Prevalence and Comparison of Asymptomatic and Symptomatic Patients with SARS-CoV-2 Infection in a General Medicine Office in Toledo, Spain
Background: The number and characteristics of asymptomatic SARS-CoV-2 infections remains questionable. The relationship between domestic and non-domestic contacts remains unclear. Also, some asymptomatic people who test positive for the virus may later develop COVID-19 symptoms. Objective: To compare in general medicine the characteristics of asymptomatic and symptomatic COVID-19 patients. Methodology: Retrospective cohort study of confirmed cases of COVID-19 (positive PCR), from March 15 to November 15, 2020, with asymptomatic patients (without any symptoms or any clinical suspicion of COVID -19, other than potential contact status, at time of test and in the 14 days after the follow-up period) and symptomatic patients (with 2 or more symptoms consistent with COVID -19). Results: 100 patients were included, 77 with symptoms. The prevalence of asymptomatic COVID-19 patients was 23%. Asymptomatic patients vs. symptomatic were younger (mean age of 33.9 vs. 43.9 years; p = .008451), they have more known previous contacts (87% vs. 56%; p
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of coronavirus disease (COVID-19) [1] that has spread rapidly between people. The pandemic has caused more than 64 million confirmed cases and 1.499.841 deaths as of December 3, 2020 [2]. Several features of SARS-CoV-2 make accurate detection during an ongoing epidemic challenging, including high transmissibility, an incubation period with a long-tailed distribution, pre-symptomatic transmission, and the existence of asymptomatic infections, which may also contribute to transmission [3, 4, 5, 6, 7, 8, 9].
One of the many pressing questions surrounding SARS- CoV-2 infections is identifying the determinants of the clinical spectrum, from people with asymptomatic disease to patients with severe COVID-19. Much is still unknown about why there is such a wide range of responses to COVID-19, and it has been claimed that up to 40% of infections may be asymptomatic [10, 11, 12]. Symptom-free transmission makes SARS-CoV-2 much more difficult to fight. Although uncertainty remains about how much they have contributed to the pandemic. Although estimates vary, mathematical models suggest that 30 to 60 percent of the spread occurs when people have no symptoms [13].
Asymptomatic or subclinical SARS-CoV-2 infections are often underreported, meaning that confirmed case counts may not accurately reflect the underlying epidemic dynamics. Understanding the ratio of confirmed symptomatic cases to actual number of symptomatic individuals and undetected epidemic progression is crucial to inform COVID-19 response planning, including the introduction and relaxation of control measures.
Furthermore, the epidemiological and clinical characteristics and immune responses of asymptomatic individuals infected with SARS-CoV-2 have not been well described [14] and consequently a large proportion of infections may go unnoticed [3], with suspicion that infected people, who remain asymptomatic, play an important role in the ongoing pandemic, although its prevalence and effects, the nature of the immune response after natural infection by SARS-CoV-2, the information on the natural history of asymptomatic infection with SARS-CoV-2, as well as the proportion of asymptomatic carriers and risk factors for SARS-CoV-2 transmission among household and non- household contacts remains unclear, and is scarce [10, 15, 16, 17]. A few studies have described the clinical characteristics of asymptomatic patients, however some of these patients were asymptomatic at the time of diagnosis, but developed symptoms later, so they cannot really represent the clinical characteristics of asymptomatic patients [18]. Therefore, it is useful to distinguish between people who are infected and who never develop symptoms (“completely asymptomatic” individuals) and those who have not yet developed symptoms, but do develop them within a few days (presymptomatic).
Ultimately, the number of asymptomatic SARS-CoV-2 infections, in which people do not show any symptoms, remains questionable. Some people who test positive for the virus and don’t feel unwell may develop symptoms later; people can be contagious before they develop symptoms; and data suggests that the virus’s early stages are when most infections are transmitted. The follow-up of infected cases and the tracing of contacts with infected cases is a key tool for health authorities to make public health decisions. In this context, we present a follow-up study of a cohort of positive SARS-CoV-2 cases, with the aim of comparing the characteristics of asymptomatic patients with COVID-19 with symptomatic ones, based on a retrospective analysis, in a General Medicine office, in Toledo (Spain) from March to November 2020.
Material and Methods
In this retrospective cohort study, we analyzed and compared confirmed cases of COVID-19 with positive polymerase chain reaction (PCR), identified in a general practice clinic, among the group of individuals who shared being asymptomatic with that of individuals who presented symptoms of COVID-19, in order to determine the differential characteristics between asymptomatic and symptomatic infected.
Study Location
The study was conducted at a general medicine office in the Santa Maria de Benquerencia Health Center, Toledo, Spain, which has a list of 2,000 patients>= 14 years of age. In Spain, general practitioners (GPs) care for people>=14 years of age, with exceptions requested by the child’s family and accepted by the GP). The study collected data from the patients’ medical records for 8 months, from March 15, 2020 to November 15, 2020.
Diagnosis of COVID-19
The diagnosis of COVID-19 was made by PCR (oropharyngeal). People who were tested
- Patients (clinical diagnosis): people with suspicious symptoms of COVID-19, who went to the GP, or who went to the emergency room of a hospital center and were subsequently followed by the GP.
- Contacts (tracking): people suspected of being infected, belonging to the GP’s patient list, who had close contact with patients positive for COVID-19; This close contact means a space (less than two meters), a time (more than fifteen minutes), a form (without a mask) and an occasion (in the two days before the onset of the patient’s symptoms, or up to eight days from the beginning of these symptoms). Close contact could occur while caring for, living, visiting, or sharing a waiting room or healthcare room with COVID-19 patients, etc.
Because of, since the outbreak began, diagnostic tests were not available at the primary care level, since the instructions were as of March 18, 2020, that diagnostic test for SARS-CoV-2 was performed at people admitted to the hospital, and in respiratory infection of any degree in health personnel. Since May 19, 2020 PCR began to be carried out on suspected COVID-19 cases and contacts in general medicine [19, 20].
In the consultation object of the study, no population screening activity was carried out to detect COVID-19 positive people without symptoms and without suspected contacts. But PCR tests were carried out in asymptomatic people before their incorporation to social health work or hospital admissions or in programmed nursing homes.
Inclusion Criteria
All patients with COVID-19 confirmed with PCR from March 15 to November 15, 2020 who could be followed in their evolution in the consultation object of the study.
Definition of Symptomatic Cases
Anyone with a positive PCR and any combination of two or more symptoms consistent with COVID -19 (fever, cough, dyspnea, myalgia, headache, asthenia, nausea/vomiting, anxiety, insomnia, general malaise, anosmia/ageusia, diarrhea, odynophagia, chest pain, anorexia, rhinorrhea, chilblains, petechiae) at the time of testing, and were tested due to clinical suspicion of COVID -19 [19, 21].
Definition of Asymptomatic Cases
Any patient with positive PCR and absence of relevant clinical symptoms in the 14 days before and after the test. Asymptomatic patients had no symptoms of COVID -19 (as defined above), or any clinical suspicion of COVID -19 (other than potential contact status), at time of test [21]. These definitions were chosen to avoid confusion between true asymptomatic and true symptomatic, as there may be infected people who have a very mild form of the disease, who are paucisymptomatic, and that common symptoms, such as cough, fever or fatigue do not develop noticeably.
Pre-Symptomatic Cases and Longitudinal Follow-Up
Since the incubation period of COVID-19 - the time between exposure to the virus and the appearance of symptoms - can be up to 14 days, it may happen that the PCR positive patient is initially asymptomatic, but symptoms develop in the days successive. In the longitudinal study of the patients, all those who presented 2 or more symptoms in the follow-up were considered as symptomatic cases, regardless of not presenting symptoms initially. This fact can occur in positive cases detected by contact tracing or by screening in certain contexts. The longitudinal study included follow-up throughout the isolation period, so that symptoms could be identified when they appeared.
Sample Size
Considering as exposure factor the known contact with a patient with SARS-CoV-2 infection and a positive PCR, and the result of having or not having symptoms, sample size was calculated for a cross-sectional study/unpaired cohort study, for a Two-sided Confidence Level (1-alpha) of 95, a Power (% probability of detection) of 80, a Ratio of a sample size of 0.5, a Percentage of patients with no exposure (no known contact) of 30%, a Percentage of patients with exposure (with known contact) of 70%.,The Total sample size (Fleiss with continuity correction ) should be 63; 42 with known contact and 21 without known contact [22].
Collected Variables
Data on the index case and close contacts were extracted from the medical records of the general medicine practice under study. The following variables were collected: age, sex, socio-health worker, symptoms, previous contacts, type of contact (family, work, school, social, in a socio-health center, by screening, and others) , and chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment ” [23, 24, 25], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD- 10 Version: 2019 [26].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test, for percentages (according to the number the expected cell totals), and the Student t test for the mean.
Results
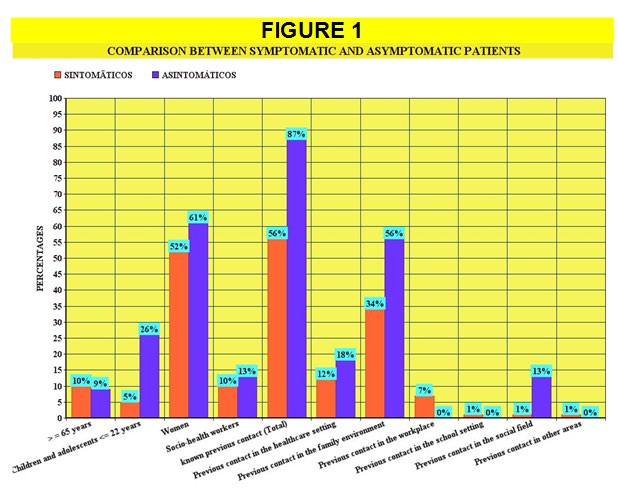
During the study period (from March 15 to November 15) 116 people with positive PCR were detected in the consultation. Following the criteria shown in the methods section, 16 cases presenting a single symptom (for example, only fever, or only cough, or only myalgia, etc.) were excluded from the study. Thus, 100 patients were included, 77 with symptoms and 23 asymptomatic. Thus, the prevalence of asymptomatic COVID-19 patients was 23%. Table 1 And Figure 1 present the distribution of the variables collected in symptomatic and asymptomatic. The only statistically significant differences were that asymptomatic patients were younger (mean age 33.9 vs. 43.9 years; p=.008451), had more known previous contacts (87% vs. 56%; p <.05), and these were They were in a higher proportion of family and social type (56% vs. 34% contacts in the family sphere; p <.05; and 13% vs. 1% contacts in the social sphere; p<.05). 13 of 77 symptomatic patients (17%) tested positive in PCR tests being asymptomatic, but developed symptoms later (presymptomatic), and were finally classified as symptomatic. Therefore, the prevalence of presymptomatic patients on the total of positive cases was 13%. The prevalence of subclinical disease (sum of true and presymptomatic asymptomatic patients) was 36%. In the group of symptomatic cases, 6% were children and adolescents (<= 22 years) vs. 26% in the asymptomatic group (p<.05). There were no differences in the total number of chronic diseases, or in their comparison according to ICD groups.
Discussion
One of the most striking aspects of COVID-19 is the marked differences in experiences of the disease. Some people never develop symptoms, while others, some apparently healthy, have severe or even fatal pneumonia [27]. Asymptomatic cases are not exclusive to COVID-19; they occur with the common flu and probably also appeared in the 1918 pandemic. Many studies have focused on characterizing the heterogeneity of COVID-19 in demographic terms, with clear evidence of higher mortality in men and older people. The adaptive immune system, including B and T cells, has recently been recognized to play a critical role in providing pre-existing immunity to SARS-CoV-2. Consequently, acquired immune responses to previous infections can explain a large percentage of the variability in the presentation of the disease, although doubts remain about additional determinants of the disease, such as pre- existing comorbidities, viral variants, genetic risk factors of the disease host, as well as adaptation or tolerance to infection [28, 29].
The dominant scientific view of asymptomatic patients is that their immune systems are especially well tuned. This could explain why children and young adults make up the majority of people without symptoms because the immune system naturally deteriorates with age. It is also possible that the immune system of the asymptomatic has been primed by a previous infection with a milder coronavirus, such as those that cause the common cold.
Furthermore, the transmission of SARS-CoV-2 from asymptomatic or presymptomatic people complicates public health measures aimed at controlling the pandemic. Consequently, symptomatic and asymptomatic cases must be studied separately to understand the dynamics of infection [30]. While current data suggest that asymptomatic people can transmit SARS-CoV-2, the relative contribution of asymptomatic people to the spread of SARS-CoV-2 remains an area of controversy. Previous reports have indicated that low values for the number of cycles required to detect the virus (Ct), indicating higher levels of virus, can occur in presymptomatic and asymptomatic patients. While many factors beyond viral load can contribute to infectivity, viral loads have been reported to be similar between asymptomatic and symptomatic (including presymptomatic) patients. Furthermore, viral loads tend to decrease more slowly in asymptomatic patients [31, 32, 33].
Asymptomatic individuals have been reported to have a weaker immune response to SARS-CoV-2 infection. But, asymptomatic individuals probably have effective cellular immunity that destroys the intracellular virus, although there is no robust antibody response to neutralize SARS- CoV-2 on the mucosal surface, when the virus enters the respiratory tract or stream blood. Therefore, relying solely on SARS-CoV-2 antibodies as proof of the prevalence of immunity runs counter to the fundamental principles of viral immunology [34].
Prevalence of Asymptomatic Patients
The reported data of asymptomatic infection vary widely. About 81% of COVID-19 infections detected on a cruise ship were asymptomatic [35]. In a study in Marine recruits, 90% of those who were positive reported having no symptoms [36]. In an outbreak of COVID-19 occurred on the U.S.S. Theodore Roosevelt, 43% of those who tested positive for the virus never had symptoms [37]. Data on COVID-19 transmission on the Diamond Princess ship, with more than 3,700 people on board, showed that 18% of the positive cases were “true asymptomatic” (people who never developed symptoms despite being infected) [38]. In South Korea of 91 children who were monitored for the course of confirmed COVID-19 disease, 22% never developed any symptoms [39]. Another study showed that 20.8% of patients had asymptomatic infections. He et al, in the series of 206 hospital cases found a prevalence of subclinical infection of 5.8% [40]. A 3.6% rate of asymptomatic carriers of SARS-CoV-2 has been reported in an asymptomatic surgical population [41]. In Massachusetts grocery store workers, three-quarters of those who tested positive were asymptomatic when tested [42].
In a study that analyzed almost a hundred studies on this subject, it was estimated that the number of patients who did not develop symptoms during the entire infection was around 20%, with a wide range that ranged from 3 to 67%; if the population bias is analyzed, the percentage of asymptomatic patients rose to 31%. These data are not far from what seroprevalence studies say: one third of patients do not develop symptoms [42]. On the other hand, another review, of more than 2,500 studies, found percentages of asymptomatic patients between 4 and 41%, and concluded that the real figure was between 14 and 20% [43].
Other reviews, however, place the figure between 40 and 50% of patients. Furthermore, the absence of COVID-19 symptoms in people infected with SARS-CoV-2 does not necessarily imply the absence of harm. Asymptomatic infection can be associated with slight changes in biochemical and inflammatory variables and subclinical pulmonary abnormalities can occur, detected by computed tomography [10, 12]. In our study, where as in other studies, asymptomatic cases came mainly from investigations of contacts of confirmed cases [44, 45]. Our results of 23% of true asymptomatic coincide with the figures that are admitted as more real.
Prevalence of Presymptomatic Patients
It has been stated that the majority of asymptomatic patients should be considered presymptomatic. Thus, it is postulated that only a minority of people with SARS-CoV-2 (approximately 20%) have a truly asymptomatic infection; most SARS-CoV-2 patients who are asymptomatic at the time of testing will develop symptoms later [46]. Of course, the difficulty of distinguishing asymptomatic people from those who are simply presymptomatic is an obstacle. The simple solution to this difficulty is longitudinal monitoring of the individual over time.
Data from the few cohort studies with longitudinal reports suggest that a small fraction of asymptomatic people may eventually develop symptoms. In the Italian and Japanese cohorts, 0% of the asymptomatic people became symptomatic. In the Greece and New York cohorts, 10.3% of asymptomatic people became symptomatic. In another study in Korea, 19% of asymptomatic patients eventually developed symptoms [31]. In an outbreak of COVID-19 occurred on the U.S.S. Theodore Roosevelt, 30.5% were presymptomatic at the time they tested positive [37]. But, in a skilled nursing facility, 89% of initially asymptomatic patients became ill. A conservative estimate of all these data would be that of a prevalence of 30% or more for the mixture of presymptomatic and true asymptomatic.
Our study that took into account the aspect of longitudinally monitoring a cohort of patients, found a prevalence of presymptomatic patients of 13%, and the prevalence of subclinical disease (sum of true and presymptomatic asymptomatic patients) was 36%. These data are in line with the studies discussed previously.
Known Contacts Vs. Unknown
It has been reported that 50% of all cases do not know how they have contracted the virus; that is, they do not have any known contact that is positive and that could have transmitted SARS-CoV-2, and this percentage is probably related to the lack of contact tracing [47, 48]. One model estimated that undocumented infections were the source of 79% of cases [49]. However, the most likely source of asymptomatic infections are close contacts of patients who have been diagnosed, predominantly in the family groups; additionally, colleagues, friends, and individuals who match the trajectories of diagnosed or suspected patients are considered high-risk populations. Thus, among those who reported close contact with an infected person, that person is often a family member (45% of cases) or a co-worker (34%) [16, 42, 48, 50, 51].
In our study, asymptomatic patients reported known previous contact in 87% (vs. 56% in symptomatic patients; p <.05.). Therefore only 13% of the asymptomatic (and 44% of the symptomatic) did not know how they had contracted the virus. These known previous contacts were predominantly in the family, health and social environment in the asymptomatic, and in the family, health and work environment in the symptomatic; but the differences were only statistically significant in the family environment (where more than half of the contacts occurred) and social field for the Asymptomatic. Basically, these data are in line with what was reported: the asymptomatic ones were family contacts.
Characteristics of Asymptomatic Vs. Symptomatic Patients
Our study shows that asymptomatic infections were more frequent in younger individuals (mean age of 34 years in asymptomatic patients vs 44 years in symptomatic patients; p <.05.), And more in women (61% asymptomatic women vs 52% women with symptoms) .Therefore, these data follow what has been shown in other studies: that asymptomatic infections are more common in populations of young individuals (and specifically, women with frequencies between 60-70% are even more likely than men not to show signs of the disease), and in middle age (average age according to different studies, between 26 and 49 years). Age can play an important role in the severity of COVID-19, and this is related to different immune responses [10, 50, 52, 53].
Regarding children and adolescents (which includes variable ages: 0-22 years in some study; 3-18 years in others, etc.), it has been reported that they can develop COVID-19 and can be a potential source of contagion of the SARS-CoV-2, although most remain asymptomatic or experience mild illness [54, 55]. The prevalence of asymptomatic children and adolescents remains controversial. In a UK study of children 2 to 15 years of age, up to 50% of infected children did not develop symptoms [56]. But in another study where children without symptoms of COVID-19 underwent PCR testing before surgery, clinic visits, or hospital admissions, the overall prevalence of positives was 0.65% [57]. And it has been suggested that the prevalence of asymptomatic infections in children correlates with the overall incidence of COVID-19 in the local population. We found 6% of children and adolescents <=22 years among the symptomatic ones and 26% among the asymptomatic ones (Table 1, Figure 1).
| Symptomatic Patients N=77 | Asymptomatic Patients N=23 | Statistical Significance | |
|---|---|---|---|
| Age in years (arithmetic mean and standard deviation) | 43.9+-16.6 | 33.9+-19.2 | T-value=2.43036; p=.008451. Significant at p<.05. |
| >=65 years | 8 (10) | 2 (9) | Fisher exact test=1. NS at p<.05. |
| Children and adolescents <=22 years | 5 (6) | 6 (26) | Fisher exact tes=0.0167. p<.05. |
| Women | 40 (52) | 14 (61) | X2=0.5675. p=.451265.NS |
| Socio-health workers | 8 (10) | 3 (13) | Fisher exact test=0.7118. NS |
| Total known previous contact | 43 (56) | 20 (87) | X2=7.3543. p=.00669. p<.05. |
| Previous contact in the healthcare setting | 9 (12) | 4 (18) | X2 with Yates correction=0.1299. p=.718582. NS |
| Previous contact known in the family environment | 26 (34) | 13 (56) | X2=3.8548. p=.049605. p<.05. |
| Previous contact in the workplace | 5 (7) | 0 | Fisher exact test=0.5866. NS |
| Previous contact known in the school setting | 1 (1) | 0 | Fisher exact test=1. NS |
| Previous contact known in the social field | 1 (1) | 3 (13) | Fisher exact test=0.037. p<.05. |
| Previous contact known in other areas | 1 (1) | 0 | Fisher exact test=1. NS |
| PCR test carried out by screening (before hospital admission, before reincorporation to social health work, etc.) | 0 | 3 (13) | NA |
| PCR test performed by symptoms | 64 (83) | 0 | NA |
| Presymptomatic patients (Initially asymptomatic patients in whom symptoms appear after positive PCR performed by known contact) | 13 (17) | 0 | NA |
Table 1: Comparison between Symptomatic and Asymptomatic Patients.
One of the most concerning aspects of COVID-19 is the risk of infection among front-line healthcare workers. In a large UK university hospital, 3% of its workers tested positive for SARS-CoV-2 [58]. In Spain, health workers comprise 24% of all confirmed COVID-19 cases, a proportion that is explained by the lack of protective equipment and organization in the first wave, and in part by greater access to PCR tests in the second wave [42, 59]. Our study finds a frequency of symptomatic infection in social-health workers of 10%, and 13% in asymptomatic; in this second population, routine screening was performed in certain situations (such as return to work after vacation or routine screening). These health professional screenings are probably necessary to provide maximum protection for both this population at risk and the patients they serve.
Regarding the role of comorbidities, our study did not find statistically significant differences between asymptomatic and symptomatic patients, neither by their total number, nor by groups of diseases (Table 2). The proportion of asymptomatic or presymptomatic infections in the population with medical comorbidities and an increased risk of severe disease are unclear. A study showed that 40% of skilled nursing facility SARS-CoV-2 infections were asymptomatic; a relatively high proportion of asymptomatic infections in a population expected to have multiple risk factors for severe COVID-19 [60].
| Symptomatic Patients N=77 | Asymptomatic Patients N=23 | Statistical Significance | |
|---|---|---|---|
| Average Number Of Chronic Diseases Per Patient | 1.2+-1.6 | 0.9+-1.7 | T= 1.04998. P= .148154. NS |
| -II Neoplasms | 1 (1) | 2 (10) | Fisher Exact Test = 0.0817. NS |
| -II Diseases Of The Blood | 1 (1) | 0 | Fisher Exact Test= 1. NS |
| -IV Endocrine | 23 (25) | 3 (15) | X2 With Yates Correction= 0.446. P= .504234. NS |
| -V Mental | 10 (11) | 1 (5) | Fisher Exact Test= 0.6855. NS |
| -VI-VIII Nervous And Senses | 6 (6) | 3 (15) | Fisher Exact Test= 0.2001. NS |
| -IX Circulatory System | 14 (15) | 2 (10) | Fisher Exact Test= 0.7325. NS |
| -X Respiratory System | 10 (11) | 2 (10) | Fisher Exact Test = 1. NS |
| -XI Digestive System | 9 (10) | 2 (10) | Fisher Exact Test= 1. NS |
| -XII Diseases Of The Skin | 3 (3) | 0 | Fisher Exact Test = 1. NS |
| -XIII Musculo-Skeletal | 7 (8) | 3 (15) | Fisher Exact Test= 0.3805. NS |
| -XIV Genitourinary | 8 (9) | 2 (10) | Fisher Exact Test= 1. NS |
| Total=112 Chronic Diseases* | 92 (100) | 20 (100) | - |
Table 2: Comparison of Chronic Diseases between Symptomatic and Asymptomatic Patients.
Limitations and Strengths of the Study
- The study has the strength of its longitudinality, characteristic of work in general medicine [61], together with the difficulty of following patients throughout the disease to verify that they do not developed symptoms.
- It has the limitations of being a retrospective design, and that the symptom expression data depend on the individual’s own ability to detect their infection. A recent publication noted that half of the British respondents were unable to identify the key symptoms of COVID-19 (fever, cough, and loss of smell and taste) [62]. For all this, some researchers consider the term asymptomatic problematic. When it is said that there are 40% asymptomatic, it actually means that there are 40% of people with an infection mild enough so that they do not indicate any symptoms to their doctor; it is perhaps a minor distinction, but an important one.
- The limitations of the PCR test (oropharyngeal). It is the test that is considered gold-standard; it is based on the determination of the RNA of the nucleocapsid. If there are fragments of the SARS-CoV-2 RNA, they replicate as many times as necessary to give a result. If the viral load is high, few Ct are required, less than twenty. If there is little viral nucleic material, 35 and 40 Ct may be required. But, it even tests positive if the viral quantity is irrelevant and the patient can no longer infect. That is to say, it can give false positives, in the sense of giving positive certain because there is materially SARS-CoV-2 nucleic acid but that such presence is irrelevant because it is so small that it cannot infect [46, 63]. On the other hand, positivity depends on the presence of enough viruses to trigger a positive test, which may depend on the test site and timing. Strength of the study was the fact that it was based on the routine assistance of the GP, so that patients were seen in the first days of the onset of symptoms. The highest percentage of virus detection (89%) has been reported to be nasopharyngeal sampling between 0 and 4 days after the onset of symptoms, decreasing to 54% after 10 to 14 days [64].
In addition, the proportion of asymptomatic infections could be even higher, as the PCR test could miss some cases. Cases of patients with SARS-CoV-2 infection with negative PCR results and no symptoms have been reported using an antibody test. Therefore, PCR and appropriate serological tests should probably be used in conjunction, for an accurate estimate of the proportion asymptomatic. However, serological tests have limitations and vary in their specificity and sensitivity. Furthermore, their results may also be confounded by previously existing antibodies against SARS- CoV, MERS-CoV, or the common cold coronaviruses [65, 66, 67].
Conclusion
The true burden of asymptomatic disease is not yet known, but it is emerging as both PCR and antibody tests to establish seroprevalence have become more available. In the context of general medicine in Toledo (Spain), during March-November 2020, we found a prevalence of asymptomatic patients of 23% and of subclinical disease (sum of true and presymptomatic asymptomatic patients) of 36%. Being an asymptomatic COVID-19 patient vs. symptomatic, it was associated with being younger and having more exposure to known contacts, mainly family and social. Even though the symptomatic-asymptomatic dichotomy is actually false; Forgets very mild patients, who have not yet developed symptoms or who are unable to report them. However, its study is essential to understand the transmission of the coronavirus and thus establish more effective measures against the pandemic. In any case, the contribution of presymptomatic and asymptomatic infections to transmission implies that combined prevention measures (hand hygiene, masks, testing, tracking, isolation and distancing) will continue to be necessary in the future. The focus of testing programs for SARS-CoV-2 should be expanded substantially to include people who do not have symptoms of COVID-19. This would be especially justified in all household contacts of young people.
References
-
(2020) Naming the coronavirus disease (COVID-19) and the virus that causes it. WHO.
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
Russell TW, Golding N, Hellewell J, Abbott S, Wright L, et al. (2020) Reconstructing the early global dynamics of under-ascertained COVID-19 cases and infections. BMC Med 18: 332.
-
Abbott S, Hellewell J, Munday J, Funk S (2020) The transmissibility of novel Coronavirus in the early stages of the 2019–20 outbreak in Wuhan: Exploring initial point-source exposure sizes and durations using scenario analysis. Wellcome Open Res 5: 17.
-
Tindale L, Coombe M, Stockdale JE, Garlock E, Lau WYV, et al. (2020) Transmission interval estimates suggest pre-symptomatic spread of COVID-19. MedRxiv.
-
Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, et al. (2020) Early dynamics of transmission and control of COVID-19: a mathematical modelling study. Lancet Infect Dis 20(5): 553-558.
-
Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI, et al. (2020) Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health 8(4): 488-496.
-
Bai Y, Yao L, Wei T, Tian F, Jin DY, et al. (2020) Presumed asymptomatic carrier transmission of COVID-19. JAMA 323(14): 1406-1407.
-
Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, et al. (2020) The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med 172(9): 577-582.
-
Oran DP, Topol EJ (2020) Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann Intern Med 173: 362-367.
-
Warren EL (2020) Why Do Some People Weather Coronavirus Infection Unscathed?. Medscape.
-
Pan Y, Yu X, Du X, Li Q, Li X, et al. (2020) Epidemiological and Clinical Characteristics of 26 Asymptomatic Severe Acute Respiratory Syndrome Coronavirus 2 Carriers. J Infect Dis 221(12): 1940-1947.
-
Apuzzo M, Gebrekidan S, Kirkpatrick DD (2020) How the World Missed Covid-19’s Silent Spread. Symptomless transmission makes the coronavirus far harder to fight. But health officials dismissed the risk for months, pushing misleading and contradictory claims in the face of mounting evidence. New York Times.
-
Long Q, Tang X, Shi Q, Li Q, Deng HJ, et al. (2020) Clinical and immunological assessment of asymptomatic SARS- CoV-2 infections. Nat Med 26: 1200-1204.
-
Saad Roy CM, Wagner CE, Baker RE, Morris SE, Farrar J, et al. (2020) Immune life history, vaccination, and the dynamics of SARS-CoV-2 over the next 5 years. Science 370(6518): 811-818.
-
Sakurai A, Kato S, Hayashi M, Ishihara T, Iwata M, et al. (2020) Natural History of Asymptomatic SARS-CoV-2 Infection. N Engl J Med 383: 885-886.
-
Ng OY, Marimuthu K, Koh V, Pang J, Linn KZ, et al. (2020) SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: a retrospective cohort study. Lancet Infect Dis.
-
Guan WJ, Ni ZY, Hu Yu, Liang WH, Ou CQ, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 382: 1708-1720.
-
Turabian JL (2020) Micro-Impact of the Pandemic by Covid-19 in the General Medicine: Clinical and Epidemiological Reflections from the Situation in Spain March 2020. Epidemol Int J 4(2): 1-11.
-
Turabian JL (2020) Polymerase Chain Reaction Positivity Rate for Covid-19 in General Medicine in Toledo (Spain) from May 19 to September 30, 2020. Is it Re-Outbreak, Second Wave of Virus or Lack of Testing?. Epidemol Int J 4(2): 1-11.
-
Kociolek LK, Muller WJ, Yee R, Bard JD, Brown CA, et al. (2020) Comparison of upper respiratory viral load distributions in asymptomatic and symptomatic children diagnosed with SARS-CoV-2 infection in pediatric hospital testing programs. J Clin Microbiol 59(1): 1-12.
-
Open Source Epidemiologic Statistics for Public Health.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The C.V. Mosby Company.
-
Gill M (2017) Augmented care: An alternative model of care for people with chronic disease. Int J Care Coord 20(1-2): 5-7.
-
Larrañaga AC, Vetrano DL, Onder G, Feliu LAG, Santaliestra CC, et al. (2016) Assessing and Measuring Chronic Multimorbidity in the Older Population: A Proposal for Its Operationalization. J Gerontol A Biol Sci Med 72(10): 1417-1423.
-
(2019) International Statistical Classification of Diseases and Health-Related Problems. WHO.
-
Callaway E, Ledford H, Mallapaty S (2020) Six months of coronavirus: the mysteries scientists are still racing to solve. Nature.
-
Beck DB, Aksentijevich I (2020) Susceptibility to severe COVID-19. Science 370(6515): 404-405.
-
Young BE, Fong SW, Chan YH, Mak TM, Ang LW, et al. (2020) Effects of a major deletion in the SARS- CoV-2 genome on the severity of infection and the inflammatory response: An observational cohort study. Lancet 396(10251): 603-611.
-
Mahase E (2020) Covid-19: the problems with case counting. BMJ 370: 3374.
-
Lee S, Kim T, Lee E, Lee C, Kim H, et al. (2020) Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern Med 180(11): 1447-1452.
-
Stadnytskyi V, Bax CE, Bax A, Anfinrud P (2020) The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc Natl Acad Sci USA 117(12): 11875-11877.
-
Laurie Barclay (2020) COVID-19: What Is the Primary Route of Transmission?. Medscape.
-
Thukalan PG (2020) SARS-CoV-2 seroprevalence in Spain. Lancet 396(10261): 1484.
-
Ing AJ, Cocks C, Green JP (2020) COVID-19: in the footsteps of Ernest Shackleton. Thorax.
-
Letizia AG, Ramos I, Obla A, Goforth C, Weir DL, et al. (2020) SARS-CoV-2 Transmission among Marine Recruits during Quarantine. N Engl J Med 383: 2407- 2416.
-
Kasper MR, Geibe JR, Sears CL, Riegodedios AJ, Luse T, et al. (2020) An Outbreak of Covid-19 on an Aircraft Carrier. N Engl J Med 383: 2417-2426.
-
Baraniuk C (2020) What the Diamond Princess taught the world about covid-19. BMJ 369: 1632.
-
Han MS, Choi EH, Chang SH, Jin BL, Lee EJ, et al. Clinical Characteristics and Viral RNA Detection in Children with Coronavirus Disease 2019 in the Republic of Korea. JAMA Pediatr.
-
He G, Sun W, Fang P, Huang J, Gamber M, et al. (2020) The clinical feature of silent infections of novel coronavirus infection (COVID-19) in Wenzhou. J Med Virol 92(10): 1761-1763.
-
Bloom JA, Erlichman Z, Tian T, Doron S, Chen L, et al. (2020) The prevalence of asymptomatic carriers of COVID-19 as determined by routine preoperative testing. J Infect Prev.
-
Lan F, Suharlim C, Kales SN, Yang J (2020) Association between SARS-CoV-2 infection, exposure risk and mental health among a cohort of essential retail workers in the USA. Occup Environ Med.
-
Garcia DB, Gany DE, Counotte MJ, Hossmann S, Imeri H, et al. (2020) Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. Plos Medicine.
-
Pollán M, Gómez BP, Barriuso RP, Oteo J, Hernan MA, et al. (2020) Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet 396(10250): 535-544.
-
Byambasuren O, Cardona M, Bell K, Clark J, Mclaws ML, et al. (2020) Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: systematic review and meta-analysis. MedRxiv.
-
(2020) The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID- 19)-China, 2020. China CDC Weekly.
-
Acción BC, Vallés MJ, Valiñas LP, Riobóo JP, Pego YT (2020) Role of asymptomatic infected people in the transmission of the SARS-cov-2 coronavirus. Galician Health Service.
-
Mc Namara D (2020) About 80% of Asymptomatic People WithCOVID-19 Develop Symptoms, Medscape.
-
(2020) Report No. 35. Situation of COVID-19 in Spain. Cases diagnosed as of May 10 COVID-19 Report.
-
Tenforde MW, Rose EB, Lindsell CJ, Shapiro NI, Files DC, et al. (2020) Characteristics of Adult Outpatients and Inpatients with COVID-19-11 Academic Medical Centers, United States, March-May 2020. MMWR Morb Mortal Wkly Rep 69(26): 841-846.
-
Slifka MK, Gao L (2020) Is presymptomatic spread a major contributor to COVID-19 transmission? Nat Med 26: 1531-1533.
-
Gao Z, Xu Y, Sun C, Wang X, Guo Y, et al. (2020) A Systematic Review of Asymptomatic Infections with COVID-19. J Microbiol Immunol Infect.
-
Anderson BD, Wang GL, Yao L, Li CB, Lei J, et al. (2020) Transmission Potential of Asymptomatic and Paucisymptomatic Severe Acute Respiratory Syndrome Coronavirus 2 Infections: A 3-Family Cluster Study in China. J Infect Dis 221(12): 1948-1952.
-
Yang R, Gui X, Xiong Y (2020) Comparison of Clinical Characteristics of Patients with Asymptomatic vs Symptomatic Coronavirus Disease 2019 in Wuhan, China. JAMA Netw Open 3(5): 2010182.
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Yonker LM, Neilan AM, Bartsch Y, Alter G, Li JZ, et al. (2020) Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J Pediatr 227: 45-52.
-
Lordan R, FitzGerald GA, Grosser T (2020) Reopening schools during COVID-19. Science 369(6508): 1146.
-
Waterfield T, Watson C, Moore R, Ferris K, Tonry C, et al. (2020) Seroprevalence of SARS-CoV-2 antibodies in children - A prospective multicentre cohort study. MedRxiv.
-
Sola AM, David AP, Rosbe KW, Baba A, Avila LR, et al. (2020) Prevalence of SARS-CoV-2 Infection in Children without Symptoms of Coronavirus Disease 2019. JAMA Pediatr.
-
Rivett L, Sridhar S, Sparkes D, Jones NK, Forrest S, et al. (2020) Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. Elife 9: 58728.
-
Turabian JL (2020) The Epidemiological Hypothesis of “The Trojan Horse”: Were Hospitals The Main Vectors Of The Exponencial Beginning Of Coronavirus Disease 2019 (Covid-19) In Spain And Other Countries? Epidemol Int J 4(3): 1-6.
-
White EM, Santostefano CM, Feifer RA, Kosar CM, Blackman C, et al. (2020) Asymptomatic and presymptomatic severe acute respiratory syndrome coronavirus 2 infection rates in a multistate sample of skilled nursing facilities. JAMA Intern Med 180(12): 1709-1711.
-
Turabian JL (2020) Epidemiological Value of Continuity of Care in General Medicine (Part Two). Epidemol Int J 4(1): 000138.
-
Smith LE, Potts HWW, Amlot R, Fear NT, Michie S, et al. (2020) Adherence to the test, trace and isolate system: results from a time series of 21 nationally representative surveys in the UK (the COVID-19 Rapid Survey of Adherence to Interventions and Responses [CORSAIR] study. MedRxiv.
-
Gérvas J, Fernández MP (2020) Antigen tests for the new coronavirus: BPR (Cheap, Accurate and Rapid if used properly). Salud, dinero y atención primaria.
-
Mallett S, Allen AJ, Graziadio S, Taylor SA, Sakai NS, et al. (2020) At what times during infection is SARS-CoV-2 detectable and no longer detectable using RT-PCR-based tests? A systematic review of individual participant data. BMC Med 18: 346.
-
Metcalf CJE, Farrar J, Cutts FT, Basta NE , Graham AL, et al. (2016) Use of serological surveys to generate key insights into the changing global landscape of infectious disease. Lancet 388(10045): 728-730.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria