Geospatial Analysis of Diabetes Patients’ Distribution within an Urbanized Environment of Ile-Ife, Southwestern, Nigeria
Diabetes Mellitus is a lingering metabolic disease considered as a germane public health issue in Nigeria. The study identified socio-demographic features of diabetes prevalence and their spatial distribution patterns aimed at devising future prevention against diabetic risks in the study area. This study considered GIS application in the spatial assessment of diabetes prevalence in Ile-Ife, Nigeria. One hundred and eighty-three copies of questionnaire were administered to obtained information on patients’ socio-demographic data and healthcare facilities accessibility; respondents’ outcomes were subjected to descriptive and chi-square test at significance p<0.05. The findings of the socio-demographic characteristics of diabetes patients revealed a significant difference in ethnicity (X2=17.468), education (X2=33.790) across the wards in each LGA; patients above 40years accounted for 72.4% and 71.8% cases in the study area. Findings shown the ratio of Female to Male were 65.5% to 34.5% of diabetes prevalence; accessibility buffer map shows that patient come from afar (30km) for treatment whereas facilities are more accessible to patients’ with 5km zone. Results revealed that Sabo/Ilare (29.31%) and Okerewe 1 (34.4%) accounted for extreme patient’s concentration Ife Central and Ife East respectively. The prevalence of diabetes is relatively high in Ile-Ife Metropolis considering the variation of cases in the wards examined. Accessibility to healthcare facilities by some patients is cumbersome as medical facilities are unavailable in rural area of the study. A record of diabetes prevalence has necessitated the need for improved health services in the study area and intensifies awareness programmers as future control measures of diabetes disease.
Introduction
Globally, diabetes is rapidly on the increase especially among the urban population where the natures of food items and lifestyles have facilitated the spread of the disease [1, 2, 3, 4]. Abubakaria AR, et al. [5] and Chalkias C, et al. [6] stated that incidence of diabetes mellitus is on the high side in Africa owing to the socio-economic difficulties and radical lifestyle introduced by western world [7]. Dales RE, et al. [8] established diabetes to be having an acute complication leading to heart related disease or stroke; and this is true reflection of the Nigerian situation [9, 10, 11]. Christian HE, et al. [12] described diabetes as a localized health problem which requires quality information of the illness in such geographic location [13]. Considering the impact on diabetes on health and financial implication, diabetes has high financial weight on the patient and reflected on the economic cost of the Country’s health system. This has made diabetes a great public health concern to medical practitioners and Institutional authorities in recent time [14, 15, 16]. World Health Organization [17] accounted for about 425 million individuals living with diabetes; with a projection of about 592 million people globally by year 2035 [18, 19].
In Nigeria, prevalence of diabetes has been estimated to be over 7.5 million persons [20]. By implication, diabetes disease is spreading significantly in the country. Governments, NGOs, and information providers have geared-up concern and attention toward the disease [7, 21, 22]. More importantly, educating people through awareness campaigns against the disease will be helpful; meanwhile, the affected individuals will be better managed by adopting new lifestyles [23, 24, 25]. Diabetes assessment has become imperative through the quantification of socio-demographic data, regional economic development and medical facilities [26, 27]. More recently, Geographic Information Systems (GIS) have been observed to be useful in the health care application and identification of prevention strategies is essential [28]; Zhou M, et al. [29] reported the application of GIS tools in assessing health facilities by diabetes patients and implementation of healthcare services and programs [30]. This is manifested in tracking disease spread, spatial relationships and pattern of improving public health via GIS integrated approach [6, 31]. Advancement of GIS mapping tools have facilitated increased awareness and better opportunities for public health facilitators for monitoring the disease capabilities [32, 33, 34].
Several existing studies have reported the geographical variance in diabetes disease burden [28]. Kolawole BA, et al. [35] evaluated the geographical variations of diabetes incidence among teenagers in the Nigeria [2]. Interdisciplinary collaboration studies have shown that meteorological and geo-environmental variable have potential influences on diabetes prevalence [4, 36, 37]. Similar studies on geospatial correlation between risk factors and population effects on diabetes were conducted in Nigeria [10, 22, 38]. However, there has been little investigation into the spatial patterning of the diabetes in Ile-Ife. Basic understanding of influencing factors on prevalence of diabetes can help to generate control measures on risk associated to diabetes. Information about the disease patients, treatment regimens and accessibility to health facilities can be effective in formulating new policies on curbing the disease [14, 39]. Rong S, et al. [15] believed that factors contributing to diabetes prevalence is multi-faceted and complex; considering the differences in location, age, ethnicity, social lifestyles of people across the globe [40, 41, 42]. With unprecedented volumes of diabetes cases in Nigeria, integrated approach needs to be applied considering wide dimensional characteristics of diabetes menace in developing countries such as Nigeria; hence the study. The study will recreate scientific approach of data-driven techniques in discovering socio-demographic characteristics; spatial occurrence of diabetes patients and its prevalence towards ensuring the need for better opportunities of healthcare services of diabetes patients in Nigeria.
Objectives of the Study
The specific Objectives for the study are to:
- Examine the influence of socio-demographic characteristics on diabetes patients.
- Assess the spatial pattern of the prevalence of diabetes.
- Map the pattern of health facilities accessibility to the diabetes patients.
Materials and Methods
Study Area: Ile-Ife
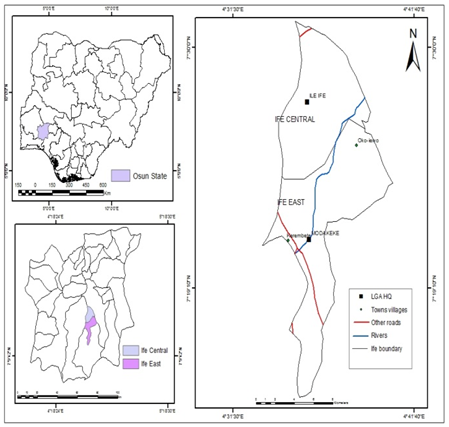
Ile-Ife Figure 1 is located in Osun State, South Western Nigeria. Ile-Ife is urban centre and the ancient Yoruba Empire known for her foremost centre of civilization globally. Ile-Ife is located within Latitudes and Longitudes (7°34’, 4°29’N); (7°37’, 4°32’N) and (7°32’, 4°35’ E), (7°28’, 4°34’E) respectively. Ile-Ife has a height ranging from 215 m to 457 m above sea level [43]. The study cut across two Local Governments Areas (LGA) namely Ife Central and Ife East with their headquarters at Ife and Oke-Ogbo respectively. The population distribution of the two LGA is 167,254 peoples and 188,027 people respectively; projected population by 2023 is at 394,863 people and 418,914 people respectively.
The climate is tropical with the rainy season between April to October while the dry season span between October to March annually. Ile-Ife Province has an annual temperature range from 27°C to 34°C annually and annual rainfall of 1340 mmyr-1. The notable institutes within Ile-Ife include: Obafemi Awolowo University (OAU), OAU Teaching Hospital, Seventh- Day Adventist Hospital, Grand Resort, Ojaja Mall and host of others. Naturally, Ile Ife has demystified her relevance and a major player in the socio-cultural and economic development of Nigeria. As such, pattern of population influx and urban growth is rapid owing to socio-economic opportunities in Ile-Ife and its environs.
Data Source
The study was conducted using primary and secondary data sources. Secondary data include: Topographic sheet of the study area, the study area ward map which was geocoded based on the respondent street location, Population figure for Ile-Ife and hospital records. Hospital records were obtained from the following sources: OAU Teaching Hospital and Seventh-Day Adventist Hospital, Ile-Ife. However, the collection of data was restricted to the urban area of Ife Central unlike non-availability of reliable sources of data in the rural areas of study area. The questionnaire administration was conducted on patients’ visiting days between the periods of eight months (March - November, 2022).
Data Processing and Spatial Analysis
The study was conducted topographic map of Ile-Ife which was scanned and geo-referenced on WGS_1984 as the base map for the study. In addition, existing digital administrative map of Osun shape-files were used to create Osun boundary, local governments, settlements, road network and other features in ArcGIS (10.4) environment. Medical records of in patients with diabetes-related discharge diagnoses were reviewed and abstracted. Such relevant attributes are as follows; admission date, inventory of diabetes in the past, patience alcohol intake, or tobacco use, diagnosis record, hereditary or family history, underlying disease, demographic data and socio-economic information. These were chosen to be assessed as potential predictors of geographic distribution of diabetes as reviewed in the literatures. Geo- database was developed using the information gotten from health centers in Ms-Excel 2016 software and saved as dBase file format before join operation of tables was carried out in a GIS environment to enable the researcher achieve objective one. The information on the attribute table of the spatial geo database developed was used to analyze, examine the socio-economical characteristics (Gender, sex, ethnic group, marital status) of diabetes patient admitted from 2010-2012. Details about patient’s addresses and medical inventories were grouped and geocoded according to the clinic ward map so as to maintain patients’ confidentiality and conformance with professional ethics rule.
Population Data and Analysis
The study engaged primary data using semi-structured questionnaire which was administered within the selected wards of the study area. The population sample were diabetic patients who attended the diabetic clinic at the OAUTHC, Ile-Ife; and Seventh Day Adventist Hospital, Lagere during the time of study. In all, two hundred (200) copies of questionnaire were administered but one hundred and eighty-three (183) copies of questionnaires were successfully retrieved. Stratified purposive sampling method was adopted for the questionnaire administration. The study area was classified into 19 wards; Ife Central Local Government Area accounted for twelve (12) wards which were: Adesanmi Estate, Ikoyi Quarters, Eleyele, Igboya, Sabo/Lagere, OAU Campus, Mayfair, Akarabata, Ojoyin, Ilare, Moore/Iremo and Ajebandele. On the other hand, Ife East accounted for seven (7) wards Local Government Area which include: Okerewe 1, Okerewe 2, Okerewe 3, Yekemi, Ilode 1, Ilode 2 and Moore. Medical officials in the respective Clinic were helpful in purposive selection and announcement of the questionnaire’s recipient both at the (Ife Central and Ife
East); the administering of questionnaire went on among these patients located within these two LGA for the study.
The analytical and statistical tools used for this study were descriptive tools and geospatial analysis. The descriptive tools used include frequencies, and percentage. Statistical software known as Statistical Package for the Social Sciences (SPSS) was employed to analyze the obtained data from the administered questionnaire using the statistical test of chi- square in analyzing the respondents’ outcomes at a p-value (0.05) to know the level of significance for the calculated values. Chi-Square is represented mathematically: X2 cal=Σ / Expected frequency;
Therefore,
$$ X ^ {2} = \Sigma \frac {(O - E) 2}{E} $$
Equation (1)
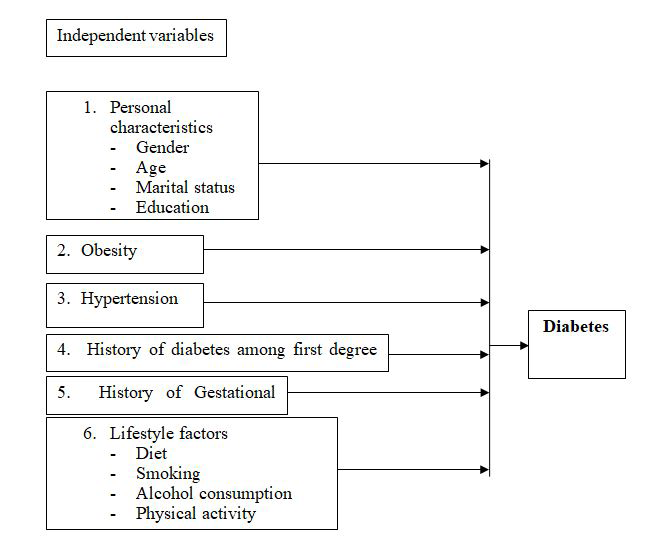
Study Framework
The methodological flowchart of the study is shown in figure 2. The stepwise procedures will include the following steps. At first, the statistical tests were employed to test the outcomes of the respondents and derived the mean values, this will help to discovered the spatial patterns of diabetes distribution in the study area. This spatial analysis on ArcGis Environment has helped to ascertain patterning of diabetes prevalence and their accessibility to healthcare facilities. GIS Application have been instrumental to analyzing diabetes prevalence and spatial regression model. In addition, the relationship between the diabetes prevalence and location of healthcare facilities revealed the proximity of patient to quick medical care; thus, help to identify and extract significant relationship of diabetes. The socio-demographic parameters have revealed some of the players contributing to incidence and management of diabetes disease in the study area.
Results
Socio-Demographic Characteristics of Diabetic Patients
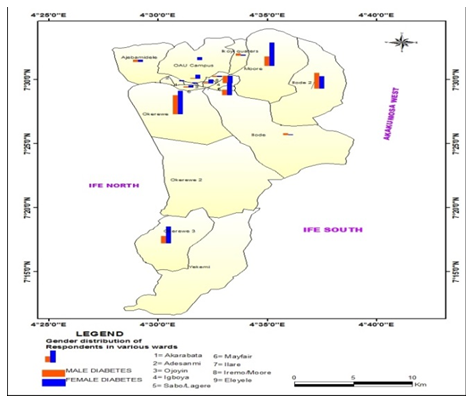
The results showed the gender and socio-economic characteristics of each Local Government Area and their wards. In Ife East, Okerewe ward 1 has the highest female percentage with 17.6%, followed closely by Moore having 16.8%; Okerewe 3 has 12.8% while the other wards have low percentages. Okerewe 1 also have the highest male percentage with 16.8%, followed by Moore with 11.2% and Okerewe 3 having 6.4% respectively. Ife Central has 12.06% male percentage in Igboya, closely followed by Sabo/Ilare 8.62% with other wards having lesser percentages, while on the Female counterpart, Sabo/Ilare has the highest percentage with 20.68%, followed by Igboya with 12.06%. Weighing the two Local Government Area together, we found out that Ife East has the highest number of males (16.8%) while Ife Central has the highest female percentage (20.68%).
Female gender is higher than Male Gender when considered the total number of patients sampled. Generally, the ratio of female to male at Ife East Local Government Area was about 51.2% to 48.8%, with Okerewe 1 having the highest with 34.4%, Moore with 28.8%, Okerewe 3 having 19.2%, Ilode 2 with 14.4% though it has more males than females and Ilode 1 with 3.2%. While in Ife Central Local Government Area, females are predominant in the wards for both LGAs except for Ikoyi quaters where we have male dominance with 5.17%, followed by Sabo/ Ilare with Female majority of 29.31%, Igboya with 24.2%, Eleyele with 8.6% and Ilare with 8.7%. The ratio of Female to Male was about 65.5% to 34.5%. In contrast Ife Central has the highest Female compared to Ife East (65.5% and
51.2% respectively) while for the Male Ife East has the highest with (48.8% to 34.5% respectively). The result high prevalence among the >60years in Ife Central unlike diabetes prevalence among the young adult in Ife East of the study area. This supported the findings Coogan PF, et al. [39] who observed that diabetes cut across all ages and womenfolk remain the great prey of diabetes. Women are more liable to develop diabetes during pregnancy [36]; as diabetes manifested in women who are more genetically vulnearable [44].
| Age Groups | ||||||
|---|---|---|---|---|---|---|
| Ife Central Wards | 18-28 | 29-39 | 40-50 | 51-61 | 62-72 | >73 and above |
| Ikoyi Qtrs | -- | 2 | 1 | -- | -- | -- |
| Ojoyin | 1 | -- | -- | -- | -- | -- |
| Akarabata | 1 | -- | 1 | -- | -- | -- |
| Mayfair | -- | 1 | 1 | -- | 1 | -- |
| OAU Campus | 1 | 2 | -- | -- | 1 | -- |
| Ajebamidele | -- | 1 | 2 | 1 | -- | -- |
| Sabo/Ilare | 2 | 2 | 3 | 2 | 9 | -- |
| Igboya | 3 | -- | 3 | 2 | 2 | 1 |
| Eleyele | 1 | 1 | -- | 1 | 2 | -- |
| Moore/Iremo | 1 | 1 | -- | 1 | -- | -- |
| Ilare | -- | 2 | 2 | -- | 1 | -- |
| Adesanmi | -- | -- | -- | -- | -- | -- |
| Total | 10 | 11 | 13 | 7 | 16 | 1 |
| Percent (%) | 17.2 | 19 | 22.5 | 12.1 | 27.5 | 1.7 |
| Ife East Ward | 18-28 | 29-39 | 40-50 | 51-61 | 62-72 | >73 & above |
| Okerewe1 | 2 | 4 | 6 | 18 | 9 | 1 |
| Okerewe2 | -- | -- | -- | -- | -- | -- |
| Okerewe3 | 1 | 1 | 6 | 7 | 7 | 2 |
| Yekemi | -- | -- | -- | -- | -- | -- |
| Ilode1 | 1 | -- | -- | 2 | -- | -- |
| Ilode2 | 4 | 5 | 7 | 6 | 4 | 1 |
| Moore | 9 | 4 | 4 | 4 | 6 | 4 |
| Total | 17 | 14 | 23 | 37 | 26 | 8 |
| Percent (%) | 13.6 | 11.2 | 18.4 | 29.6 | 20.8 | 6.4 |
Table 1: ** Age Distribution of the Study Area.
Source: Field work 2022 Table 1: Age Distribution of the Study Area.
Ethnic Distribution of the Diabetes Patients in the Study Area
Table 2 showed the diabetes prevalent within the study area findings show that there was more prevalent among the Yorubas’ (72.4%) of Ife Central while Ife East Local Government Area accounted for 71.2%. Other ethnic groups were Igbo 26.4% and Hausa 2.4% respectively, while for Ife Central similar results were obtained with 72.4% being Yorubas, 24.1% Igbos while 3.5% were from Hausa origin. A
chi-square test was further carried out to find out if there was significant difference in ethnicity across the wards in each LGA; the result showed that there was significant difference with (X2=17.468, p<0.05).
| Ife Central Ward | Igbo | Yoruba | Hausa | Ife East Ward | Igbo | Yoruba | Hausa | |
|---|---|---|---|---|---|---|---|---|
| 1 | Ikoyi Qtrs | 1 | 1 | 1 | Okerewe1 | 7 | 32 | |
| 2 | Ojoyin | -- | 1 | -- | Okerewe2 | -- | -- | -- |
| 3 | Akarabata | - | 1 | -- | Okerewe3 | 3 | 19 | 3 |
| 4 | Mayfair | 1 | 2 | -- | Yekemi | -- | -- | -- |
| 5 | OAU Campus | 1 | 2 | -- | Ilode1 | 2 | 1 | -- |
| 6 | Ajebamidele | -- | 4 | -- | Ilode2 | 11 | 16 | -- |
| 7 | Sabo/Ilare | 3 | 14 | -- | Moore | 10 | 21 | -- |
| 8 | Igboya | 5 | 8 | 1 | Total | 33 | 89 | 3 |
| 9 | Eleyele | 1 | 4 | -- | Percent (%) | 26.4 | 71.2 | 2.4 |
| 10 | Moore/Iremo | 1 | 1 | -- | ||||
| 11 | Ilare | 1 | 4 | -- | ||||
| 12 | Adesanmi | -- | -- | -- | ||||
| Total | 14 | 42 | 2 | |||||
| Percent (%) | 24.1 | 72.4 | 3.5 |
Table 2: Ethnic Distribution of Diabetes Patient for Ife Central and Ife East.
Source: Field work 2022 Table 2: Ethnic Distribution of Diabetes Patient for Ife Central and Ife East.
Educational Levels of the Diabetes Patients in the Study Area
Findings shown in Table 3 revealed that diabetes was more frequent with College/University educational status leavers (Literate) with 62.4% in most wards, 29.6% went to secondary, 4.8% went to primary while 3.2% went further for post graduate. While for Ife Central 77.6% are university leavers, 18.97% secondary school graduates while 3.5% are post graduate holders. A chi-square test was carried out to find out if there was significant difference in educational level across the wards in each LGA. The result showed that there was significant difference with (X2=33.790, p<0.05).
| Ife Central | Ife East | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Wards | Pri | Sec | Undergrad | P.G. | Wards | Pri | Sec | Undergrad | P.G. |
| Ikoyi Qtrs | -- | 1 | 2 | -- | Okerewe1 | 2 | 7 | 29 | 4 |
| Ojoyin | -- | -- | 1 | -- | Okerewe2 | -- | -- | -- | -- |
| Akarabata | -- | -- | 1 | -- | Okerewe3 | 2 | 3 | 19 | -- |
| Mayfair | -- | -- | 3 | -- | Yekemi | -- | -- | -- | -- |
| OAU Campus | -- | -- | 3 | -- | Ilode1 | -- | 3 | -- | -- |
| Ajebamidele | -- | 1 | 3 | -- | Ilode2 | 2 | 15 | 10 | -- |
| Sabo/Ilare | -- | 3 | 14 | -- | Moore | 2 | 9 | 20 | -- |
| Igboya | -- | 3 | 9 | 1 | Total | 6 | 37 | 78 | 4 |
| Eleyele | -- | 1 | 4 | -- | Percent (%) | 4.8 | 29.6 | 62.4 | 3.2 |
| Moore/Iremo | -- | 1 | 1 | 1 | |||||
| Ilare | -- | -- | 4 | -- | |||||
| Adesanmi | -- | -- | -- | -- | |||||
| Total | -- | 11 | 45 | 2 | |||||
| Percent (%) | -- | 18.97 | 77.6 | 3.5 |
Table 3: Educational Distribution for Ife Central and Ife East.
Source: Field work 2022 Pri. =Primary; Sec.=Secondary; Undergrad. =Undergraduate and P.G.=Post Graduate Table 3: Educational Distribution for Ife Central and Ife East.
Spatial Pattern of Diabetes Prevalence in the study area
Generally, diabetic patients emerge virtually from all nooks and crannies of Ile-Ife town to the hospital for treatment, but as each local government area has been classified into wards, we have some higher percentages in some wards than other wards. Specifically, in Ife Central LGA, Sabo/Ilare patients have the extreme concentration percentage with 29.31%, followed by Igboya with 24.12%. The remaining wards have low percentages within a similar range.
| Ife Central | Ife East | ||||
|---|---|---|---|---|---|
| Wards | Frequency | % | Wards | Frequency | % |
| Ikoyi Quarters | 3 | 5.17 | Okerewe I | 43 | 34.4 |
| Ojoyin | 1 | 1.73 | Okerewe II | -- | -- |
| Akarabata | 1 | 1.73 | Okerewe III | 24 | 19.2 |
| Mayfair | 3 | 5.17 | Yekemi | -- | -- |
| OAU Campus | 3 | 5.17 | Ilode I | 4 | 3.2 |
| Ajebamidele | 4 | 6.9 | Ilode II | 18 | 14.4 |
| Sabo/Ilare | 17 | 29.31 | Moore | 36 | 28.8 |
| Igboya | 14 | 24.12 | |||
| Eleyele | 5 | 8.6 | |||
| Moore/Iremo | 2 | 3.5 | |||
| Ilare | 5 | 8.7 | |||
| Adesanmi | -- | -- |
Table 4: ** Case Number of Diabetic Patients in the Study Area**.**
Sources: Field work 2022 Table 5: Case Number of Diabetic Patients in the Study Area.
Ife East though has just fewer wards but has the extreme concentration percentage of diabetic cases in Okerewe 1 having 34.4%, followed by Moore having 28.8%. The least percentages were recorded in Ilode 1 (3.2%). Comparing these two Local Government Area together, Ife East has the highest prevalence percentage. Diabetic cases are extremely concentrated in Okerewe 1 with 34.4% cases, Sabo/Ilare with 29.31%, Moore with 28.8%, Igboya with 24.12%, Ilode 2 with 14.4% with fewer or no patients within Ilode 1, Okerewe 2, Yekemi and Adesanmi wards respectively.
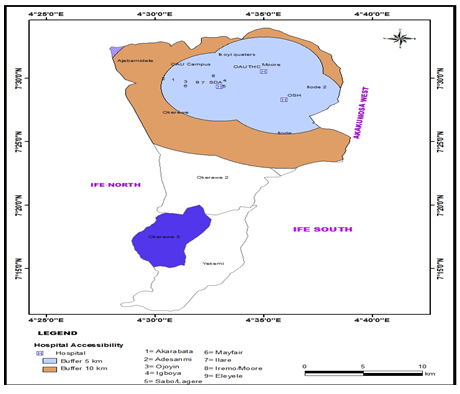
Spatial Accessibility of Diabetic Patients to Healthcare Facilities
The WHO standard for patient distance to the place of treatment for diabetes is 5km; finding from map (Figure 3) revealed that places within the 5km buffered zone of the teaching hospital were the regions with the very high prevalence of diabetes in Ile-Ife, these regions are Moore, Sabo/Lagere, Igboya and Okerewe 1, regions with the high prevalence too, which are Ilode 2, and OAU campus while the region of medium prevalence which are Ilode 1, Ikoyi quarters, Akarabata, Ojoyin, Mayfair, Ilare, Iremo/Moore and Eleyele region respectively. The other 10km buffered region of the teaching hospital was found out to have enclosed both the very high prevalence and medium regions of the prevalence of diabetes in Ile-Ife. Findings from the map (figure 3) show that areas that fall outside of the buffered regions are far to the place of healthcare facilities indicating uneasy accessibility to health facilities.
Discussion
This study focused on the existing socio-demographic characteristic of diabetes and its prevalence in Ife, Nigeria. The study found that these influencing characteristics such as age, gender, ethnicity, educational level have varied significantly at p<0.05. Also, reported cases of diabetes prevalence is relatively high in Ile-Ife Metropolis considering the variation of cases in the two local government areas which has been classified into wards, yet the study recorded higher percentages in some wards than other wards. This observed socio-demographic characteristic tallied with findings of Chalkias C, et al. [6]; Kironji AG, et al. [44] described the manifestation of diabetes in women than men. Grintsova O, et al. [40] further highlight craves for food intake during pregnancy could lead to diabetes incidence in women. William ED, et al. [23] affirmed that personal identity, societal expectations and cultural ideologies have been established a great influence in diabetes prevalence globally [15].
Furthermore, Coogan PF, et al. [39] reported that diabetes prevalence is high as the population ageing. Patricia O, et al. [33] confirmed old age can contribute to diabetes risk. In other studies, Fretts AM, et al. [3]; Zhou M, et al. [29]; Li J, et al. [25] reiterated that age advancement has shown increasing trends of diabetes in both men and women globally. Report evidences: Federal Ministry of Health [9]; Abubakaria AR, et al. [5]; National Diabetes Statistics [20] reported that national record of diabetes in Nigeria was calculated to be 6.8% in every adult of 40 years and above; indicating about 3-to-4-fold rise in diabetes risk after the age of 44years. The deteriorating of insulin resistance with age and unfitting healthcare facilities in Nigeria have contributed to the incessant rise in diabetes prevalence [8, 16, 45]. Dimensionally, discovered that lifestyle and human habit have significant influence on prevalence of diabetes as Salois MJ, et al. [46]; Kyei-Nimakoh M, et al. [41]opined that diabetes can affect both the rich and poor masses. By implication, socioeconomic status and lifestyle is an associate factors of diabetes risk [46, 47]. Geographical accessibility factors are considered to be an hinderance to many diabetes patients [44]. Walker JJ, et al. [24] discoursed the opportunities toward quality medical treatments, typical transport timeliness and road connectivity of a spatial buffers in-around the treatment facilities is required for management of diabetes disease [18]. Issa BA, et al. [36]; Hipp JA, et al. [28] reported that population increase is tantamount to urban connectivity index. The pattern of urbanization in-line with Hierink F, et al. [30] demonstrated that the Diabetes prevalence occurred in geographic areas of indigenous people concentration [42]. This finding corroborated with studies: Coberley C, et al. [21]; William ED, et al. [23]; Hou L, et al. [4]; Li J, et al. [16] expatiated the relevance of hospital facilities as preventable resources for diabetes management in a timely manner. Thus, high numbers of hospitalizations within spatial distributions serve as indicators for better healthcare delivery in regions of high diabetic cases [13, 32, 48, 49, 50, 51, 52].
Conclusion
This study offers point view for the local authority management of all diabetes patients in the Health Information System (HIS) database and Spatial Connectivity System (SCS) within an urbanized environment. This will help to build a local patient database and follow up information prevention programs and policies for disease management. Evidence of geographic disparities exists in the local government and as such pose a common risk factor to the urban population. The disparities existing in medical facilities availability among the regions and socioeconomic classes varied significantly. However, this study has made a modest contribution by examining prevalence of diabetes in the local government and how to advance public/private partnership in management strategies for diabetes disease in the study area. This study will support several reports on access to healthcare facilities which are doused by socio- economic status, level of education, employment status and geographic location of patient, health care practitioner and health care facilities. Moreover, road network measure is highly important to health care practitioners, administrators and most importantly to patients. More so, early prevention mechanism will be geared toward controlling early life blood pressure of the local people thorough the roles of primary healthcare clinics. The programme will be structured to create diabetes awareness, upgraded acknowledgement and exclusion of diabetes associated stigma obtainable vis- viz-vis: Face, Arm, and Speech Test (FAST). Furthermore, regular and in-service training will be conducted for healthcare administrators towards the recognition, education and management of diabetes. This strategy will be comprehensive to ensure progressive sensitization of rural and urban populace aimed at reducing diabetes prevalence in the country.
Conflict of Interest
The authors declare no conflicts of interest relevant to this study.
Availability of Data
The data used in this study are available from corresponding author upon reasonable request.
References
-
Centers for Disease Control and Prevention (2005) National diabetes fact sheet.
-
Bello-Sani F, Anumah FEO (2009) Electrocardiographic abnormalities in persons with type 2 diabetes in Kaduna, Northern Nigeria. International Journal Diabetes & Metabolism 17(3): 99-103.
-
Fretts AM, Howard BV, Kriska AM, Smith NL, Lumley T, et al. (2009) Physical activity and incident diabetes in American Indians: The Strong Heart Study. American Journal of Epidemiology 170(5): 632-639.
-
Hou L, Li M, Huang X, Wang L, Sun P, et al. (2017) Seasonal Variation of Hemoglobin A1c Levels in Patients with Type 2 Diabetes. International Journal of Diabetes in Developing Countries 37(4): 432-436.
-
Abubakaria AR, Bhopalb RS (2008) Systematic review on the prevalence of diabetes, overweight/obesity and physical inactivity in Ghanaians and Nigerians. Public Health 122(2): 173-182.
-
Chalkias C, Papadopoulos AG, Kalogeropoulos K, Tambalis K, Psarra G, et al. (2013) Geographical heterogeneity of the relationship between childhood obesity and socio- environmental status: Empirical evidence from Athens, Greece. Applied Geography 37: 34-43.
-
International Diabetes Federation (2012) Definition Diagnosis and Classifications of Diabetes Mellitus, pp: 1-5.
-
Dales RE, Cakmak S, Vidal CB, Rubio MA (2012) Air Pollution and Hospitalization for Acute Complications of Diabetes in Chile. Environment International 46: 1-5.
-
Federal Ministry of Health (2004) Revised National Health Policy. Nigeria, pp: 20-24.
-
Oguntola S (2011) Why men develop diabetes more easily than women.
-
Eze IC, Hemkens LG., Bucher HC, Hoffmann B, Schindler C, et al. (2015) Association between ambient air pollution and diabetes mellitus in Europe and North America: Systematic review and meta-analysis. Environmental Health Perspectives 123(5): 381-389.
-
Christian HE, Bull FC, Middleton NJ, Knuiman MW, Divitini ML, et al. (2011) How Important is the Land Use Mix Measure in Understanding Walking Behavior? Results from the RESIDE study. International Journal of Behavioral Nutrition and Physical Activity 8(1): 55.
-
Kelly C, Hulme C, Farragher T, Clarke G (2016) Are Differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. Bio- Medical Journal 6(11): 13059.
-
Dinca Panaitescu S, Dinca Panaitescu M, Bryant T, Daiski I, Pilkington B, et al. (2011) Diabetes prevalence and income: Results of the Canadian Community Health Survey. Health Policy 99(2): 116-123.
-
Rong S, Le C, Wenlong C, Jianhui H, Dingyun Y, et al. (2016) Multilevel analysis of socioeconomic determinants on diabetes prevalence, awareness, treatment and self- management in ethnic minorities of Yunnan Province, China. International Journal of Environmental Research and Public Health 13(8): 751.
-
Huang Y, Li J, Hao H, Xu L, Nicholas S, et al. (2019) Seasonal and monthly patterns, weekly variations, and the holiday effect of outpatient visits for type 2 diabetes mellitus patients in China. International Journal of Environmental Research and Public Health 16(15): 2653.
-
World Health Organization (2016) Global Report on Diabetes.
-
Domingueti CP, Dusse LMSA, Carvalho MdG, de Sousa LP, Fernandes AP, et al. (2016) Diabetes mellitus: The linkage between oxidative stress, inflammation, hypercoagulability and vascular complications. Journal of Diabetes and Its Complications 30(4): 738-745.
-
Jia P, Xue H, Cheng X, Wang Y (2019) Effects of school Neighborhood Food Environments on Childhood Obesity at Multiple Scales: A Longitudinal Kindergarten Cohort Study in the USA. BioMed Central Medicine 17(1): 99.
-
National Diabetes Statistics (2021) National diabetes information clearinghouse.
-
Coberley CR, Puckrein GA, Dobbs AC, McGinnis MA, Coberley SS, et al. (2007) Effectiveness of disease management programs on improving diabetes care for individuals in health disparate areas. Disease Management 10(3): 147-155.
-
Omogunloye OG (2013) Geospatial Analysis and Distribution of Records of Sicknesses/Diseases (Malaria, Diabetes, Sickle Cell Disorder, Typhoid Fever) A Case Study of the General Hospitals in Lagos State. Nigeria Journal of Medical and Applied Biosciences 5(1): 75-83.
-
Williams ED, Tapp RJ, Magliano DJ, Shaw JE, Zimmet PZ, et al. (2010) Health behaviours, socioeconomic status and diabetes incidence: the Australian Diabetes Obesity and Lifestyle Study. Diabetologia 53(12): 2538-2545.
-
Walker JJ, Livingstone SJ, Colhoun HM, Lindsay RS, McKnight JA, et al. (2011) Effect of socioeconomic status on mortality among people with type 2 diabetes: A study from the Scottish Diabetes Research Network Epidemiology Group. Diabetes Care 34(5): 1127-1132.
-
Li J, Wang S, Han X, Zhang G, Zhao M, et al. (2020) Spatio- temporal trends and influence factors of global diabetes prevalence in recent years. Social Science & Medicine 256: 113062.
-
Majgi SM, Soudarssanane BM, Roy G, Das AK (2012) Risk Factors of Diabetes Mellitus in Rural Puducherry. Online Journal of Health and Allied Sciences 11(1).
-
Faka A, Chalkias C, Montano D, Georgousopoulou EN, Tripitsidis A, et al. (2017) Association of Socio- Environmental Determinants with Diabetes Prevalence in the Athens Metropolitan Area, Greece: A Spatial Analysis. The Review of Diabetic Studies 14(4): 381-389.
-
Hipp JA, Chalise N (2015) Peer reviewed: Spatial Analysis and Correlates of County-Level Diabetes prevalence, 2009–2010. Preventing Chronic Disease 12: 1-14.
-
Zhou M, Astell-Burt T, Bi Y, Feng X, Jiang Y, et al. (2015) Geographical variation in diabetes prevalence and detection in China: Multilevel spatial analysis of 98,058 adults. Diabetes Care 38(1): 72-81.
-
Hierink F, Okiro EA, Flahault A, Ray N (2021) The winding road to health: a systematic scoping review on the effect of geographical accessibility to health care on infectious diseases in low-and middle-income countries. PLoS ONE 16(1): 21.
-
Jia P, Xue H, Yin L, Stein A, Wang M, et al. (2019) Spatial Technologies in Obesity Research: Current Applications and Future Promise. Trends in Endocrinology and Metabolism, 30(3): 211-223.
-
Allender S, Wickramasinghe K, Goldacre M, Matthews D, Katulanda P, et al. (2011) Quantifying urbanization as a risk factor for non-communicable disease. Journal of Urban Health 88(5): 906-918.
-
Patricia OO, Okoye ZSC, Isichei C (2013) Prevalence of Diabetes Mellitus in Bukuru Metropolis of Plateau State. IOSR Journal of Pharmacy and Biological Sciences 8(4): 50-56.
-
Maina J, Ouma PO, Macharia PM, Alegana VA, Mitto B, (2019) A Spatial database of health facilities managed by the public health sector in sub Saharan Africa. Scientific Data 6(1): 134.
-
Kolawole BA, Abodunde O, Ikem RT, Fabiyi AK (2009) A test of the reliability and validity of a diabetes specific quality of life scale in a Nigerian hospital. Quality of Life Research 13: 1287-1295.
-
Issa BA, Yussuf AD, Baiyewu O (2007) The Association between Psychiatric Disorders and Quality of Life of Patients with Diabetes Mellitus. Iran Journal Psychiatry 2: 30-34.
-
Tang K, Wang H, Liu Y, Tan SH (2019) Interplay of regional economic development, income, gender and type 2 diabetes: Evidence from half a million Chinese. J Epidemiol Community Health 73(9): 867-873.
-
Okeoghene AO, Chinenye S, Onyekwere A, Fasanmade O (2007) Prognostic indices of diabetes mortality. Ethnicity and Disease 17(4): 721-725.
-
Coogan PF, White LF, Yu J, Burnett RT, Seto E, et al. (2016) PM2.5 and diabetes and hypertension incidence in the Black women’s health study. Epidemiology 27(2): 202.
-
Grintsova O, Maier W, Mielck A (2014) Inequalities in Health Care Among Patients with Type 2 Diabetes by Individual Socio-Economic Status (SES) and Regional Deprivation: A Systematic Literature Review. International Journal for Equity in Health 13(1): 43.
-
Kyei-Nimakoh M, Carolan-Olah M, McCann TV (2017) Access barriers to obstetric care at health facilities in sub-Saharan Africa—a systematic review. System Review 6(1): 110.
-
Jia P, Cheng X, Xue H, Wang Y (2017) Applications of Geographic Information Systems (GIS) Data and Methods in Obesity-Related Research. Obesity Reviews 18(4): 400-411.
-
Ijaware VA (2020) GIS based Flood Vulnerability Studies for Ife Central Local Government Area, Osun State, Nigeria. Nigerian Journal of Environmental Sciences and Technology 4(1): 160-171.
-
Kironji AG, Hodkinson P, Stewart S, Ramirez T, Anest LW, et al. (2018) Identifying barriers for out of hospital emergency care in low and low-middle income countries: a systematic review. BMC Health Service Resources 18(1): 291.
-
Jeon CY, Lokken RP, Hu FB, Dam RM (2007) Physical activity of moderate intensity and risk of type 2 diabetes: a systematic review. Diabetes Care 30(3): 744-752.
-
Salois M (2012) Obesity and Diabetes, the Built Environment, and the ‘Local’ Food Economy in the United States, 2007. Economics and Human Biology 10(1): 35-42.
-
Eze IC, Foraster M, Schaffner E, Vienneau D, Heritier H, et al. (2017) Long-term exposure to transportation noise and air pollution in relation to incident diabetes in the SAPALDIA study. International Journal of Epidemiology 46(4): 1115-1125.
-
Diabetes Association of Nigeria (2021) New treatment for diabetes, pp: 1-6.
-
Di-Nicolantonio JJ, O’Keefe JH, Lucan SC (2015) Added fructose: A Principal Driver of Type 2 Diabetes Mellitus and its Consequences. Mayo Clinic Proceedings 90(3): 372-381.
-
Ezzati M, Riboli E (2013) Behavioral and Dietary Risk Factors for Non-communicable Diseases. New England. Journal of Medicine 369(10): 954-964.
-
Familoni OB, Olatunde O, Raimi TH (2008) The relationship between QT interval and Cardiac Autonomic Neuropathy in Nigerian Patients with Type 2 Diabetes Mellitus. Nigeria Medical Practitioner 53(4): 48-51.
-
Liu C, Yu Z, Li H, Wang J, Sun L, et al. (2010) Association of alcohol consumption with diabetes mellitus and impaired fasting glycaemia among middle – aged and elderly Chinese. BMC Public Health 10: 713.
- Lessons to Learn: Trees are More than the Lungs of the World
- Community Forestry Enterprises as a Model for Sustainable Forest Development: The Case Of The "Baja Tarahumara" in Chihuahua, Mexico
- Ecological and Socio-Economic Impacts of Chromolaena odorata and Mesosphaerum suaveolens, Two Invasive Alien Species in Central and Southern Benin, West Africa
- Epigenetic Sustainability: Modeling the Human Factor as a Natural Resource through Science 4.0 and the NR3C1 Biological Pilot
- Growth-at-Risk: A Framework for Assessing Economic Vulnerability
- The Rural Territory as a Socioecological System for the Management of Public Policy for Sustainable Rural Development