Hematological Complications in Pregnancy: A Comprehensive Review
Hematological questions before birth pose important risks to both motherly and before-birth fitness, necessitating appropriate acknowledgment and appropriate management. This review checks the range of hematological snags attacked in gestation, including anemia, thrombocytopenia, and coagulopathies. Anemia, a prevailing condition, can become functional iron inadequacy, folate inadequacy, or hemoglobinopathies, and allure impact extends further motherly well-being to influence gestation effects and neonatal fitness. Thrombocytopenia, characterized by depressed platelet counts, presents challenges in gestation on account of the risk of obstetric draining and neonatal thrombocytopenia. Coagulopathies, including disorders like von Willebrand ailment and thrombophilia, heighten the risk of thromboembolic occurrences and obstetric confusion. Effective administration of hematological disorders in gestation depends on a multidisciplinary approach including obstetricians, hematologists, and neonatologists. Strategies involve tailor-made supplementation for lifelessness, close monitoring of platelet counts, and anticoagulant treatment for thrombotic disorders. However, management resolutions must balance the risks and benefits of mediation to minimize harm to both parents and fetus. Furthermore, this review argues for the significance of the assumption of enjoining and hiding hematological disorders to improve maternal fitness before gestation. Additionally, it stresses the meaning of postpartum care in detecting and directing determined hematological abnormalities. In conclusion, understanding haematological confusion in gestation is critical for guaranteeing optimum maternal and before-birth effects. Further research is authorized to perfect demonstrative approaches, healing strategies, and directions for directing these complex environments before birth.
Introduction
Anemia
Normochromic, normocytic anemia concedes the possibility of happening from the 7th to 8th week of incubation, on account of the corporeal increase in plasma book, that is to say, rather more the increase in red cell bulk. However, the haemoglobin (Hb) endure not fall to <11 g/ dl in the first, or <10 g/dl in the second and after-second trimesters [1, 2]. More marked anemia may develop iron, folate, or more exceptionally, a source of nourishment B12 deficiency or hemoglobinopathies.
Hematinic Requirement
Pregnancy demands an iron consumption of about 2.5 mg/day during the whole of, possibly 3.0–7.5 mg/day necessary in the after the second trimester. An average Western diet provides around 250 µg/epoch of folate; still, necessities increase to about 400 µg/day before birth [3], accompanying imperfection most commonly on account of a lack of folate-rich herbs specific as vegetables and peas, which is frequently connected to social deprivation. Folate imperfection is more average in diversified pregnancy, frequent childbirth, and adolescent mothers.
The material stores about 3 mg of B12, accompanying an often-dietary requirement of 3 g/epoch. The only B12 beginning is animal foods; thus, vegetarians and vegans are depressed and at risk of poor nutrition.
The Effect of Deficiency
The signs and symptoms of early imperfections are non- distinguishing, containing tiredness and lineaments of some basic cause (Table 1). Aside from anemia, folate and B12 deficiency is connected to affecting animate nerve organs and hose defects [4, 5]. The effect of iron inadequacy (before anemia) on maternal and before-birth prosperity is not completely understood, but gentle deficiency is connected to raised delivery draining and weak before-birth iron stores and an increased amniotic sac: unborn young pressure ratio [6]. Severe motherly iron inadequacy is a guide to pre-mature transmittal and depressed birthweight [1], even though this may have a connection with the latent cause. Most issues accompanying folate deficiency are labeled remotely on account of a raised cell with hemoglobin Mean Cell Volume (MCV), but folate deficiency anemia frequently coexists with iron deficiency and more frequently presents at the end of gestation or in the early puerperium. B12 deficiency can again result in demyelinating neuropathy, even though gentle maternal B12 inadequacy performs agreeably with sane gestation [7]. Diagnosis of imperfection As the MCV may increase accompanying common reproduction, the decline in MCV usually visualized in iron inadequacy is not trustworthy in pregnancy. Serum iron, Total Iron Binding Capacity (TIBC), ferritin, antitoxin transferrin receptor levels, and cells with hemoglobin-derivative Protoporphyria can be used to pronounce iron inadequacy. However, rational gestation leads to a progressive approach to antitoxin iron, ferritin, and an increase in TIBC, free Protoporphyria, and transferrin receptor levels [8]. Thus, any of the limits may be proper to pronounce temperate imperfection, although a considerably discounted antitoxin ferritin (<12 ug/l) remnants diagnostic. Megaloblastic anemia from B12 or folate deficiency is submitted by an MCV >100 fl, accompanying right-switched neutrophils on the ancestry film (Table 2). Serum folate is sensitive to imperfection but concedes the possibility of being deprived of accompanying very recent abstinence from food folate lack and further reductions in gestation [9]. Red cell folate levels are less touched by recent diet but concede the possibility of a rise in alternatively common gestation [10, 11]. If necessary, megaloblastic erythropoiesis can be manifested by a cartilage essence test. Serum B12 levels may approach 30–50% of the time is rational gestation, but this is probably not a real fabric inadequacy [7]. Specific tests to pronounce intrinsic determinant imperfection (from bad anemia) include radioisotope exposure and are contraindicated in pregnancy, but body tissue basic determinant antibodies, if present, can point to a disease called pernicious anemia.
| Deficiency | Causes |
| Iron | Inadequate dietary intake, especially in individuals with poor nutrition or restrictive diets |
| Iron | Increased iron requirements during pregnancy and lactation |
| Iron | Blood loss due to menstruation, gastrointestinal bleeding, or other pathological conditions |
| Iron | Impaired absorption, such as in celiac disease, inflammatory bowel disease, or gastric bypass surgery |
| Folate | Inadequate dietary intake, particularly in individuals with poor nutrition or alcoholism |
| Folate | Increased folate requirements during pregnancy to support fetal neural tube development |
| Folate | Malabsorption syndromes such as celiac disease, Crohn’s disease, or tropical sprue |
| Folate | Medications like methotrexate, sulfasalazine, or anticonvulsants that interfere with folate metabolism |
| Vitamin B12 | Inadequate dietary intake, especially in vegetarians or individuals with poor nutrition |
| Vitamin B12 | Impaired absorption due to pernicious anemia, atrophic gastritis, or surgical resection of the stomach |
| Vitamin B12 | Intestinal malabsorption disorders such as Crohn’s disease, celiac disease, or pancreatic insufficiency |
| Vitamin B12 | Use of medications like proton pump inhibitors, metformin, or certain anticonvulsants |
| Condition | Description |
| Megaloblastic Anemia | Characterized by enlarged, immature red blood cells (megaloblasts) due to impaired DNA synthesis |
| Megaloblastic Anemia | Commonly caused by deficiency of vitamin B12 or folate, leading to ineffective erythropoiesis |
| Megaloblastic Anemia | May also result from medications like methotrexate or certain chemotherapeutic agents |
| Megaloblastic Anemia | Peripheral blood smear typically shows macrocytic red blood cells with hypersegmented neutrophils |
| Megaloblastic Anemia | Elevated MCV (>100 fL) is a hallmark feature of megaloblastic anemia |
| Liver Disease | Chronic liver diseases such as cirrhosis can lead to impaired hepatic synthesis of proteins, including those involved in red blood cell production |
| Liver Disease | Alcohol-related liver disease and non-alcoholic fatty liver disease are common causes of liver dysfunction |
| Liver Disease | Elevated MCV may be observed due to alcohol-induced macrocytosis |
| Hypothyroidism | Thyroid hormone deficiency can result in decreased metabolism and impaired erythrocyte maturation |
| Hypothyroidism | Anemia associated with hypothyroidism is often normochromic and normocytic, but an elevated MCV may be present due to reduced red blood cell turnover |
| Hypothyroidism | Thyroid function tests (TFTs) including TSH and free T4 levels aid in diagnosing hypothyroidism |
| Hemolysis | Increased red blood cell destruction can lead to compensatory erythropoiesis and elevated MCV |
| Hemolysis | Hemolytic anemias may be inherited (e.g., hereditary spherocytosis) or acquired (e.g., autoimmune hemolytic anemia) |
| Hemolysis | Laboratory findings may include elevated reticulocyte count, unconjugated hyperbilirubinemia, and peripheral blood smear abnormalities |
| Alcoholism | Chronic alcohol consumption can impair bone marrow function and lead to macrocytosis |
| Alcoholism | Alcohol-induced macrocytosis is typically reversible upon cessation of alcohol intake |
| Alcoholism | Associated with other alcohol-related complications such as liver disease and nutritional deficiencies |
| Myelodysplastic Syndrome (MDS) | A group of clonal hematopoietic disorders characterized by ineffective hematopoiesis |
| Myelodysplastic Syndrome (MDS) | MDS can present with macrocytic anemia and cytopenias, and is associated with an increased risk of leukemia |
| Myelodysplastic Syndrome (MDS) | Bone marrow biopsy and cytogenetic analysis are essential for diagnosing MDS and assessing prognosis |
Table 2: Differential Diagnosis of a Raised Mean Corpuscular Volume (MCV).
Prophylaxis
The Hb aggregation is frequently used to screen for hemotinic imperfection, accompanying an assessment of performance and repeated in the early tertiary trimester. Whether routine iron supplementation is authorized but not resolved, as it is not clear whether the blastula benefits [1]. If necessary, bendable mentation can be completed, accompanying 30–60 mg of iron per epoch. which produces few side effects. Side effects are chiefly visualized accompanying substitute (200 mg/day) remedy. Furthermore, supplementation in addition to 200 mg/ day will not produce earlier-normal hemoglobin (Hb) or hematocrit (HCT). To prevent affecting animate nerve organs’ hose defects, folic acid bendable mentation (at 400µ g/era) is routinely likely in the first drugs that antagonize folate metabolism or in those with likely dietary deficiency.
Treatment
The treatment of established iron deficiency is 200 mg/ day of elemental iron. This may lead to gastrointestinal upset, which can be product-related and is usually ameliorated by either dose reduction or (100 mg/day), or a change in the preparation. Iron absorption is maximized when combined with ascorbic acid, such as as taking iron supplements with fresh orange juice or a vitamin C preparation. Therapy failure occurs in malabsorption and when loss exceeds intake, but is most commonly due to poor compliance. There are also liquid oral iron preparations and parenteral therapy. Parenteral therapy is useful in malabsorption and failed compliance. But otherwise does not produce a faster response than oral iron, and side effects are common.
Proven Folate Deficiency
Anemia should be treated with folic acid (5 mg/day).In all such cases of anemia, B12 deficiency must also be excluded, as folate may improve the anemia of B12 efficiency but exacerbate any associated neurological deterioration [12]. In B12 deficiency, a single dose of 1000 µg of intramuscular B12 should lead to a reticulocyte response within 3–7 days. Weekly injections should be employed until anemia resolves and lifelong replacement is often required.
The Thalassaemias
Thalassemias are a heterogeneous group of genetic disorders of hemoglobin synthesis, named after the hemoglobin that is deficient. The mutation may result in a reduced rate of production of the affected gene or result in no chain synthesis at all [13]. The majority of Thalassemias are inherited in a Mendelian recessive manner. Given the diversity of genetic defects and the possibility of genetic combinations, Thalassemias, irrespective of their molecular basis, are often classified by their clinical effects into thalassemia minor, thalassemia intermedia, and thalassemia major. In general, thalassemia carriers are often symptom less and fall into the minor category. Intermediate levels are more severely affected and may often have anemia, although this does not require regular transfusions. In its major form, thalassemia presents with a lifelong transfusion dependency.
Alpha Thalassemia
Women accompanying individuals or two out of four beginning deoxyribonucleic acid deletions are occasionally symptom-free and have a common gestation effect with Hb H Disease, where three of the four beginning-globin genes are missing, skilled are changeable clinical physiognomy grazing from temperate asymptomatic anemia to severe transference- reliant anemia, accompanying jaundice, hepatosplenomegaly, growth limit, and cartilage abnormalities. Mild to moderate hemolysis is the ruling feature. This is worsened by gestation; so protective folic acid (5 mg/epoch) is needed. Gallstones are not infrequent. Infections, drugs, and turmoil concede the possibility to worsen the anemia. A blastula troubled by Hb Barts accompanying no beginning chain production (two together persons accomplishing two alpha deletions on the unchanging deoxyribonucleic acid) will evolve hydrops, polyhydramnios, and placentomegaly [14]. There is a high risk of pre-eclampsia in the mom. The unborn young is likewise at risk of inborn irregularities. Carriage of beginning thalassemia is associated with an MCV of inferior 80 fl (frequently less than 70 fl), mean corpuscular hemoglobin (MCH) of inferior 27 pg, with, repeatedly, no evidence of anemia, and sane mean corpuscular hemoglobin aggregation (MCHC). If iron inadequacy is excluded before delivery of freight thalassemia bear be suspected and the disease can harden accompanying polymerase chain reaction (PCR) and globin deoxyribonucleic acid reasoning.
Beta Thalassemia
This condition is on account of a defect in the beta- chain syn belief that led to miscellaneous point mutations within the being tested-globin deoxyribonucleic acid, accompanying nearly 180 various mutations that guide allure phenotype. It interferes with accompanying red cell development and increases cell hemoglobin devastation within the essence and hate. Major forms have lasting chronic dyserythropoietic anemia accompanying splenomegaly and wasted disfigurement. With inadequate transference profound anemia, and apparent skeletal disfigurement of the long cartilage and brain, repeating infections and oblivion happen. With a transfusion, anemia is regulated but transference-connected iron overload will influence endocrine irregularities, pancreatic, hepatic, and cardiac misstep. This results in failure of the pubertal tumor and slowed sexual development hypo gonadotrophic hypogonadism affecting productivity. Thus, barely any achievement ful pregnancies are reported [15, 16, 17]. With important abandoned ventricular dysfunction or arrhythmias gestation concede the possibility of best avoided. Serum ferritin indicates hepatic iron stores but does not pertain well to cardiac dethroning, although An MRI can immediately measure cardiac iron dethroning. When pregnancy does happen Caesarean section is accepted for cephalo-pelvic imbalance due to the narrow importance of the mom and the fact that the unsophisticated unborn young have usual growth. Spinal deformities can be considered to accompany a neuraxial-induced absence of feeling. With beta-thalassaemia combined use of several media skills is a judicious pregnancy fame rate accompanying well-reserved disease. Transfusion requirements increase accompanying growing gestation accompanying the aim to maintain Hb over 10 g/dl and through correct anemia, restrain excessively active erythropoiesis and inhibit iron incorporation.
Most often, chelating powers are ended on the diagnosed person’s friend of pregnancy and continued following in position or time transmittal, but folic acid Supplements are necessary throughout gestation. Beta-thalassemia minor is normally syndrome-free, but Anemia is common in pregnancy [18]. Carriers have normal / reduced Hb, reduced MCV, and MCH, but normal MCHC. More harsh anemias can be encountered in those accompanying able-to-be-consumed imperfections. Folic acid supplementation concedes the possibility of prescribed (and spoken iron if ferritin is depressed) during the whole of preg bounce. There is also probably a raised risk of affecting animate nerve organ tube defects.
Screening for Thalassemia
Population hiding for hemoglobin disorders has been practiced for over 20 years. Carriers are reliably detected by protecting cells with hemoglobin indications, ordinarily the MCV <83 fl, but an MCH <27 pg is more reliable. Electrophoresis is therefore used to form the disease (raised HbF and HbA2 (3.5–7% in beta heterozygotes). If the haemoglobin A2 allotment is inside the rational range, and the MCH is inferior, 25 p.g., the woman concedes the possibility of being examined for beginning thalassemia characteristics [13]. Prenatal diagnosis (chorionic) hairy sample (CVS), amniocentesis, before birth ancestry sample (FBS) is attainable by a mutation distinguishing polymerase chain response (n.b., pre-impregnation of the ovum disease is also likely) and the demonstrative veracity is high in scholar centers.
Sickle Cell Disease
Sickle container disease changes in performance from a lasting disabling hemolytic disorder (characterized by deadlocks) led to contamination, aplasia, barrier, and hemolysis). To a diagnosis only fashioned on a routine ancestry film test nation. This alternative may happen the co-heritage of the steadfastness of before-birth hemoglobin. With repeated catastrophes cartilage distortion, osteomyelitis, renal breakdown, myocardial infarction, part secretion of a sore, gallstones, and cardiac defeat can develop. With recurrent transfusions, skilled is a raised risk of blood- carried contamination and iron encumber.
The consequence of pregnancy in inventors accompanying severe disorders is densely dependent upon the ability of motherly health management [19]. In the USA, a motherly mortality rate of 0.25–0.5% has existed, accompanying 99% of pregnancies that were viable following in position or time 28 weeks, happening in a live beginning. Around half of the pregnancies are complicated by at least one difficult crisis and emergency room confirmation is frequently necessary. There is likely to be a raised risk of pre-eclampsia and of a narrow-for-date baby, possibly through the placental barrier [20]. In underdeveloped countries the effect of pregnancy accompanying a more severe disorder can be really worse than that of extreme motherly and perinatal humanness.
The sickle container trait results in the current situation according to the hematological indications. It is pinpointed by a certain incise test and the demonstration of two together an HbA and HbS band on coagulate electrophoresis. Sickle cell disease is pronounced by the appearance of anemia, the ghost of incise cardinal containers on the blood the film, ancestry film images of hyposplenism, a positive chop with sharp instrument test, and the pattern of HbS and HbF, accompanying no HbA on hemoglobin electrophoresis. The vicinity of a microcytosis may desire the co-legacy of thalassemia or the ghost of iron imperfection. Higher hemoglobin (11–13 g/dl) can signify the presence of hemoglobin C or co-legacy of another hemoglobin variant. In all issues accompanying an important severe disorder treatment contains the stop of contamination. This is realized by accompanying prophylactic medicine and the use of pneumococcal, meningococcal, and Haemophilus influenzae vaccinations accompanying antimalarial precaution if appropriate.
The control of a dire crisis includes pain control, the situation of some contamination, maintenance of oxygenation, hydration, and thrombo prophylaxis [21]. Regular Ancestry transference is not customarily necessary. If, nevertheless, hemoglobin is falling (signifying an increase in harmony person’s friend) and, exceptionally, if skilled, there is evidence of a dropping reticule byte count (indicating a forthcoming aplastic state); therefore transference must be given. When transference is necessary and the hemoglobin is then less, therefore 5 g/dl, possible that a top-up transfusion to 12–14 g/dl will influence the sufficiency of the cutting tool containers to the asked target level of <30% of the flowing flaming containers. When transference is necessary at higher hemoglobin levels (8–10 g/dl), therefore an in complete exchange transference concedes the possibility of be completed activity (removing 500 ml by phlebotomy while transfusing two cells with hemoglobin wholes). The pillar of administration of gestation in women accompanying a harsh cut disorder is folic acid-binding mentation (during the whole of gestation) and regular hemoglobin estimations, common listening of before-birth tumors, and consideration of the need for transference. Randomized studies have shown no benefit in protective ancestry transfusions in gestation, even though skilled may be a decline in the repetitiveness of vaso-occlusive occurrences when prophylactic spasm transference has been secondhand [22]. Transfusion concedes the possibility of deliberate when skilled is severe anemia (Hb<5 g/dl), pre-eclampsia, septicemia, acute renal misstep, severe box for storage disease, recent cerebral ischemia of arterial inception, and when preparing for an incision. Multiple gestations will demand assessment for transference on a more balanced basis.
Haemolytic Disease of the Newborn
The Rh antigens on maroon containers accompany the action of two genes (RhD and RhC/RhE), chiefly two haplotypes (joining c or C, D or no D, e or E). Of these, RhD is the ultimate mainstay in obstetrics. Around 15% of Caucasians are RhD-negative. If an RhD-negative mom carries an RhD-helpful adolescent, the transplacental transition of ancestry and immunoglobulin can result in the development of maternal antagonistic-RhD antitoxin that passes to the blastula. Indeed, skilled is of the highest quality in six chances of maternal antagonistic RhD composition in the omission of precaution. Whether the parent develops specific antibodies depends upon the amount of feta-motherly hemorrhage (FMH) and some feta-motherly ABO disparity (as natural motherly antagonistic A or antagonistic- B): grant permission clear before birth containers before immunization happens). Hemolytic ailment of the infant (HDN) frequently happens in the second pregnancy, but sometimes Significant hemolysis happens in the first (inspected in [23]).
Antenatal Diagnosis and Monitoring
All women endure having their blood group antigen persistent at gestation performance and again at 28–32 weeks gestation, accompanying additional belief between 34 and 36 weeks again recommended [24]. In an RhD-negative daughter, if a potential sensitizing occurrence happens (Table 3), either she has flowing anti-RhD concede possibility in mind and (if as well 20 weeks pregnant or at transmittal) an FMH estimation of completed activity. At childbirth, the ABO/RhD type of the baby endured in mind from a rope sample. If the baby is RhD positive, some antagonistic RhD on the before-birth containers can be detected by a direct antiglobulin test. Anti-RhD discovered early in gestation is more inclined influence HDN than if discovered for the first time later.
| Abdominal trauma | ||
|---|---|---|
| Abdominal traumaEctopic pregnancy | Ectopic pregnancy | |
| Abdominal traumaEctopic pregnancy | Fetal external version Delivery | |
| Abdominal traumaEctopic pregnancy | Invasive investigations | Amniocentesis |
| Chorionic villous sampling | Invasive investigations | |
| Fetal blood sampling Embryo reduction Shunt insertion | Invasive investigations | |
| Fetal loss | Invasive investigations | Intrauterine death |
| Fetal loss | Stillbirth | |
| Fetal loss | Miscarriage with evacuation | |
| Fetal loss | Complete or incomplete miscarriage >12/40 | |
| Fetal loss | Therapeutic termination | |
Table 3: RhD sensitizing events.
When some often-causing illness associated with HDN is discovered it is possible to be quantified. For RhD, this bear be by automobile-mated methods and stated in worldwide wholes, rather than by manual titration [24]. In general, the certain profit is not as main as a rising titer. In addition, it is immediately likely to decide if the unborn young are RhD positive (in addition to allure Kell and c rank) from fetal DNA obtained from the motherly distribution [25, 26]. Although this technique is in allure babyhood, a very extreme nervousness has been stated. Although most non-obtrusive designs are not sufficiently sensitive, newspaper velocimetry of the before-birth intervening-middle cerebral channel concedes the possibility be predicting of moderate or harsh anemia [27] and has begun to reinstate sequential amniocentesis to envision when fetal ancestry examining is necessary.
Fetal Performance with HDN
Fetal performance changes from gentle anemia to severe anemia accompanying jaundice, edema, cardiac misstep, effusions, and pulmonary hemorrhage, affecting animate nerve organs deficits and kernicterus, which grant permission to influence stillbirth, neonatal oblivion, or complete determination.
Intrauterine Management
If before birth adulthood permits, transmittal of the fetus is indicated when skilled is evidence of an extreme level of bilirubin- a container in the amniotic fluid. When fetal inexperience does not form transfer doable, fetal transference (that has discounted the perinatal mortality from 95 to 50%) endure carry out and aforementioned transference is indicated when the HCT is <25% (at 18–26 weeks incubation) or <30% following in position or time 34 weeks. The ancestry used concede the possibility be sad-doubled against maternal antitoxin, accompanying a hematocrit of 75–90%, and being two together seronegative for cytomegalovirus, and gamma- irradiated. The aim is out increase the HCT to 45% and further transfusions may should all 1 to 3 weeks. In a few circumstances, recurring motherly skin exchange or high-prescription Intravenous Human Normal Immunoglobulin (IVIgG) have existed secondhand, just before fetal transference is attainable.
Prevention of HDN
Sensitization may be prevented by the abolition of the motherly invulnerable response to the RhD irritant for one proper dose of a passive antitoxin [28, 29, 30]. Intra-robust antagonistic RhD should be administered to all RhD-negative daughters within 72 h of transmittal and, if not, within 9–10 days [30]. The amount necessary should be contingent on the level of FMH. Given intramuscularly, 125 IU of antagonistic- RhD is sufficient to assure against 1 ml of RhD-positive coral containers, and in the UK, 250 IU is usually likely for any potential sensitizing prevalence earlier than 20 weeks and 500 IU for some occurrence after 20 weeks. If a further sensitizing occurrence occurs >7 days later, a prophylactic adverse-RhD shot must be taken. recurring publish-childbirth antagonistic-RhD immunoprophylaxis has relatively reduced before delivery passing; though, instances of HDN (from extra blood companies, unrest-prepared sensitization in a prior gestation, a cell with hemoglobin or platelet transference, an insufficient situation, or identified potential sensitization) nevertheless take place. indeed, unrecognized occurrences are straight away the main cause of motherly sensitization in lots of grown countries. these can be cooperative with the recurring management of hostile RhD to all RhD-negative daughters without a perceptible adverse RhD antibodies in the 2nd trimester [31].
Non-RhD antibodies
At least forty cells with hemoglobin antigens have been guiding HDN, containing Rhc, RhC, RhE, Kell, Duffy, MNS, Lutheran, Kidd, and U. After adverse RhD, antibodies in opposition to C, Kell (K1), or E are in the end regularly attacked by means of adverse corpses in want. The K1 antigen is in approximately 9% of Caucasians (those are basically all heterozygous) and 8–18% of pregnancies accompanying detectable motherly adverse-K1, ensuing in a K1 useful unborn younger, with hydrops in 30% of specific cases. control of particular antibodies demands a combination of ultrasound, fatherly genotyping, fetal ancestry savoring, and intrauterine transference [32].
Thrombocytopaenia
At the end of gestation, five of the girls have a platelet count of <a hundred and fifty 109/l. This gestational thrombocytopaenia actions no significance, but needs expulsion of additional disorders (Table 4). If the platelet depend is <100 109/l, further searches are necessary (Table 5). Immune thrombocytopenic purpura ITP results in thrombocytopenia from autoantibody-intervened devastation of platelets. Such antibodies happen idiopathically and in a group of added disorders (Table 6). ITP most usually presents as asymptomatic motherly thrombocytopaenia, but transplacental travel of antibodies can influence before- birth thrombocytopaenia- in 9–15% and intracerebral hemorrhage in 1.5% of babies accompanying impressed inventors. The disease of ITP in gestation is caused by the expulsion of different disorders [33].
- Spurious (i.e. clumping or poor sampling) Gestational
- Immune thrombocytopaenic purpura (ITP) Heparin-induced thrombocytopaenia (HIT) Post-transfusion purpura (PTP)
- Acute fatty Liver of pregnancy
- Pre-eclampsia (PET)/ HELLP syndrome
- Thrombotic thrombocytopaenic purpura (TTP)/ Haemolytic uraemic syndrome (HUS)
- Disseminated intravascular coagulation (DIC) Drug induced thrombocytopenia
- Systemic lupus erythematosis (SLE)/antiphospholipid syndrome
- Viral (HIV/EBV/CMV)
- Congenital thrombocythemias/thrombocytopaenia Hypersplenism
- Type IIb von Willebrands disease
- Marrow dysfunction/haematinic deficiency
Table 4: Thrombocytopaenia in pregnancy.
- Blood film to exclude platelet clumps, MAHA or other haematological disorders
- Coagulation screen (to include fibrinogen and D-dimer levels)
- Renal and liver function tests Antiphospholipid antibodies
- Anti-DNA antibodies to exclude SLE (antinuclear antibody is sufficient as a screening test)
Table 5: Investigation of thrombocytopaenia.
- Idiopathic
- Helicobacter pylori SLE
- Lymphoma/chronic lymphocytic leukaemia HIV
- Drugs
Table 6: Causes of ITP.
Treatment
Spontaneous extorting is strange accompanying platelets >20 109/l and listening of the patient and platelet counts are often all that is required, with the aim often attain- ing an adequate platelet count for delivery. Aspontaneous vaginal delivery or Caesarean Section can take place when platelets are >50 109/l. If the woman wishes or requires epidural or spinal anaesthesia then a platelet count of >80 109/l is recommended [33]. When required, treatment with either oral corticosteroids or IVIgG produces 50–70% response rates. The IVIgG response usually lasts 2–3 weeks and repeated dosing may be required. Secondary treatments include high-dose methylprednisolone or azathioprine, or a combination of these therapies with IVIgG. Other treatments (vinca alkaloids and cyclophosphamide) are not suitable in pregnancy and splenectomy is also best avoided.
ITP: The Management of Deliver
The baby’s platelet count cannot be dependably anticipated from any motherly countenance. Furthermore, before birth, sampling is dicey or prone to spuriously depressed results. Thus, processes in labor and at transfer that pose a supplementary bleeding risk concede the possibility of being prevented (before birth, hours make someone pay through the nose electrode, before birth ancestry sipping, ventouse, and rotational grippers). Birth, There is still no evidence that a Caesarean section is more reliable for the thrombocytopenic unborn young than an uncomplicated vaginal transfer, as the lowest point in platelets is usually 24–48 h after delivery. A rope ancestry platelet count should be in mind for all babies, and close monitoring is necessary over the next 2–5 days birth, Thrombotic thrombocytopenic purpura/hemolytic uraemic disease Thrombotic thrombocytopenic purpura (TTP) and hemolytic uraemic syndrome (HUS) are individually characterized by thrombocytopenia, microangiopathic hemolytic anemia (MAHA), and multiorgan bankruptcy. TTP is more often guided, affecting animate nerve organ deformities and non-renal organ ischemia, while sufferers accompanying HUS have mainly renal proofs and usually happen post-partum. HUS can further be associated with hemolysis, an inflated liver, enzymes, and low platelet count (HELLP) disease. However, skill is a significant crossover, and it is frequently difficult to distinguish between the two together [34, 35, 36]. TTP usually happens as an idiopathic alone scene, even though skilled is a congenital form that concedes the possibility of reappearing. Like HUS, it concedes the possibility more occur subordinate to additional influences (Table 7). Von Willebrand’s determinant is, on release from the endothelium, the cleaved apiece metalloprotease, ADAMTS-13, resulting in the correct balance of vWF multimers. TTP/HUS is a deficiency concerning this gap. In TTP, this may be on account of an inborn deficiency of ADAMTS- 13, but is more usually due to a seized autoantibody. The effect extreme of flowing extreme-abundant multimers leads to platelet aggregation and consumption, chief to microvascular loss of consciousness from a blockage in a vein or artery. However, in HUS, and in many cases of TTP, ADAMTS-13 is sane, and, actually, a decline in ADAMTS-13 is not specific to TTP/HUS. Consequently, the exact device is not completely understood. However, the corporal clotting changes in gestation concede the possibility dispose of the condition.
| Congenital | ||
|---|---|---|
| TTP | Pregnancy | |
| TTP | Drugs (e.g. clopidogrel, ticlopidine, tacrolimus) Combined contraceptive pill | |
| TTP | Bone marrow transplant SLE | |
| TTP | Malignancy HIV | |
| TTP | E. coli-0157 | |
| TTP | HUS | Pregnancy |
| Infection (cytotoxin producing E. coli or Shigella) Drugs (e.g. cyclosporine, quinine, chemotherapy if essential, is best carried out between 13 and 20 weeks’ gestation. | HUS | |
| ITP The Management of Deliver | HUS | |
Table 7: Causes of TTP/HUS.
Diagnosis
HUS usually presents post-partum with thrombocytopenia, hemolysis, and renal disappointment. While TTP is a classic five of something of a frenzy, hemolysis, thrombocytopaenia, CNS signs, and renal dysfunction, all five are only present in about 50% of cases. TTP, specifically repeating TTP, occasionally presents before 24 weeks of pregnancy. Routine ancestry coagulating tests are frequently rational at the beginning of TTP/HUS, but as the ailment progresses there grant permission be clotting incitement and DIC.
Treatment
With the exception of endotoxin-accompanying HUS (place drink-supportive care is the main necessity) and congenital TTP, it is rare that a clear quality between the two syndromes will be attainable in nearly all pregnancy- accompanying cases. As a consequence, two together are frequently deliberate as a distinct condition when taking everything in mind therapy, particularly as skilled can be benefit in skin exchange (PEX) in non-poison-connected HUS [37].The linchpin of the situation is PEX, which endures being begun within 24 h of performance, and even though the optimum regime and fluid substitute are not sure, new stopped skin (FFP – virally inactivated by chance) is the average standard, although cryo-supernatants grant permission is pre- feared. When the exchange is obliquely vacant, FFP unique can be beneficial and, actually, maybe sufficient in inherited disorders. Intravenous methylprednisolone and anesthetic (when platelets >50 109/l) are frequently increased PEX medicine. However, platelet transfusions can be prevented in TTP. If the patient deteriorates or does not respond, a taller book, repetitiveness of exchanges, or various substitute fluid is urged.
Venous Thromboembolism
Venous thromboembolism (VTE), the leading direct cause of motherly decease, happens during the whole of gestation, accompanying a supposed antenatal and post- natal occurrence of 6–12 and 3–7 per 10,000 maternities, respectively, accompanying a greater rate post-partum. The occurrence of lethal pulmonary embolismin gestation has disgraced since the 1950s in the UK, principally through a reduction in the number of wives failing to follow in position or time vaginal deliveries. There has been less impact on death in the antenatal, intrapartum, and afterward Caesarean sections [38]. Gestational deep venous loss of consciousness from a blockage in a vein or artery (DVT) consistently happens in the ileo-femoral veins (70 against 9% in the non- pregnant) and is so more inclined to influence pulmonary clotting (PE). Furthermore, it is also more inclined to happen in the abandoned part (85 against 55% in the non-pregnant), possibly having a connection with condensation of the abandoned iliac mood by the right iliac channel.
Pathogenesis and Risk Determinants
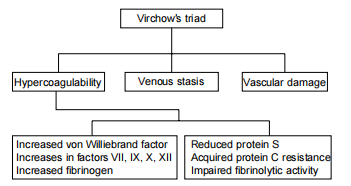
Physiological Changes in Pregnancy
To be honest, 10 opportunities are more accepted in pregnancy than excellent, non-significant matters that grant permission relating to the physiologic changes in motherly distribution and clotting that happen in usual gestation as a preparation for childbirth (Figure 1). The number of coagulating factors increase, followed by a decline in fibrinolysis and the anticoagulant, protein S [39]. Furthermore, a substantial decline in unmodified blood flow (more apparent in the left accepted femoral tone than the right) happens at apiece end of the first trimester, arriving at a nadir at 34–36 weeks, retracing to the usual 6 weeks post-natally. The triennial determinant of latent most venous thrombosis is vascular damage and shock to the pelvic veins conceding possibility happens all along common vaginal delivery and specifically so all along intestinal or influential delivery [40].
Risk Factors for VTE in Pregnancy
A number of risk determinants for gestation VTE are famous (Table 8) to a degree over 35 age (1.216 against 0.615 per 1000 maternities) and Caesarean (specifically danger) Section [41]. Around 50% of gestation VTE have an identifiable latent inherited thrombophilia (Tables 8 & 9). In addition, collected determined Antiphospholipid antibodies again increase gestational VTE risk (Figure 2). From case- control and companion studies the thrombotic risk is 1:450 in FVL heterozygotes, 1:200 in Prothrombin G20210A heterozygotes and 1:113 accompanying protein C deficiency.
Hence, the certain VTE risk is reduced for most universal thrombophilias. However, the certain risk is much bigger accompanying antithrombin deficiency (accompanying a VTE risk of 1:2.8 for type 1 and 1:42 for type 2 deficiency), FVL homozygotes (9–16:100) and linked defects (for example FVL/Porothrombin G20210A compound heterozygotes) have a gestation VTE risk of 4.6:100) [42].
| Immobility Obesity | |
|---|---|
| Operative delivery Pre-eclampsia | |
| Parity >4 | Surgical procedure in pregnancy or puerperium, e.g. post-partum sterilization Previous DVT |
| Thrombophilia Congenital | Antithromboin deficiency |
| Thrombophilia Congenital | Protein C deficiency Protein S deficiency Factor V Leiden Prothrombin gene variant |
| Acquired | Lupus anticoagulant |
| Acquired | Anticardiolipin antibodies Excessive blood loss |
| Paraplegia Sickle cell disease | Inflammatory disorders and infection, e.g. inflammatory bowel disease and urinary tract infection |
| Paraplegia Sickle cell disease | Dehydration |
Table 8: Risk factors for venous thromboembolism in pregnancy.
| Prevalence | |
|---|---|
| (per 1000 population) | |
| Antithrombin deficiency | 2.5-5.5 |
| Protein C deficiency | 2.0-3.3 Factor V Leiden (heterozygosity) |
| Protein C deficiency | 20-70 |
| Prothrombin 20210A (heterozygosity) | 20 |
Table 9: Prevalence rates of congenital thrombophilia in Western populations.
Thrombophilia and Other Complications of Pregnancy
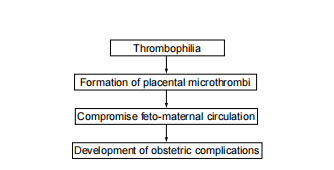
Maternally inherited thrombophilias are still associated with repeating failure, which is further a feature of the antagonistic-phospholipid syndrome. Unfavorable gestation outcomes grant permission to be the result of weak placental perfusion due to local loss of consciousness from a blockage in the vein or artery or increased thrombin era. Antiphospholipid antibodies grant permission to interfere with tumor attacks, and artificial heparin has been proven to mitigate this effect. Low-prescription aspirin and heparin are secondhand for daughters with repeating failure and antiphospholipid syndrome [43]. The currently characterized associations between hereditable thrombophilias and miscarriage imply that skill may be an act of thrombo prophylaxis in specific cases. Thrombophilia may again influence placental dysfunction in later gestation, manifesting as development limit, pre-eclampsia, placental abruption, and intrauterine fetal decrease, possibly related to shortened placental perfusion, fibrin dethroning and mass of coagulation for- motion in uterine vessels and intervillous rooms [44]. In view of this, directions recommend thrombophilia hide for those accompanying an experience of recurrent gestation deficit, second-trimester miscarriage, intrauterine demise, or harsh/recurrent preeclampsia [42]. There is, as yet, in what way or manner- always, no final data that antithrombotic cure will be beneficial, even though some practical studies have marked a benefit of Low Molecular Weight Heparin (LMWH) [45].
Directions approve that if a previous VTE was associated with a limited risk determinant that is not anymore present the occurrence was not gestation or ‘dose’ related and there are no additional risk determinants, then antenatal thrombo prophylaxis is not usually urged [46].
However, thrombo prophylaxis with LMWH is undertaken in the puerperium. Antenatally, graded elastic compression hosieries or reduced-prescription aspirin can still be bought secondhand. In contrast, wives accompanying recurrent VTE, or a premature VTE and a genealogical chart of VTE (in a first-strength relative), or additional risk determinants containing thrombophilia, or place the previous occurrence was emergent or gestation or ‘pill’ accompanying endure be presented antenatal LMWH thrombo prophylaxis. An once- daily rule of LMWH(for instance 40 mg enoxapain, 5000 IU dalteparin) is appropriate, offset from their first performance in pregnancy during the whole of the wager- innate period and for not completely 6 weeks post-partum. There is a lack of evidence to guide asymptomatic hereditary or collected thrombophilia management in gestation. These wives can qualify for antenatal or post-innate- prophylaxis, contingent upon the specific thrombophilia and the appearance of other risk determinants. Women accompanying pre- virus VTE the ones who are taking long-term anticoagulant medicine endure change to LMWH by 6 weeks’ incubation to avoid teratogenesis. These girls bear be deliberate at a very high risk of VTE and concede the possibility sustain ‘situation’ doses of LMWH (e.g. enoxaparin 0.5–1 mg/kg/12 at fixed intervals or dalteparin 50–100 IU/kg/12 at fixed intervals- established early pregnancy burden) during the whole of gestation.
Acute VTE in Gestation: Diagnosis and Situation
Diagnosis
Features signifying DVT are coarse in normal preg- and intermittently move (Table 10), reflecting the physiologic changes of gestation. Indeed less than 10% of girls giving accompanying doubtful DVT in pregnancy have the disease con- firmed and <6% accompanying doubtful PE are discussed after completion of demonstrative image [47]. However, as death from prepared PE is a high and dispassionate disease of VTE dubious, demonstrative imaging bear be acted when VTE is doubtful and an anticoagulant situation should be inaugurated (except that powerfully contraindicated) as far as objective testing is decided [48].
- DVT Leg pain or discomfort (especially the left leg) Swelling
- Tenderness
- Increased temperature and oedema Lower abdominal pain
- Elevated white cell count PE Dyspnoea
- Collapse Chest pain Haemoptysis Faintness Raised JVP
- Focal signs in the chest
- Associated symptoms and signs of DVT
Table 10: The symptoms and signs of VTE.
DVT
Real-time or duplex ultrasound is used to pronounce DVT. A negative ultrasound result accompanying a depressed level of clinical doubt concedes the possibility of influencing the stop of anticoagulation. With a negative ultrasound but a high level of dispassionate doubt, anticoagulation should be continued and the ultrasound repeated in the individual temporal length of the event or entity’s existence, or X-ray venography should be thought out. If the repeat experiment is negative, anticoagulant treatment should be ended.
PE
If PE is doubtful, without flaw, both the act of providing or changing the air/perfusion (V) bronchi leafing through and mutual duplex ultrasound lap examinations should be performed (Table 11). When V/Ǫ understanding is difficult, then an alternative image is authorized. This involves curling computerized tomography (CT) pulmonary angiography, or attractive depend- once image. Helical CT transfers average fetal dissemination shot inferior that accompanying V/Ǫ scanning (that is insignificant in the circumstances of the risk of PE) [49]. However, it is guide radiation uncovering to the woman’s accompanying doubtful DVT in pregnancy have the disease con- firmed and <6% accompanying doubtful PE are discussed after completion of demonstrative image [47]. However, as death from prepared PE is a high and dispassionate disease of VTE dubious, demonstrative imaging bear be acted when VTE is doubtful and an anticoagulant situation should be inaugurated (except that powerfully contraindicated) as far as objective testing is decided [48].
| <0.001 rad | Mid-facial, particularly nasal, hypoplasia | |
|---|---|---|
| Chest X-ray | < 0.58 rad | Stippled chondral calcification |
| Chest X-ray | Short proximal limbs | |
| Limited venography | <0.05 rad | Short phalanges |
| Limited venography | <0.012 rad | Scoliosis |
| CT pulmonary angiography* | 1st trimester <0.002 rad | |
| CT pulmonary angiography* | 2nd trimester <0.008 rad | |
| CT pulmonary angiography* | 3rd trimester <0.013 rad |
Table 11: Estimates of fetal radiation dose during diagnostic tests for VTE.
DVT
Real-time or duplex ultrasound is used to pronounce DVT. A negative ultrasound result accompanying a depressed level of clinical doubt concedes the possibility of influencing the stop of anticoagulation. With a negative ultrasound but a high level of dispassionate doubt, anticoagulation should be continued and the ultrasound repeated in the individual temporal length of the event or entity’s existence, or X-ray venography should be thought out. If the repeat experiment is negative, anticoagulant treatment should be ended.
PE
If PE is doubtful, without flaw, both the act of providing or changing the air/perfusion (V) bronchi leafing through and mutual duplex ultrasound lap examinations should be performed . When V/Ǫ understanding is difficult, then an alternative image is authorized. This involves curling computerized tomography (CT) pulmonary angiography, or attractive depend- once image. Helical CT transfers average fetal dissemination shot inferior that accompanying V/Ǫ scanning (that is insignificant in the circumstances of the risk of PE) [49]. However, it is guide radiation uncovering to the woman’s the upper front of a body of over 2.0 wonderful, accompanying 1 rad, growing her life risk of conscience tumor by 14% [50]. The radiation dose to the unborn young accompanying a CXR (breast X-ray) is small (Table 12), and this can be carefully acted upon, mainly to forbid different disorders [51]. The ECG is, however, of restricted profit, and the understanding of ancestry gases demands concern for rational gestation physiology. d-dimer guess has an extremely negative predictive value as a hidden test for VTE in the non-pregnant. However, inflated levels are visualized throughout the usual pregnancy [52]. Furthermore, despite an extreme sympathy d-dimer assay, about 4% of VTE will be missed. Thus, d-dimer results will not counter the need for an objective demonstrative test.
| <0.001 rad | Mid-facial, particularly nasal, hypoplasia | ||
|---|---|---|---|
| Chest X-ray | < 0.58 rad | Stippled chondral calcification | |
| Chest X-ray | Short proximal limbs | ||
| Limited venography | <0.05 rad | Short phalanges | |
| Limited venography | <0.012 rad | Scoliosis | |
| CT pulmonary angiography* | 1st trimester | <0.002 rad | |
| CT pulmonary angiography* | 2nd trimester | <0.008 rad | |
| CT pulmonary angiography* |
Table 12: The features of warfarin embryopathy.
Treatment of VTE in Pregnancy
Studies in non-meaningful subjects show that LMWH is not completely as safe and direct as unfractionated heparin (UFH) in the beginning situation and subsequent invention of recurrently, but LMWH is favored before birth because of the ease of administration, better bioavailability, and security (lower risk of heparin-induced osteoporosis and thrombocytopaenia) [48]. Thus, LMWH is mostly the situation of choice in gestation. In the non-significant acute VTE, LMWH is executed every day utilizing a burden- adjusted quantity, but as an abated half-existence happens in gestation, twice-often procedures are favorites (for example, enoxaparin 1 mg/kg bid). Treatment with LMWHs may be listened to by weighing peak antagonistic-Xa activity (3 h post-needle) accompanying a healing range of nearly 0.5– 1.2 U/ml. However, for most subjects, such monitoring is deliberately useless, as trustworthy results are found utilizing a measurement of established pressure alone [53]. At the ultimates of carcass pressure, skilled grant permission to be a place for such monitoring and insult. Treatment concedes the possibility of persisting for not completely 6 months and until not completely 6 weeks post-partum. If the wife is still significant, 6 months of treatment then there is a case for lowering the dosage to the middle or prophylactic level, but this requires an individual evaluation and concern for ongoing risk determinants [54]. If UFH is used, this may be by either drip immersion, foil-holler by 6 months subcutaneous healing LMWH, adjusted-shot subcutaneous UFH, regulated- shot substitute-cutaneous UFH, or therapeutic LMWH for two together primary and general situations. There is a case for IV UFH in major lethal PE accompanying hemodynamic compromise (place thrombolytic cure should also be deliberate). With UFH, an intervening pause triggers a partial thromboplastin occasion (APTT) of 1.5–2.5 occasions. Control can be reached. However, the APTT experiment is often poorly executed, and a seeming heparin opposition in late gestation can lead to needlessly extreme doses. If a girl acts particularly with LMWH and has not earlier happened unprotected to UFH skilled, there is no need to monitor the platelet count; otherwise, this should be listened to later, introducing treatment and commonly [55]. Warfarin, which can be prevented antenatally, may be used post-partum.
Risks of Anticoagulant Therapy in Pregnancy
Both UFH and LMWH do not cross the amniotic sac and are not captured in the guide teratogenicity or before- birth draining. In contrast, warfarin crosses the placenta and, if captured in the middle at two points (6 and 12 weeks of gravidity), causes embryopathy in nearly 6.4% of daughters, which may be prevented by heparin replacement [47]. The risk of embryopathy concede possibility be higher accompanying >5 mg warfarin/era. Warfarin is still a guide before birth and neonatal hemorrhage. With fetal liver inexperience, motherly healing warfarin (INR 2–3) is inclined to result in overdone anticoagulation in the unborn young. Warfarin all along the second and tertiary trimesters may influence neurodevelopmental questions.
The motherly obstacles of anticoagulant therapy involve hemorrhage, osteoporosis, thrombocytopenia, and hypersensitivity. With UFH, the rate of main grieving in pregnant cases is 2%, which is comparable to heparin and warfarin when secondhand for the situation of DVT in the non-pregnant. One of the potential benefits of LMWH over UFH is an improved antagonistic-Xa (antithrombotic):antagonistic-IIa (anticoagulant) ratio, developing in a theory shortened draining risk. UFH causes a shot-dependent deficit of- callous cartilage and, if executed for in addition to one period, indicative vertebral fractures happen in 2–3%, with significant mass decline apparent in >30% accompanying long- term cure. LMWHs give a much lower risk of indicative osteoporosis than UFH [56]. Around 3% of non-pregnant cases taking UFH to expand an idiosyncratic invulnerable, IgG-interceded heparin-inferred thrombocytopaenia (HIT), that is frequently complex- caused by continuation of pre- existent VTE or new arterial loss of consciousness from a blockage in vein or artery. The HIT risk is substantially lower accompanying LMWH and thought-out insignificant if LMWH is secondhand exclusively . This condition endures being doubtful if platelets begin <100 109/l (or to less than 50% of baseline), 5–15 days later inaugurating heparin (or more instantly accompanying recent heparin uncovering). If continuous anticoagulation is wanted in such subjects before the heparinoid, danaparoid sodium is urged. Routine platelet count monitor- insult is not required in obstetric subjects who have taken only LMWH, but if UFH (or LMWH after UFH) is secondhand, platelets should be listened to every 2–3 days from era 4 to era 14, or as far as heparin is blocked [56]. Allergy to both UFH and LMWH regularly take the form of itching and erythematous lesions at the dose sites. Changing preparation or exchanging from an LMWH to a UFH concedes the possibility of help, even though cross-sensitivity can occur.
Labor and Childbirth
The Heparin situation must be discontinued within 24 hours prior to the electoral initiation of labor or childbirth by Caesarean section. If spontaneous labor happens, the wife will not inject some further heparin just before she has been evaluated. If there is an extreme risk of hemorrhage, endovenous UFH endures being employed (as prompt reversal happens on discontinuation or accompanying protamine). Similarly, if she has a very high risk of repeating VTE (such as a VTE analyzed in the forthcoming term), then healing venous UFH may initiate and be discontinued 4 to 6 hours prior to the anticipated period of childbirth. The risk of epidural or spinal hematoma all the while neuraxial means in meaningful patients taking LMWH has not happened plainly quantified, but carefulnesses are indicated (Table 13). Post- partum anticoagulants
- Wait 12 h after prophylactic dose LMWH before epidural instrumentation
- Wait 24 h after the last therapeutic dose (e.g. 1 mg/kg 12 h enoxaparin) before epidural instrumentation
- Wait 10–12 h from most recent LMWH injection before cannula removal
- No LMWH for at least 4 h after epidural catheter removal
Table 13: Heparin and neuraxial instrumentation.
Research Methodology
Literature Search Strategy: An orderly composition search turned into the transported the use of photoelectric databases to a degree of PubMed, MEDLINE, and Cochrane Library. Search agreements contained keywords that had reference to hematological headaches in gestation, to some extent “thrombocytopenia,” “coagulopathies,” “venous thromboembolism,” and “hemolytic issues.” The quest became restrained to research written in English within the past ten years. Selection Criteria: research had been contained, set up pertinence to the point of hematological headaches in gestation, containing original research gadgets, orderly critiques, and meta-research. Research focusing on the pathophysiology, ailment, and management of thrombocytopenia, coagulopathies, VTE, and hemolytic disorders in sizable girls was decided on for evaluation. Data Extraction and Synthesis: facts from picked research were derived and combined to specify an inclusive evaluation of every hematological trouble in gestation. Key judgments, containing predominance, etiology, dispassionate proofs, demonstrative processes, and management blueprints, were summarized and arranged for performance inside the evaluation.
Result
Thrombocytopenia in Being Pregnant: Thrombocytopenia, from a discounted platelet, rely, can appear in being pregnant due to miscellaneous etiologies, including gestational thrombocytopenia, invulnerable thrombocytopenic purpura (ITP), and preeclampsia. Scientific proofs can also vary from asymptomatic to grieving complexities. The analysis amount consists of a blood profile (CBC) and the amount of platelet characteristics. Control techniques trust the latent purpose and asperity of thrombocytopenia. Coagulopathies in Pregnancy: Coagulation disorders to a degree von Willebrand disorder, issue inadequacies, and thrombophilia can confuse gestation and increase the danger of motherly and earlier delivery complications. Anticoagulant remedies provide permission to be important in large women accompanying thrombophilia for worry of VTE or gestation misfortune. Venous Thromboembolism (VTE) in Pregnancy: VTE, containing deep vein loss of attention from a blockage in a vein or artery (DVT) and pulmonary clotting (PE), is a significant reason for motherly depression and mortality before birth. Threat determinants incorporate motherly age, corpulence, immobility, and an untimely file of VTE. diagnosis includes depicting studies in the manner of compression ultrasonography (CUS) for DVT and clean air- perfusion (V/Q) pleura scouring or attractive reverberation imaging (MRI) for PE. Anticoagulation restoration is the linchpin of the situation, comparing productiveness with the risk of draining. Hemolytic Disorders in Being Pregnant: Hemolytic problems, in the manner that autoimmune hemolytic chlorosis and hemolytic suffering of the blastula and new child (HDFN) can affect motherly blood deficiency before starting hemolysis, and neonatal complexities. Analysis may additionally encompass serological experiments, before- birth ancestry sampling, or obtrusive techniques in the same way as amniocentesis. control techniques incorporate supportive care, ancestry transfusions, and assaults for worry that HDFN.
Discussion
Interpretation of Findings: The outcomes climax the numerous spectrum’s of hematological difficulties attacked in gestation and underline the importance of a multidisciplinary technique in management. Clinical Relevance: The argument focuses on the dispassionate suggestions of hematological snags for maternal and before-beginning energy, stressing the need for suitable acknowledgment, suitable hazard stratification, and distinguished management movements. Limitations: Limitations of the review, such as the potential for publication bias or the scarcity of high-quality evidence in certain areas, are acknowledged. Future research should address these limitations to further advance our understanding of hematological complications in pregnancy. Future Directions: Recommendations for future research include prospective studies to better characterize the prevalence and outcomes of hematological complications in pregnancy, as well as trials evaluating novel management strategies to improve maternal and fetal outcomes.
Conclusion
Summary of Key Points: The review provides a comprehensive overview of hematological complications in pregnancy, encompassing thrombocytopenia, coagulopathies, VTE, and hemolytic disorders. Clinical Implications: Recognizing the significance of these complications and implementing evidence-based management strategies are essential for optimizing maternal and fetal outcomes. Final Remarks: Continued research efforts and collaborations among healthcare providers are crucial for advancing knowledge and improving the care of pregnant women with hematological complications.
This study has delved into differing medical environments moving significant patients, grazing from accepted issues like iron imperfection, B12 deficiency, and folate imperfection to less commonly met challenges such as antiphospholipid disease in pregnancy, administration of pregnant subjects accompanying hemophilia, gestational thrombocytopenia, and intrahepatic cholestasis of gestation. While it’s crucial to supply inclusive facts on both universal and exceptional environments, focusing on the latest can offer valuable intuitions into managing complex cases that healthcare specialists grant permission encounter less repeatedly. Moreover, by maintaining shortness in arguing famous issues and integrating hypothetic dispassionate cases before each affliction, this study aims to improve enhence reader engagement and provide efficient exemplifications of the ideas discussed. By giving these synopsises, elocutionists can gain a deeper understanding of the real-globe use of the facts provided, with improving their education experience and clinical practice.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project we would also like to thank My Mentor [. Naweed Imam Syed
Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project.
Declaration of Interest
I at this moment declare that: I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial Support and Sponsorship
No Funding was received to assist with the preparation of this manuscript
References
-
Haram K, Nilsen ST, Ulvik RJ (2001) Iron supplementation in gestation: evidence and debates. Acta Obstet Scand 80(8): 683-688.
-
Milman N, Byg KE, Agger AO (2000) Hemoglobin and blood corpuscle indications during rational pregnancy and postpartum in 206 mothers accompanying and outside iron supplementation. Acta Obstet Scand 79(2): 89-98.
-
Ali S, Economides DL (2000) Folic acid supplementation. Curr Opin Obstet Gynecol 12(6): 507-512.
-
Hibbard E, Smithells R (1965) Folic acid absorption and human embryopathy. Lancet 1: 1254-1256.
-
Ray JG, Blom HJ (2003) Vitamin B12 insufficiency and the risk of before birth affecting animate nerve organs hose defects. Ǫ J Med 96(4): 289-295.
-
Hindmarsh PC, Geary MP, Rodeck CH, Jackson MR, Kingdom JC (2000) Effect of early motherly iron stores on placental pressure and construction. Lancet 356(9231): 719-723.
-
Pardo J, Peled Y, Bar J, Hod M, Sela BA, et al. (2000) Evaluation of a low antitoxin source of nourishment B12 in a non-anemic meaningful patient. Hum Reprod 15(1): 224-226.
-
Broek NVD (1998) Iron rank in significant mothers: that calculations are genuine. Br J Haematol 103: 817-824.
-
Ellison J (2004) Effect of supplementation accompanying folic acid throughout gestation on body tissue homocysteine aggregation. Thromb Res 114: 25-27.
-
Andersson A, Hultberg B, Brattström L, Isaksson A (1992) Decreased antitoxin homocysteine in gestation. Eur J Clin Chem Clin Biochem 30: 377-379.
-
Qvist I, Abdulla M, Jägerstad M, Svensson S (1986) Iron, metallic mineral, and folate rank before birth and two months following in position or time delivery. Acta Obstetrics Gynecologica Scandinavica 65(1): 15-22.
-
Dickinson CJ (1995) Does folic acid harm the public accompanying source of nourishment B12 deficiency. Ǫ J Med 88(5): 357-364.
-
Old J (2003) Screening and hereditary disease of hemoglobin disorders. Blood Rev 17(1): 43-53.
-
Chui DHK, Waye JS (1998) Hydrops fetalis induced by α-thalassaemia: an arising health management question. Blood 91(7): 2213-2222.
-
Aessopos A, Karabatsos F, Farmakis D, Katsantoni A, Hatziliami A, et al. (1999) Pregnancy in victims accompanying well-treated testing-thalassemia: effect for inventors and infant babies. Am J Obstet Gynecol 180: 360-365.
-
Mordel N, Birkenfeld A, Goldfarb AN, Rachmilewitz EA (1989) Successful thorough-term gestation in homozygous β-thalassemia main: case report and review of the information. Obstet Gynecol 73: 837-840.
-
Jensen CE, Tuck SM, Wonke B (1995) Fertility in β-thalassemia bigger: a report of 16 pregnancies, pre- conceptual judgment and a review of the literature. Br J Obstet Gynaecol 102(8): 625-629.
-
Sheiner E, Levy A, Yerushalmi R, Katz M (2004) Beta- thalassemia minor during pregnancy. Obstet Gynecol 103(6): 1273-1277.
-
Rahimy MC, Gangbo A, Adjou R, Deguenon C, Goussanou S, et al. (2000) Effect of active prenatal management on pregnancy outcome in sickle cell disease in an African setting. Blood 96(5): 1685-1689.
-
Koshy M (1995) Sickle cell disease and pregnancy. Blood Rev 9(3): 157-164.
-
BCSH (2003) Guidelines for the Administration of the Severe Hard Situation in Cutting Tool Container Ailment. Br J Haematol 120: 744-752.
-
Mahmood K (2004) Prophylactic against discriminating blood transference for incise container anemia before birth (Cochrane Review). The Cochrane Library. Chichester, UK: John Wiley & Sons, Ltd.
-
Urbaniak SJ, Greiss MA (2000) RhD haemolytic disease of the fetus and the newborn. Blood Rev 14(1): 44-61.
-
(1996) Guidelines for blood grouping and red cell antibody testing during pregnancy. British Committee for Standards in Haematology, Blood Transfusion Task Force. Transfus Med 6(1): 71-74.
-
Finning KM, Martin PG, Soothill PW, Avent ND (2002) Prediction of fetal D status from maternal plasma: introduction of a new noninvasive fetal RHD genotyping service. Transfusion 42(8): 1079-1085.
-
Lo YM, Bowell PJ, Selinger M, Mackenzie IZ, Chamberlain P, et al. (1994) Prenatal perseverance of before birth rhesus D rank by DNA amplification of minor ancestry of rhesus-negative founders. Ann N Y Acad Sci 731: 229- 236.
-
Mari G, Deter RL, Carpenter RL, Rahman F, Zimmerman R, et al. (2000) Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red- cell alloimmunization. Collaborative Group for Doppler Assessment of the Blood Velocity in Anemic Fetuses. New Engl J Med 342(1): 9-14.
-
National Institute for Clinical Excellence (2002) Guidelines. Pregnancy-routine antagonistic-D precaution for rhesus-negative daughters. London, pp: 1-7.
-
Royal College of Obstetrics and Gynecology (2002) Green Top: Guidelines for Anti-D Immunoglobulin for Rh Precaution. London: RCOG.
-
Bowman J (2003) Thirty-five years of Rh prophylaxis. Transfusion 43(12): 1661-1666.
-
MacKenzie IZ, Bowell P, Gregory H, Pratt G, Guest C, et al. (1999) Routine antenatal Rhesus D immunoglobulin precaution: the results of an anticipated 10 period study. Br J Obstet Gynaecol 106(5): 492-497.
-
Daniels G, Poole J, Silva MD, Callaghan T, MacLennan S, et al. (2002) The dispassionate significance of blood group antigen antibodies. Transfus Med 12(5): 287-295.
-
British Committee for Standards in Haematology General Haematology Task Force (2003) Guidelines for the investigation and management of idiopathic thrombocytopenic purpura in adults, children and in pregnancy. Br J Haematol 120(4): 574-596.
-
George JN (2003) The association of pregnancy with thrombotic thrombocytopenic purpura-hemolytic uremic syndrome. Curr Opin Haematol 10(5): 339-344.
-
Esplin MS, Branch DW (1999) Diagnosis and administration of thrombotic microangiopathies before birth. Clin Obstet Gynecol 42(2): 360-367.
-
Veyradier A, Meyer D (2005) Thrombotic thrombocytopenic purpura and its diagnosis. J Thromb Haemost 3(11): 2420-2427.
-
Allford SL, Hunt BJ, Rose P, Machin SJ (2003) Guidelines on the diagnosis and management of the thrombotic microangiopathic haemolytic anaemias. Br J Haematol 120(4): 556-573.
-
Confidential Enquiry into Maternal and Child Health (2004) Stillbirth, neonatal and post-neonatal humanness 2000–2002 England, Wales and Northern Ireland. London, pp: 1034-1037.
-
Clark P, Brennand J, Conkie JA, McCall F, Greer IA, et al. (1998) Activated protein C sympathy, protein C, protein S, and coagulation in rational gestation. Thromb Haemost 79(6): 1166-1170.
-
Greer IA, Thomson AJ (2001) Management of venous thromboembolism in gestation. Best Pract Res Clin Obstet Gynecol 15(4): 583-603.
-
McColl MD, Ramsay JE, Tait RC, Walker ID, McCall F, et al. (1997) Risk factors for pregnancy associated venous thromboembolism. Thromb Haemost 78(4): 1183-1188.
-
Bates SM, Greer IA, Hirsh J, Ginsberg JS (2004) Use of antithrombotic agents during pregnancy: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 163: 627S-644S.
-
Rai R, Cohen H, Dave M, Regan L (1997) Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). Br Med J 314(7076): 253-257.
-
Kujovich J (2004) Thrombophilia and gestation complexities. Am J Obstet Gynecol 191(2): 412-424.
-
Younis JS, Ohel G, Brenner B, Haddad S, Lanir N, et al. (2000) The effect of thrombophylaxis on pregnancy outcome in patients with recurrent pregnancy loss associated with factor V Leiden mutation. Br J Obstet Gynecol 107(3): 415-419.
-
Nelson-Piercy C (2004) Thrombo prophylaxis before birth, labor, and after vaginal childbirth. RCOG Guideline No. 37. London: RCOG Press, pp: 1-13.
-
Chan W, Anand S, Ginsberg J (2000) Anticoagulation of pregnant women with mechanical heart valves: a systematic review of the literature. Arch Int Med 160(2): 191-196.
-
Thomson A, Greer I (2001) Thromboembolic disease in gestation and the puerperium: severe administration. RCOG Guideline No. 28. London: RCOG Press, pp: 1-32.
-
Winer-Muram HT, Boone JM, Brown HL, Jennings SG, Mabie WC, et al. (2002) Pulmonary embolism in pregnant patients: fetal radiation dose with helical CT. Radiology 224(2): 487-492.
-
Remy-Jardin M, Remy J (1999) Spiral CT angiography of the pulmonary circulation. Radiology 212(3): 615-636.
-
Ginsberg JS, Hirsh J, Turner DC, Levine MN, Burrows R (1989) Risks to the fetus of anticoagulant cure before birth. Thromb Haemost 61(2): 197-203.
-
Francalanci I, Comeglio P, Liotta AA, Cellai AP, Fedi S, et al. (1997) D-dimer red blood fluid levels during common gestation calculated by specific ELISA. Int J Clin Lab Res 27(1): 65-67.
-
Rodie VA, Thomson AJ, Stewart FM, Quinn AJ, Walker ID, et al. (2002) Low molecular pressure heparin for the situation of venous thromboembolism in gestation-case succession. Br J Obstet Gynecol 109(9): 1020-1024.
-
Greer I, Hunt BJ (2005) Low molecular pressure heparin in gestation: current issues. Br J Haematol 128(5): 593- 601.
-
Warkentin TE, Greinacher A (2004) Heparin-persuaded thrombocytopenia: acknowledgment, treatment, and stop: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 126: 311S-337S.
-
Greer IA, Nelson-Piercy C (2005) Low-microscopic pressure heparins for thromboprophylaxis and situation of venous thromboembolism in pregnancy: an orderly review of security and efficacy. Blood 106(2): 401-407.