COVID-19 Asymptomatic Cases in the Family Distort the Characteristics of True Primary and Secondary Cases
Background: The presence of COVID-19 asymptomatic cases within the family could bias SARS-CoV-2 transmission study. Objective: To study the differences respect to certain chosen variables, between the index cases and secondary cases in families with asymptomatic cases and in families without asymptomatic cases. Methodology: An observational and retrospective study of families in which there was at least two polymerase chain reaction (PCR) confirmed COVID-19 cases -one primary case or index and one secondary case-, was conducted from March 15 to December 31, 2020, in a general medicine office in Toledo, Spain. Socio-demographic and clinical variables of the index cases and of the secondary cases were compared between families with asymptomatic cases and families without asymptomatic cases. Results: 109 people from 39 families were included. The primary cases of families with asymptomatic cases differed statistically significant from the primary cases of families without asymptomatic cases because they were more women, families with a greater number of members, and presented more respiratory symptoms. The secondary cases of families with asymptomatic cases would differ significantly from the secondary cases of families without asymptomatic cases due to being younger, having more students, more ethnic minorities, low-income households, less severe, and presenting more chronic musculoskeletal diseases. Conclusion: The characteristics of primary and secondary cases of COVID-19 in families differ depending on whether or not there are asymptomatic cases (which can be difficult to classify as secondary or primary), which can confuse the epidemiological results.
Introduction
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2) [1] is complex, with variable clinical symptoms and disease severity. Several features of SARS-CoV-2 make accurate detection during the ongoing epidemic challenging, including high transmissibility, an incubation period with a long-tailed distribution, pre-symptomatic transmission, and the existence of asymptomatic infections, which may also contribute to transmission [2, 3, 4, 5, 6, 7, 8].
Household contacts that are isolated within the same home as the index case make up the majority of the infected person’s contacts and are likely to remain exposed to the infected household member during this period of isolation [9]. Although SARS-CoV-2 transmission occurs within households, however, estimates of transmission vary widely, which may be due to different study methodologies [10]. An important detail is the fact that the extent and direction of the causal transmission of SARS CoV-2 in families, in a situation of community transmission, can only be determined as presumptive, except: a) When all cases are symptomatic (and symptom onset dates are available); when there are asymptomatic cases, it is not possible to determine whether the index case was a symptomatic case with cataloged symptom onset dates or an asymptomatic case; so that both transmission directions would be possible under these circumstances [11]. b) If genetic analysis is available of the infected cases and their family contacts and identify the viral strain that circulated among them [12, 13].
In this context, it has been claimed that up to 40% of infections may be asymptomatic and have been implicated in diseases transmission [14, 15, 16, 17], with an increase in the probability of exposure of household members, and the transmission of COVID -19 within families accounts for the majority of epidemic growth [18]. Thus, the objective of this study, based on a retrospective analysis, in a General Medicine office, in Toledo (Spain) from March to December 2020, was to study the differences, with respect to certain chosen variables, between the index cases and secondary cases, in families with asymptomatic cases and in families without asymptomatic cases, to assess whether the presence of secondary asymptomatic cases (which have been classified as such without complete assurance of their condition as secondary due to their asymptomatic nature) could distort the epidemiologic characteristics of the primary cases and secondary within families.
Material and Methods
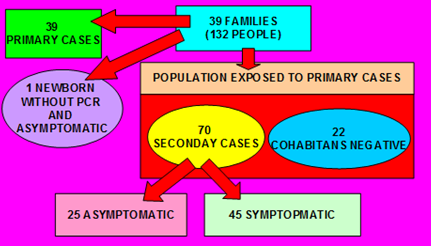
An observational and retrospective study of 39 families y 132 people, in which there was at least two polymerase chain reaction (PCR) confirmed COVID-19 cases -one primary case or index and one secondary case-, was conducted from March 15 to December 31, 2020, in a general medicine office in Toledo, Spain. The study was part of a set of studies on COVID-19 in families, and in part the methodology has already been published [19, 20]. Secondary cases without infection (with negative PCR and asymptomatic) were excluded within the family, and the variables collected were analyzed as predictors of secondary transmission.
Diagnosis of COVID-19
Symptomatic cases: The diagnosis was confirmed with PCR oropharyngeal. Information on COVID-19 patients and their contacts was obtained from the registry systems used by general medical services in the consultation. A confirmed case with active infection was considered to be any person with a clinical picture of sudden onset acute respiratory infection of any severity that occurs, among others, with fever, cough or feeling of shortness of breath; other symptoms such as odynophagia, anosmia, ageusia, muscle pain, diarrhea, chest pain or headache, among others, were also considered symptoms of suspected SARS-CoV-2 infection according to clinical criteria, and a positive PCR test. People with symptoms compatible with COVID-19 who had already had a PCR-confirmed SARS-CoV-2 infection in the previous 90 days were not considered suspect cases again [21]. Primary case or index: It refers to the first case diagnosed or reported in the family. Asymptomatic cases: They were defined as family members who, after the appearance of the index case, had positive PCR without the presence of any symptoms. Household contacts: Household contacts were defined as people who shared a residence with the COVID-19 index case. We defined family members as those who had lived with primary cases in a house 4 days before and for more than 24 hours after the primary cases developed illness related to COVID-19. Families with secondary transmission were defined as those where some or all of the family members become infected within one incubation period (2 weeks) of symptom onset of the primary case. The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [22]. The onset date for an asymptomatic carrier was defined as the date a positive COVID-19 PCR test was obtained. Contacts were quarantined shortly after the index case was diagnosed, thereby reducing the risk of transmission (a provision not available in all circumstances).
Collected variables
Data on the index case and close contacts were extracted from the medical records of the general medicine practice under study. The following variables were collected: age; sex; symptoms; duration of symptoms; previous known contacts; chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment” [23], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD- 10 Version: 2019 [24]; social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [25, 26]; complex family and low income household based on the genogram and in the experience of the general practitioner for their continuity of care and knowledge of the family (genogram is a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that “complex” genograms present families with psychosocial problems) [27, 28, 29, 30]; ethnic minority; family size (number of members); and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths / min.; pulse oxygen saturation ≤ 93% with room air at rest; arterial partial pressure of oxygen / oxygen concentration ≤ 300 mmHg.) [22]. To simplify comparison, moderate and severe cases were counted together.
Sample: A convenience sampling was used. The families participating in the study were chosen because they had their members in the same consultation and all medical information was available. Sample size: Sample size was calculated for an unpaired study for a Two-sided Confidence Level (1-alpha) of 95, a Power (% probability of detection) of 80, a Ratio of 0.23, a hypothetical ratio of being a woman in primary cases in families with asymptomatic cases of 75%, and a hypothetical proportion of being a woman in primary cases in families without asymptomatic cases of 10%. These data indicate a sample size of 30, 24 primary cases in families with asymptomatic cases and 6 primary cases in families without asymptomatic cases (Fleiss) [31].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test when necessary, (according to the number the expected cell totals) for percentages, and the Student t test for the mean.
Results
Thirty-nine families with 131 cohabitants were included, where there was one primary case and at least one secondary case (one newborn without CRA and asymptomatic was excluded). Of these families, 21 had at least one asymptomatic secondary case, with 44 secondary cases; and 18 families had no asymptomatic secondary cases, with 26 secondary cases. In both groups of families (with and without asymptomatic secondary cases), 22 cases with negative PCR were excluded from the analysis, therefore, 109 people from 39 families were studied (Figure 1).
The primary cases of families with asymptomatic cases differed statistically significantly from the primary cases of families without asymptomatic cases because they were more women, were families with a greater number of members, and presented more respiratory symptoms (Tables 1-3). The secondary cases of families with asymptomatic cases would differ significantly from the secondary cases of families without asymptomatic cases due to being younger, having more students, being more ethnic minorities, being low- income households, being less severe and presenting more chronic musculoskeletal diseases (Tables 4-6).
| Variables | Primary Cases in Families with Asymptomatic Cases (N = 21) | Primary Cases in Families without Asymptomatic Cases (N = 18) | Statistical Significance | |
|---|---|---|---|---|
| -Woman | 15 (71) | 5 (28) | X2=7.3919. p= .006552. Significant at < .05. | |
| -Age (years) (arithmetic mean and standard deviation) | 38.23 +-17.62 | 39.44 +-12.73 | t= -0.24123. NS | |
| > = 65 years | 0 | 0 | Fisher exact test= 1. NS | |
| < 45 years | 14 (67) | 12 (67) | X2= 0. NS | |
| -Workers with some type of specialization | 14 (67) | 7 (39) | X2=3.0093. NS | |
| -Students | 4 (19) | 3 (17) | X2 with Yates correction= 0.0508. NS | |
| -Ethnic minority | 5 (24) | 3 (17) | X2 with Yates correction= 0.0234. NS | |
| -Low income household | 4 (19) | 3 (17) | X2 with Yates correction= 0.0508. NS | |
| -Complex family | 6 (29) | 2 (11) | X2 with Yates correction= 0.8996. NS | |
| -Number of people per family | 3.85 +-0.85 | 2.83+-0.78 | t= 3.87208. p= .000212. Significant at p < .05. | |
| -Family with > = 4 members | 13 (62) | 4 (22) | X2=6.207. p= .012724. Significant at p < .05. | |
| -Known contact | 9 (43) | 5 (28) | X2= 0.9578. NS |
Table 1: ** Comparison between Primary Cases in Families with Asymptomatic Cases (N = 39) and Primary Cases in Families without A
( ): Denotes percentages of total in primary cases NS: Not significant at p< .05. Table 1: Comparison between Primary Cases in Families with Asymptomatic Cases (N = 39) and Primary Cases in Families without Asymptomatic Cases (N = 18).
| Symptoms* | Primary Cases in Families with Asymptomatic Cases (N = 21) | Primary Cases in Families without Asymptomatic Cases (N = 18) | Statistical Significance |
|---|---|---|---|
| General (discomfort, Asthenia, Myalgia, fever) | 20 (31) | 26 (44) | X2=2.1543. NS |
| Respiratory (Cough, Dyspnea, Chest pain) | 25 (39) | 13 (22) | X2=4.1696. p= .041156. Significant at p < .05. |
| ENT (Anosmia / Ageusia, Odynophagia, Rhinorrhea) | 11 (17) | 7 (12) | X2=0.6963. NS |
| Digestive (Anorexia, Nausea / Vomiting, Diarrhea, Abdominal pain) | 3 (5) | 4 (7) | X2=0.2504. NS |
| Neurological (Headache, dizziness) | 5 (8) | 6 (10) | X2=0.2094. NS |
| Psychiatric (Anxiety, Insomnia) | 0 | 2 (3) | Fisher exact test= 0.1074. NS |
| Skin (Chilblains, Flictenas, Rash) | 0 | 1 (2) | Fisher exact test= 0.4797. NS |
| Total symptoms | 64 (100) | 59 (100) | |
| Pneumonia | 5 (24) | 1 (6) | Fisher exact test= 0.1897. NS |
| -Duration of symptoms in days (arithmetic mean and standard deviation) | 12.38+-15.54 | 11.44+-8.08 | t= 0.22997. NS |
| Moderate-severe cases | 5 (38) | 1 (6) | Fisher exact test= 0.1897. NS |
| -Exitus | 1 (5) | 0 | Fisher exact test= 1. NS |
| Chronic Diseases According to WHO, ICD- 10 GROUPS * | Primary Cases in Families with Asymptomatic Cases (N = 21) | Primary Cases in Families without Asymptomatic Cases (N = 18) | Statistical Significance |
| -Presence of crhonic diseases | 10 (48) | 9 (50) | X2= 0.022. NS |
| -II Neoplasms | 3 (19) | 0 | Fisher exact test= 0.2348. NS |
| -IV Endocrine | 5 (31) | 2 (14) | Fisher exact test = 0.4179. NS |
| -V Mental | 2 (13) | 3 (22) | Fisher exact test= 0.6466. NS |
| -VI-VIII Nervous and Senses | 0 | 2 (14) | Fisher exact test= 0.2065. NS |
| -IX Circulatory system | 2 (13) | 2 (15) | Fisher exact test= 1. NS |
| -X Respiratory system | 2 (12) | 1 (7) | Fisher exact test= 1. NS |
| -XI Digestive system | 0 | 1 (7) | Fisher exact test= 0.4615. NS |
| -XII Diseases of the skin | 1 (6) | 0 | Fisher exact test= 1. NS |
| -XIII Musculo-skeletal | 1 (6) | 1 (7) | Fisher exact test= 1. NS |
| -XIV Genitourinary | 0 | 2 (14) | Fisher exact test= 0.2065. NS |
| TOTAL | 16 (100) | 14 (100) |
Table 2: ** Comparison of Symptoms in Primary Cases between Families with Asymptomatic Cases (N=21) and Families without Asymptom
( ): Denotes percentages of total in primary cases *Patients could have more than one symptom. The percentages are over the total of symptoms of primary cases NS: Not significant at p< .05. Table 2: Comparison of Symptoms in Primary Cases between Families with Asymptomatic Cases (N=21) and Families without Asymptomatic Cases (N = 18).
( ): Denotes percentages of total in primary cases *Patients could have more than one chronic disease. The percentages are over the total of chronic disease of primary cases. NS: Not significant at p< .05. Table 3: Comparison of Chronic Diseases in Primary Cases between Families with Asymptomatic Cases (N = 21) and Families without Asymptomatic Cases (N = 18).
| Variables | Secondary Cases in Families with Asymptomatic Cases (N = 44) | Secondary Cases in Families without Asymptomatic Cases (N = 26) | Statistical Significance |
|---|---|---|---|
| -Woman | 32 (73) | 19 (73) | X2= 0.001. NS |
| Age (years) (arithmetic mean and standard deviation) | 28.43 +-19.91 | 38.83+-20.96 | t= -1.13416. NS |
| > = 65 years | 3 (7) | 3 (11) | Fisher exact test= 0.6635. NS |
| < 45 years | 37 (84) | 14 (54) | X2= 7.5596. p= .005969. Significant at p < .05. |
| -Workers with some specialization | 13 (30) | 7 (27) | X2= 0.0551. NS |
| -Students | 21 (48) | 6 (23) | X2= 4.1912. p= .040634. Significant at p < .05. |
| -Ethnic minority | 20 (45) | 3 (11) | X2= 8.5214. p= .00351. Significant at p < .05. |
| -Low income household | 20 (45) | 3 (11) | X2= 8.5214. p= .00351. Significant at p < .05. |
| -Complex family | 10 (23) | 2 (8) | X2 with Yates correction= 1.6501. NS |
| -Family with > = 4 members | 11 (25) | 5 (19) | X2= 0.3085. NS |
| Symptoms* | Secondary Cases in Families with Asymptomatic Cases (N = 44) | Secondary Cases in Families without Asymptomatic Cases (N = 26) | Statistical Significance |
| General (discomfort, Asthenia, Myalgia, fever) | 15 (31) | 23 (32) | X2= 0.0064. NS |
| Respiratory (Cough, Dyspnea, Chest pain) | 16 (33) | 24 (33) | X2= 0. p= 1. NS |
| ENT (Anosmia / Ageusia, Odynophagia, Rhinorrhea) | 8 (17) | 9 (13) | X2= 0.4112. NS |
| Digestive (Anorexia, Nausea / Vomiting, Diarrhea, Abdominal pain) | 5 (11) | 6 (8) | X2 with Yates correction= 0.0042. NS |
| Neurological (Headache, dizziness) | 3 (6) | 6 (8) | X2 with Yates correction= 0.005. NS |
| Psychiatric (Anxiety, Insomnia) | 1 (2) | 2 (3) | Fisher exact test statistic= 1. NS |
| Skin (Chilblains, Flictenas, Rash) | 0 | 2 (3) | Fisher exact test= 0.516. 1. NS |
| Total symptoms | 48 (100) | 72 (100) | - |
| Pneumonia | 7.73+-13.17 | 10.53+-10.16 | t= -0.81759. NS |
| (n = 19; not counting 25 asymptomatic cases) | |||
| -Duration of symptoms in days (arithmetic mean and standard deviation) | 0 | 3 (11) | Fisher exact test = 0.0475. Significant at p < .05. |
| Moderate-severe cases | 0 | 3 (11) | Fisher exact test = 0.0475. Significant at p < .05. |
| -Exitus | 0 | 1 | Fisher exact test= 0.3714. NS |
Table 3: ** Comparison between Secondary Cases in Families with Asymptomatic Cases (N = 44) and Secondary Cases in Families with
( ): Denotes percentages of total in secondary cases NS: Not significant at p< .05. Table 4: Comparison between Secondary Cases in Families with Asymptomatic Cases (N = 44) and Secondary Cases in Families with No Asymptomatic Cases (N = 26).
( ): Denotes percentages of total in primary cases and in secondary cases * Patients could have more than one symptom. The percentages are over the total of symptoms of primary cases and of secondary cases NS: Not significant at p< .05. Table 5: Comparison of Symptoms in Secondary Cases between Families with Asymptomatic Cases (N = 44) and Families without Asymptomatic Cases (N = 26).
| Secondary Cases in Families with Asymptomatic CASES (N = 44) | Secondary Cases in Families without Asymptomatic CASES (N = 26) | Statistical Significance | |
|---|---|---|---|
| -Presence of crhonic diseases | 17 (39) | 14 (54) | X2= 1.5323. NS |
| -II Neoplasms | 1 (3) | 0 | Fisher exact test= 0.4478. NS |
| -IV Endocrine | 8 (27) | 13 (36) | X2= 0.5521. NS |
| -V Mental | 7 (23) | 3 (8) | X2 with Yates correction= 1.9443. NS |
| -VI-VIII Nervous and Senses | 1 (3) | 5 (13) | Fisher exact test= 0.2131. NS |
| -IX Circulatory system | 1 (3) | 4 (11) | Fisher exact test= 0.37. NS |
| -X Respiratory system | 1 (3) | 2 (5) | Fisher exact test= 1. NS |
| -XI Digestive system | 2 (7) | 3 (8) | Fisher exact test= 1. NS |
| -XII Diseases of the skin | 2 (7) | 1 (3) | Fisher exact test= 0.5829. NS |
| -XIII Musculo-skeletal | 7 (24) | 1 (3) | X2 with Yates correction= 4.8877. p= .027049. Significant at p< .05. |
| -XIV Genitourinary | 0 | 5 (13) | Fisher exact test= 0.0599. NS |
| TOTAL | 30 (100) | 37 (100) |
Table 4: ** Comparison of Chronic Diseases in Secondary Cases between Families with Asymptomatic Cases (N = 44) and Families with
( ): Denotes percentages of total in primary cases and in secondary cases *Patients could have more than one chronic disease. The percentages are over the total of chronic disease of primary and secondary cases NS: Not significant at p< .05. Table 6: Comparison of Chronic Diseases in Secondary Cases between Families with Asymptomatic Cases (N = 44) and Families without Asymptomatic Cases (N = 26).
Discussion
Transmission in the Home: Importance, Difficulties and Biases in its Determination
Most people with COVID-19 receive care at home, increasing the likelihood of exposure for household members [17]. The domestic transmissibility of SARS-CoV-2 remains unclear, although it is accepted that homes where someone is ill with covid-19 remain hotspots for the transmission of the virus, even if the overall community spread slows [32]. But the exact transmission rate is not known, as different studies show results that vary widely. In a prospective study that included systematic and daily follow-up, was found that more than half of the people (53%) living with someone with COVID-19 became infected within a week; and less than half of the infected household members had symptoms when the infection was first detected. Many reported no symptoms during the 7-day follow-up, underscoring the potential for transmission from asymptomatic secondary contacts. Children may show minimal symptoms but still be contagious. On the other hand, in families, it has been reported that more than a third of close contacts positive for SARS-CoV-2 were asymptomatic, and home secondary attack rate ranged from 8% to 23% [33].
Of course, these large differences in reported secondary attack rates may be due to several factors [10]: a) Several studies have reported estimates of home transmission, mainly from contact tracing activities, with limited follow-up and testing of household members or late enrolment in relation to index patient identification b) Other studies have been prospective and have included systematic and daily follow-up of family members. c) Other studies have included the rapid isolation of patients in facilities outside the home or the adoption of different control measures, such as the use of a mask at home.
But, it is really only possible to determine with certainty the direction of interfamilial transmission when all cases are symptomatic (and the dates of onset of symptoms are available). But when there are asymptomatic cases, it is not possible to determine whether the index case was a symptomatic case with catalogued symptom onset dates or an asymptomatic case; so that both directions of transmission would be possible under those circumstances [11]. Furthermore, without genetic analysis of the cases and their infected family contacts and identifying the viral strain that circulated among them, the transmission and causal extension of the infection from index cases to other family members, in a situation of community transmission, is only presumptive based (according timing of onset of symptoms and / or dates of PCR) [12, 13].
What’s more, the long incubation and high presymptomatic infectivity of COVID-19 make transmission between family members a particular risk. Modeling of COVID-19 viral shedding suggests that the highest viral load is found at the onset of symptoms or just before, and that 44% of transmission occurs before symptoms. Public health councils recommend isolation of symptomatic household members, but this can be difficult, especially in small apartments with shared facilities [17].
Confounding Factors about the Characteristics of Index Cases and Secondary Cases In Families When Asymptomatic Ones Are Included
Our study suggests that there are a number of confounding variables when studying secondary cases in families when there are asymptomatic cases. These would be, at least:
Social Determinants of Health in the Family Context: Ethnic Minorities and Low-Income Households
COVID-19 has disproportionately hit the poor and ethnic minorities [34]. To the extent that family functioning is poorer in poor families and family structure and functioning are linked to health. The family context in which people eat, sleep and live is both a structural determinant (family structure) and an intermediate determinant (family functioning) of health and being affected by health [35]. Evidence also suggests that socioeconomic factors may be drivers of variations in COVID-19 morbidity and mortality. For example, COVID-19-related mortality in England and Wales is almost twice the rate in the most deprived areas compared to the least deprived [36]. The US Centers for Disease Control and Prevention outlines a list of risk factors for SARS-CoV-2 infection, including poverty and overcrowding. Also, a study conducted in the United Kingdom investigated the role of ethnicity and socioeconomic position in the development of SARS-CoV-2 infection; the authors found that socioeconomic deprivation and low educational attainment were consistently associated with a high risk of confirmed infection. Furthermore, reports have shown higher mortality from infectious diseases in patients with low levels of education. Various types of health behaviors, such as smoking, excessive alcohol consumption, physical inactivity and an unhealthy diet, are expected to mediate the impact of educational attainment on the incidence of diseases. Low levels of education are related to a high incidence and prevalence of cardiovascular and cerebrovascular diseases, cancer, diabetes, hypertension, and chronic respiratory diseases [37]. The socioeconomic level of the patients influences educational inequalities in non-communicable diseases [38].
In age-adjusted models, people of all ethnic minority groups have at elevated risk of mortality from COVID-19. The differences in mortality from COVID-19 between ethnic groups are largely attenuated by geographic and sociodemographic factors, although some residual differences persisted [39]. The elevated COVID-19 mortality risk for ethnic minority groups is largely due to location, living circumstances, socioeconomic factors, occupational exposure, and self-management reported health status [39].
We found that the secondary cases of families with asymptomatic cases differed significantly from the secondary cases of families without asymptomatic cases because they were more ethnic minorities and were low-income households. Consequently, including asymptomatic cases in families can skew the characteristics of the cases towards a greater presence of ethnic minorities and a low social level.
Clinical Presentation
Clinical presentation of secondary contacts has been reported to be asymptomatic in 6%, mild in 16%, moderate in 68%, and severe / critical in 10% [40]. Likewise, the greater severity of the disease in the index case results in a greater risk of transmission, which vary from 0.3% in contacts of asymptomatic cases to 6% in contacts of severe / critical cases [40]. When the index case patients had expectoration, they were associated with almost five times the risk of secondary transmission (14% versus 3% for the index cases without expectoration) [40, 41].
In our study, the secondary cases of families with asymptomatic cases differed significantly from the secondary cases of families without asymptomatic cases because they were less severe. And on the other hand, we found that the primary cases of families with asymptomatic cases differed statistically significantly from the primary cases of families without asymptomatic cases presenting more respiratory symptoms. Consequently, the presence of asymptomatic cases biases the characteristics of familial secondary cases towards less severity, and familial primary cases towards a higher prevalence of respiratory symptoms.
Family Size and SARS CoV-2 Infection
Connection has not been proven to date between the risk of infection and the number of all people living in the same household. In one study, the secondary risk of infection for those living in the same household increased from 15% (1 person households) to 44% (2 persons), 35% (3 persons) and 18% (4 Persons; where the researchers expected higher values) [42]. In our study we found that the primary cases of families with asymptomatic cases differed in a statistically significant way from the primary cases of families without asymptomatic cases because they were families with a greater number of members. In other words, the inclusion of asymptomatic cases biases the characteristics of the primary cases in families towards households with more members.
Sex/Gender
The data suggests that men and women are equally likely to acquire COVID-19, but men are at increased risk of severe illness and death for biological and cultural reasons. On the other hand, in the COVID-19 pandemic, greater psychosocial effects can be observed in women, in relation to work, family, intra-family transmission and childcare, quarantine affectation, etc., which is aggravated by the fact that the majority of health workers are women. Outcomes for women in crisis situations are significantly worse [43]. The sex ratio varies with age. In both the youngest age groups (20-29 years) and the elderly (80 years or older), there are more cases in women than in men. However, for other age groups (0-9 years, 60-69 years and 70-79 years), there are more cases in men than in women [44]. We found that primary cases of families with asymptomatic cases differed statistically significantly from the primary cases of families without asymptomatic cases because they were more women. In other words, the characteristics of primary cases in families tend to bias towards a greater presence of women when including asymptomatic cases
Children and Adolescents in the Domestic Transmission of SARS-CoV-2
A detailed study of family groups reveals that children were rarely the index case or the probable vector of the spread of SARS-CoV-2 infection in the home [45]. In a secondary analysis of a household contact study, in a cohort of children and their household contacts, including the COVID-19 index case, for 14 days after exposure, 28% of pediatric contacts and 30% of those adult contacts tested positive.
Transmission to adults was similar in households with and without children (28% and 33%). Among pediatric contacts, 63% were children of an adult index case. An infected parent posed the highest risk for a child, but this risk was not correlated with household size, age, or underlying diseases. Children reported symptoms less frequently than adults and experienced a shorter duration of symptoms (10 days vs. 16 days). Although children transmit SARS-CoV-2, they do so at lower rates than adults, and when children, especially young children, acquire the infection, their symptoms are milder. Mild or absent symptoms in children may allow the infection to go unrecognized, possibly increasing the risk of transmission [46]. Children between the ages of 10 and 19 can transmit SARS-CoV-2 to household members more easily than adults. When the index patient was between 10 and 19 years old, 19% of the household contacts were infected. In contrast, when the index patient was between 30 and 49 years old, 12% of the household members were infected (and when the index patient was between 0 and 9 years old, only 5% of the household contacts were infected); but, authors write they could not determine the direction of transmission [11].
It has been reported that children and adolescents under 20 years of age were more likely to infect others than adults 60 years and older. Asymptomatic individuals were much less likely to infect others than symptomatic cases. Children and adolescents were less susceptible to infection, but more infectious once infected, than people 20 years of age or older. Overall, both the observed secondary attack rate and the model-estimated probabilities of infection (with respect to susceptibility) increased with the age of household contacts [47].
We find many asymptomatic cases in families, preferably in children and adolescents; Thus, it is not possible to determine whether these asymptomatic children were secondary cases or index cases in the families. This difference is an important limitation, since the two hypotheses that: 1) Children are asymptomatic secondary cases; or 2) Children are primary cases in families, cannot be clarified, and this have important and very different implications.
It gives the impression that children can represent a gateway for SARS Cov-2 in families that should not be excluded at all. We found that the secondary cases of families with asymptomatic cases differed significantly from the secondary cases of families without asymptomatic cases because they were younger, and there were more students. In other words, the inclusion of asymptomatic cases skews the characteristics of secondary cases in families towards young students.
Limitations of the Study
The study has two important limitations. The sample of families included was not a probabilistic sample; it was a convenience sample (The families participating in the study were chosen because their members were treated in the same consultation and all the medical information was available). However, there are no logical reasons to think that the current research sample was different from the ideal, randomly selected sample (from the entire population), nor that there might be under- or over-represented people in the sample. On the other hand, another limitation is the small sample size; although the sample size fulfilled the requirements for some variables, it did not, however, for all of them.
Conclusion
Asymptomatic infections are one of the most mysterious and disturbing aspects of COVID-19 and its true impact on the spread of the pandemic has yet to be verified. In the context of general medicine in Toledo (Spain), the characteristics of primary and secondary cases of COVID-19 in families differ depending on whether or not there are asymptomatic cases (which can be difficult to classify as secondary or primary); so they can confuse epidemiological results, producing a bias towards primary cases more frequently women and in families with a greater number of members, and towards younger secondary cases, students, ethnic minorities, low-income and less serious households. In summary, the presence of asymptomatic secondary cases in families biases the epidemiological data towards a greater presence of women and a larger family size in index cases, and a greater presence of social factors, less severity and younger ages in secondary cases.
References
-
Coronavirus disease (COVID-19)/Technical guidance (2020) Naming the coronavirus disease (COVID-19) and the virus that causes it.
-
Russell TW, Golding N, Hellewell J, Abbott S, Wright L, et al. (2020) Reconstructing the early global dynamics of under-ascertained COVID-19 cases and infections. BMC Med 18(332).
-
Abbott S, Hellewell J, Munday J, Funk S (2020) The transmissibility of novel Coronavirus in the early stages of the 2019–20 outbreak in Wuhan: Exploring initial point-source exposure sizes and durations using scenario analysis. Wellcome Open Res 5: 17.
-
Tindale L, Coombe M, Stockdale JE, Garlock ES, Lau Venus WY, et al. (2020) Transmission interval estimates suggest pre-symptomatic spread of COVID-19. Epidemiology.
-
Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, et al. (2020) Early dynamics of transmission and control of COVID-19: a mathematical modelling study. Lancet Infect Dis 20(5): 553-558.
-
Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI et al. (2020) Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health 8(4): 488-496.
-
Bai Y, Yao L, Wei T, Tian F, Jin DY, et al. (2020) Presumed asymptomatic carrier transmission of COVID-19. JAMA 323(14): 1406-1407.
-
Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, et al. (2020) The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med 172(9): 577-582.
-
Yu HJ, Hu YF, Liu XX, Yao XQ, Wang QF, et al. (2020) Household infection: The predominant risk factor for close contacts of patients with COVID-19. Travel Med Infect Dis 36: 101809.
-
Grijalva CG, Rolfes MA, Zhu Y, McLean HQ, Hanson KE, et al. (2020) Transmission of SARS-COV-2 Infections in Households- Tennessee and Wisconsin, April– September 2020. MMWR Morb Mortal Wkly Rep 69(44): 1631-1634.
-
Park YJ, Choe YJ, Park O, Park SY, Kim YM, et al. (2020) Contact tracing during coronavirus disease outbreak, South Korea, 2020. Emerg Infect Dis 26(10): 2465-2468.
-
Winter L (2020) Conference Linked to as Many as 300,000 COVID-19 Cases: Study. Around 100 people were infected at a scientific meeting hosted by Biogen in Boston in February. Then they went back home, taking the virus with them. The Scientist.
-
Lemieux JE, Siddle KJ, Shaw BM, Loreth C, Schaffner SF (2020) Phylogenetic analysis of SARS-CoV-2 in Boston highlights the impact of super spreading events. Science 371(6529): 3261.
-
Oran DP, Topol EJ (2020) Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann Intern Med 173: 362-367.
-
Laber Warren E (2020) Why Do Some People Weather Coronavirus Infection Unscathed? Medscape.
-
Pan Y, Yu X, Du X, Li Q, Qin T, et al. (2020) Epidemiological and Clinical Characteristics of 26 Asymptomatic Severe Acute Respiratory Syndrome Coronavirus 2 Carriers. J Infect Dis 221(12): 1940-1947.
-
Little P, Read RC, Amlôt R (2020) Reducing risks from coronavirus transmission in the home-the role of viral load. BMJ 369: 1728.
-
Wang Y, Tian H, Zhang L, Zhang M, Guo D, et al. (2020) Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Global Health 5: e002794.
-
Turabian JL (2021) SARS-COV-2 infection prevalence and characteristics in domestic contacts: Study of 39 families and 132 people in a general medicine clinic in Toledo (Spain): Implications for the general practitioners. Int J Epidemiol Health Sci 2(1): 02.
-
Turabian JL (2021) A Longitudinal Study of SARS- CoV-2 Secondary Infection Risks in Family Members: Psychosocial Factors May be More Important than Biological Ones. Epidemol Int J 5(1): 1-11.
-
(2020) COVID-19 early detection, surveillance and control strategy. Ministerio de Sanidad. España.
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The C.V. Mosby Company.
-
WHO (2019) International Statistical Classification of Diseases and Health-Related Problems.ICD-10 Version.
-
Royal Collage of General Practitioners (1986) The Classification and Analisis of General Practice Data. Ocasional Paper 26.
-
Donaldson RJ, Donaldson LJ (1983) Essential Comunity Medicine. Lancaster: MTP Press.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci 3(1): 186-191.
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Watts C, Shrader E (1998) How to do (or not to do)…The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy Plan 13(4): 459-464.
-
McIlvain H, Crabtree B, Medder J, Stange KC, Miller WL (1998) Using practice genograms to understand and describe practice configurations. Fam Med 30(7): 490- 496.
-
Open Source Epidemiologic Statistics for Public Health.
-
Madewell ZJ, Yang Y, Longini IM, Halloran ME, Dean NE (2020) Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw Open 3(12): 2031756.
-
Ng OY, Marimuthu K, Koh V, Pang J, Lin KZ, et al. (2020) SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: a retrospective cohort study. Lancet Infect Dis 21(3): 333-343.
-
Doolittle BR (2021) Are we Athens or Florence? COVID-19 in historical context. Fam Med Community Health 9(1): 000811.
-
Booysen F, Botha F, Wouters E (2021) Conceptual causal models of socioeconomic status, family structure, family functioning and their role in public health. BMC Public Health 21: 191.
-
Niedzwiedz CL, O Donnell CA, Jani BD, Demou E, Ho FK, et al. (2020) Ethnic and socioeconomic differences in SARS-CoV-2 infection: prospective cohort study using UK Biobank. BMC Med 18: 160.
-
Concepción Zavaleta MJ, Coronado Arroyo JC, Zavaleta Gutiérrez FE, Concepción Urteaga LA (2020) Does level of education influence mortality of SARS-CoV-2 in a developing country? International Journal of Epidemiology 49(6): 2091-2093.
-
Oshio T, Kan M (2019) Educational level as a predictor of the incidences of non-communicable diseases among middle-aged Japanese: a hazards-model analysis. BMC Public Health 19: 852.
-
Ayoubkhani D, Nafilyan V, White C, Goldblatt P, Gaughan C, et al. (2021) Ethnic-minority groups in England and Wales-factors associated with the size and timing of elevated COVID-19 mortality: a retrospective cohort study linking census and death records. Int J Epidemiol 49(6): 1951-1962.
-
Luo L, Liao X, Wu X, Jing Q, Zheng J, et al. (2020) Contact settings and risk for transmission in 3410 close contacts of patients with COVID-19 in Guangzhou, China: A prospective cohort study. Ann Intern Med.
-
Frellick M (2020) Risk of Secondary COVID-19 Transmission Low in Most Settings. Medscape.
-
van den Heuvel M (2020) Diesen Artikel so zitieren: Heinsberg-Studie im„ Preprint“: Hohe Dunkelziffer an Infektionen, Sterberate nur 0,36% – gilt das für ganz Deutschland? Medscape; 5 Mai.
-
Turabian JL (2020) Sex and Gender Bio-psychosocial Differences in Coronavirus Disease 2019 (Covid-19): Men have more Biological Problems, but Women Suffer more Long-Term Serious Psychosocial Consequences and with more Implications for Population. J Women’s Health Care 9: 487.
-
Men, sex, gender and COVID-19 (2020) Sex, Gender and Covid-19 Project.
-
Posfay Barbe KM, Wagner N, Gauthey M, Moussaoui D, Loevy N, et al. (2020) COVID-19 in children and the dynamics of infection in families. Pediatrics 146(2): 20201576.
-
Laws RL, Chancey RJ, Rabold EM, Chu VT, Lewis NM, et al. (2020) Symptoms and Transmission of SARS-CoV-2 among Children- Utah and Wisconsin, March–May 2020. Pediatrics 147(1): 2020027268.
-
Li F, Li YY, Liu MJ, Fang LQ, Dean NE, et al. (2021) Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: a retrospective observational study. Lancet Infect Dis 21(5): 617-628.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria