (2020) DNA Could Hold Clues to Varying Severity of COVID-19. The Scientist.
-
Kozlov M (2020) Key Genes Related to Severe COVID-19 Infection Identified. Differences in the expression of genes associated with antiviral immunity and lung inflammation may contribute to a more serious COVID-19 infection. The Scientist.
-
Althouse BM, Wenger EA, Miller JC, Scarpino SV, Allard A, et al (2020) Stochasticity and heterogeneity in the transmission dynamics of SARS-CoV-2. ArXiv.
-
Moschetti J (2020) Massive screening: Professor Antoine Flahault is “not convinced”. Medscape.
-
Mohindra R, Ghai A, Brar R, Khandelwal N, Biswal M, et al. (2021) Superspreaders: A Lurking Danger in the Community.J Prim Care Community Health 12: 1-4.
-
Carvalho T (2020) COVID-19 clusters. Nat Med 26: 1806.
-
Meyerowitz EA, Richterman AG (2020) Viral Shedding and COVID-19 Superspreading Events. Medscape.
-
Li F, Li YY, Liu MJ, Fang LQ, Dean NE, et al. (2021) Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: a retrospective observational study. Lancet Infect Dis.
-
Waisgrais S (2020) Survey of Perception and Attitudes of the Population. Impact of the COVID-19 pandemic and the measures taken by the government on daily life. First edition, April 2020. Unicef Argentina.
-
Turabian JL (2020) Sex and Gender Bio-psychosocial Differences in Coronavirus Disease 2019 (Covid-19): Men have more Biological Problems, but Women Suffer more Long-Term Serious Psychosocial Consequences and with more Implications for Population. J Women’s Health Care 9(3): 487.
-
Xie J, Tong Z, Guan X, Du B, Qiu H (2020) Clinical Characteristics of Patients Who Died of Coronavirus Disease 2019 in China. JAMA Netw Open 3(4): 205619.
-
Wu KJ (2020) Studies Begin to Untangle Obesity’s Role in Covid-19, People with extra weight may struggle to mount a robust immune response to the coronavirus- and may respond poorly to a vaccine. The New York Times.
-
Guo W, Li M, Dong Y, Zhou H, Zhang Z, et al. (2029) Diabetes is a risk factor for the progression and prognosis of COVID‐19. Diabetes Metab Res Rev 36(7): 3319.
-
Tucker ME (2020) COVID-19 and Diabetes: Known Mechanisms and a ‘New Beast’?. Medscape.
-
van den Heuvel M (2020) Heinsberg study in “preprint”: high number of unreported infections, death rate only 0.36% - does that apply to the whole of Germany?. Medscape.
-
Oh TK, Choi JW, Song IA (2021) Socioeconomic disparity and the risk of contracting COVID-19 in South Korea: an NHIS-COVID-19 database cohort study. BMC Public Health 21: 144.
-
Firouzbakht M, Omidvar S, Firouzbakht S, Amoli AA (2021) COVID-19 preventive behaviors and influencing factors in the Iranian population; a web-based survey. BMC Public Health 21: 143.
-
Luo L, Liu D, Liao X, Wu X, Jing Q, et al. (2020) Contact settings and risk for transmission in 3410 close contacts of patients with COVID-19 in Guangzhou, China: A prospective cohort study. Ann Intern Med.
-
Frellick M (2020) Risk of Secondary COVID-19 Transmission Low in Most Settings. Medscape.
-
Shen Y, Li C, Dong H, Wang Z, Martinez L, et al. (2020) Community outbreak investigation of SARS-CoV-2 transmission among bus riders in Eastern China. JAMA Intern Med 180(12): 1665-1671.
-
Winter L (2020) Conference Linked to as Many as 300,000 COVID-19 Cases: Study. Around 100 people were infected at a scientific meeting hosted by Biogen in Boston in February. Then they went back home, taking the virus with them. The Scientist.
-
Lemieux JE, Siddle KJ, Shaw BM, Loreth C, Schaffner SF, et al. (2020) Phylogenetic analysis of SARS-CoV-2 in Boston highlights the impact of superspreading events. Science 371(6529): 3261.
-
Nogrady B (2020) How kids’ immune systems can evade COVID. Childrens’ untrained immune response seems to be key to eliminating SARS-CoV-2. Nature 588: 382.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria