Effects of Complex Treatment by Use of Fetal Stem Cells on Bone Mineral Density in Postmenopausal Women
Analysis of bone mineral density index and a 10-year risk of fractures have been performed and two groups of postmenopausal women under the study were compared. Both investigated groups were randomized and conventional therapy by use of medicines including peroral administration of vitamin D3 and bisphosphonate were prescribed due to special indication. In treatment of the main group (MG), women along with standard therapy methods had been receiving treatment by use of fetal stem cells (FSCs). In accordance with the results and comparison between the groups, bone mineral density of femoral neck and trochanter became significantly higher in the group of women who underwent combined treatment with FSCs if compared to the control group (CG). Furthermore, in the MG we noted a tendency to downgrading a 10-year risk of fractures development in postmenopausal women, if compared to the CG upon randomization, where the patients received only a traditional treatment using medicines. This research aims to investigate effectiveness of complex therapy with FSCs derived from 7 to 12-week gestation fetuses and comparing such a treatment influence on certain markers of ageing process in postmenopausal women between the MG and the CG of patients. Criteria for comparing suggested a study of bone mineral density (BMD), as well as 10-year risk of fractures by Fracture Risk Assessment Tool (FRAX), which are the markers of agerelated changes of the skeletal system in women.
Introduction
Owing to significant ageing of people throughout the world and due to increasing population of postmenopausal women, the problems of osteoporosis have particularly become of vital importance. According to an estimation done by the WHO, at present, about 46% of women population living on the planet are in the age of over 45 years. A contemporary woman spends about one-third of her life in a period of post-menopause, which is infrequently associated with significant reduction of life quality owing to appearance of the range of vegetative-vascular, psychoneurotic disturbances, urogenital and cardiovascular system pathology. Diseases of musculoskeletal system and; in particular, osteoporosis is one of the most important contemporary problems. Osteoporosis affects about one- third to half of all women in the postmenopausal period [1, 2, 3]. In majority of cases, primary clinical signs of osteoporosis are low-energetic and minimally traumatic fractures remaining straight complications of this disease. With regard to likely complications, a definition of osteoporosis in the scientific literature appears as a “quiet” and “silent” epidemic. Loss of BMD is one of the most significant markers of growing older in the women. Almost each woman in her age over 65 years suffered from one fracture of the bones as minimum and following such anamnesis a risk of the next fractures appearance sharply increases [4].
Cells of osseous system, similar to the other body tissues remain in a continuous dynamic process for resorption and regeneration of bones. The process of a full bone tissue replacement in man continues up to 10 years on average. Process of renovation gradually becomes slower due to the extent of senescence and reduction of the stem cells pool participating in osteogenesis. This leads to development of osteopenia; and further occurrence of osteoporotic lesions. Decreasing of BMD index caused by a misbalance between development of the new bones from osteoblasts and a resorption of the bones by osteoclasts occurs. There is literary scientific evidence that proves interrelation between osteoporosis, extensive apoptosis and the defects of stem cells (SCs) differentiation into osteoblasts [5, 6, 7].
However, a progress of osteoporosis is caused by not only decreasing the number of stem cells in human body with age, but it also results in changing of qualitative features of such cells. Thus, in accordance with the data after the experiment carried out on the mice, an internal ageing of the skeletal stem cells (SSCs) leads to changing the signals in the niche of bone marrow and disrupts the process of differentiation of the bones and hematopoietic lineages that results in fragile bones and they begin regenerating poorly. Due to functional features, old SSCs possess a decreased bone- and cartilage- building potential, but they express high levels of pro- inflammatory and pro-resorptive cytokines [8]. In particular, mesenchymal stem cells (MSCs), extracted from the adult women with osteoporosis, showed an evident decreasing of their recruitment to the sites of fractures and lower response to anabolic BMP2 and BMP7 signals in bones [9]. In the same way, MSCs extracted from the patients with osteoporosis demonstrated their lower response to mitogenic signals (IGF-1), producing extracellular matrix and collagen type I contributed to adipogenous differentiation of MSCs into adipocellular tissue due to reduction of bone tissues [10]. All above-mentioned factors lead to bones fragility. They are considered to be a cause of numerous fractures resulting in elderly patients invalidity [11, 12].
Nowadays, a mechanism of FSCs influence on the adult recipient has not been precisely defined. However, on our opinion, most probably administered FSCs of fetuses, including MSCs and SSCs as components of the tubular bones are able to replace partially lost function of osteogenesis in women suffering from osteoporosis. FSCs, in contrast to SCs received from adult patients already suffering from osteoporosis, quickly and adequately react to the paracrine signals produced by the human organism. They also maintain property of much active production of type I collagen. Most likely, refill of SCs pool by way of FSCs injection subsequently differentiating into pre-osteoblasts and furtherly to osteoblasts and osteocytes will most efficiently contribute to activation of the processes of regenerating and slowing down bone tissue resorption. In this respect, all attempts to find a solution of the problems with age-related osteoporosis in women are still of great importance for medicine.
Materials and Methods
Study included 36 women in their post-menopause age. To determine BMD and a 10-year risk of exposure to fractures, doctors made a densitometry evaluation prior to therapy and over 9 months after treatment by use of FSCs. The mean age of postmenopausal women constituted 64.2 years, whereas an average age of patients in the period of menopause made up 47.5 years. Thus, 18 women (50%) had been initially diagnosed with the signs of osteoporosis, having the higher risk of fractures. In 10 women (27,8%) suffering from osteopenia an increased risk of fractures had been also remarkable, when in 6 women of menopausal period (22,2%) such densitometry indexes remained about normal. 27 women in the CG were randomized according to the age and due to the baseline parameters of BMD. The patients in the period of menopause had been also performed assessment for determining their BMD index.
Nowadays, a method of densitometry is the only recommended method for measurement of bone loss and a way to confirm the diagnosis of osteopenia and osteoporosis in the women. In this clinical study, our evaluation had been performed by use of the ECHОLIGHT densitometry apparatus (Italy). Assessment of BMD (g/cm2) was conducted in localization of the femoral neck and trochanter. Based on those findings, an integrative index of BMD and 10-year probability for developing generalized osteoporosis, as well as the risk of traumatic fractures (by FRAX scale) had been evaluated. All women suffering from osteoporosis and osteopenia both in the MG and the CG were prescribed bisphosphonate medicine for per os administration-Bonviva 150 mg. x 1 tab. per month.
Besides, doctors assessed 25(ОН) concentration of vitamin D in blood of the MG patients who had been administered FSCs therapy, as well as in the CG women. At present, Vitamin D3 concentration is regarded as one of the markers of ageing in the patients. In addition, it had been proved that vitamin D deficiency due to a range of mechanisms causes inflammation, cancer and cardiovascular diseases [13, 14]. Following the preliminary examination, all women under study with a diagnosed vitamin D deficit had been recommended treatment by use of Dekristol 2000 IU (Vitamin D3) in a dose of 1 tab. daily. Study had been conducted by means of analyzer Atellica IM 1600 (Germany) with application of the reagents kit Siemens Healthcare Diagnostics (Germany). The method of Enzyme-linked immunosorbent assay (ELISA) method with application of a special luminescent reagent was used by us. At the moment of visiting clinic for therapy, women did not suffer from any serious somatic pathology. The primary aim of treatment for them was overall rejuvenation.
Both groups of women underwent conventional treatment using medicines, which was prescribed due to a diagnosed pathological deviation in BMD index. The MG women along with a classical treatment received complex 3-day FSCs therapy program according to the Cell Therapy Center EmCell protocol established for the patients’ general antiaging and rejuvenation. To prepare FSCs suspensions, biological material harvested from aborted fetuses of 7 to 12 weeks of gestation had been used by the specialists [15]. The healthy women, who had been previously examined to exclude any viral or the other chemic infections donated fetal cells preparation following a pregnancy termination at the health care establishments due to social indications. All works with fetal material were performed according to the norms of legislation acting on the territory of Ukraine [16, 17, 18].
After FSCs preparing, all suspensions had been cryopreserved in liquid nitrogen at minimal temperature of (- 196 °C). All FSCs preparations contained the determined number of nucleated cells and CD34+ cell count, the number of colony-forming units (CFU), including clearly identified viability of the cells prior to cryopreservation. Defrost of FSCs had been carried out due to the standard protocol. Before administration to the patient, containers including FSCs preparations were removed from liquid nitrogen being placed to water bath for thawing at (+ 37˚С) temperature during a period of 90 seconds before their liquid phase is achieved. Following defrost, the number of nucleated cells was determined by use of flow cytometer and it constituted over 98% from the levels identified which had been obtained prior to cryopreservation of the FSCs suspension. All manipulations had been conducted with strict adherence to the rules of aseptic. Following thawing, stem cell suspensions were administered to the patient within 10 minutes.
Selection of FSCs preparations was performed individually for each patient after examination. Cryopreserved FSCs for clinical use were exposed to triple control of safety: donor’s blood, chorion fetal stem cell material and aborted fetus had been analysed at the laboratory. Bacteriology study for sterility had been conducted during 7 days at +37°С temperature inside of isolated vials and with application of Bac/ALERT automated system. A virology control was made with application of polymerase chain reaction (PCR) technique and it included checkup for 20 different infections (HIV-1, HIV-2, HBV, HCV, HGV, CMV, EBV, HHV6, HSV 1,2, HPV, Parvovirus B19, and SARS-Cov-2; checkup for Treponema pallidum, Toxoplasma gondii, Chlamydia trachomatis, Mycoplasma hominis, Mycoplasma genitalium, Ureaplasma Parvum, and Urealyticum). Intravenous drip feed infusion of FSCs containing harvested preparation obtained from fetal liver (in the dose from 0.21 till 0.56 mln/kg of viable nucleated cells per 200 mL of sodium chloride solution) had been performed in the MG patients on the 1st and the 2nd day of therapy. The procedure of stem cells administration continued 60 minutes. In addition, on treatment day 2, doctors prepared FSCs chorion suspension acquired from 7-12 weeks gestation fetuses. FSCs were administered to adipocellular tissue of anterior abdominal wall. This allowed creating a depot of preparation and to prolong time required for entering the patient’s blood stream. On the 3rd day of therapy, patients had been administered mesenchymal FSCs which possess ability to differentiate into osteoblasts, chondrocytes and adipocytes. In addition, doctors injected preneuronal stem cells, the cells of tubular bones and cartilages. Prior to therapy with FSCs all treated patients had been informed about the plan of treatment and the range of diagnostic procedures, the cell types to be used, the number of stem cells, as well as about the methods for FSCs injections. Doctors also described the most expected therapy outcomes for the patients. In order to get sufficient information on treatment, all women signed their written informed consent for FSCs therapy. Statistic processing of the results was performed in accordance with Student’s T-criterion and significance was calculated after consideration of the mean value and deviation of the results and was regarded as average arithmetic values.
Results
Dynamic of densitometry indexes in the MG women you can see in Table 1. They together with traditional treatment were administered FSCs therapy if compared to the CG patients randomized due to their age and receiving just conventional therapy. Both groups of women reported that they are in their post-menopause age period. The age when menopause began in both groups of women did not significantly differ.
| Index | MG (n=36) | CG (n=27) | ||||||
|---|---|---|---|---|---|---|---|---|
| P1* | Before treatment | Over 9 months | Р2** | Before treatment | Over 9 months | P2** | P3*** | |
| BMD (g/cm2) bone mineral density (femoral neck) | >0.05 | 0.597+0.22 | 0.712+0.28 | <0.005 | 0.604+0.3 | 0.622+0.19 | >0.05 | <0.05 |
| BMD(g/cm2) bone mineral density (trochanter) | >0.05 | 0.743+0.27 | 0.866+0.31 | <0.005 | 0.756+0.29 | 0.771+0.34 | >0.05 | <0.05 |
| BMD(g/cm2) bone mineral density (total) | >0.05 | 0.731+0.25 | 0.859+0.29 | <0.005 | 0.722+0.27 | 0.763+0.31 | >0.05 | <0.05 |
| T score (femoral neck) | >0.05 | -2.28+0.24 | -1.52+0.27 | <0.05 | -2.16+0.59 | - 2.02+0.48 | >0.05 | >0.05 |
| T score (trochanter) | >0.05 | -1.41+0.22 | -0.89+0.19 | >0.05 | -1.58+0.44 | -1.43+0.46 | >0.05 | >0.05 |
| T score | >0.05 | -1.75+0.25 | -1.01+0.26 | >0.05 | -1.81+0.22 | -1.63+0.2 | >0.05 | >0.05 |
| FRAX (10-year chance for developing fractures) Common osteoporosis (%) | >0.05 | 11.1+2.62 | 8.7+2.9 | >0.05 | 10.8+3.11 | 9.9+2.98 | >0.05 | >0.05 |
| FRAX (10-year chance for developing fractures) fracture of the thigh (%) | >0.05 | 3.15+0.57 | 2.42+0.48 | >0.05 | 2.98+0.62 | 2.79+0.58 | >0.05 | >0.05 |
Table 1: Parameters of BMD in menopausal women of the MG who underwent combined FSCs treatment (after 9 months following thera
Notes: Р1* -significant difference between women of the MG and CG prior to therapy Р2 -significant difference for each of the groups in dynamic (before and after treatment) Р3* -significant difference between women of the MG and CG following therapy Table 1: Parameters of BMD in menopausal women of the MG who underwent combined FSCs treatment (after 9 months following therapy if compared to the CG).
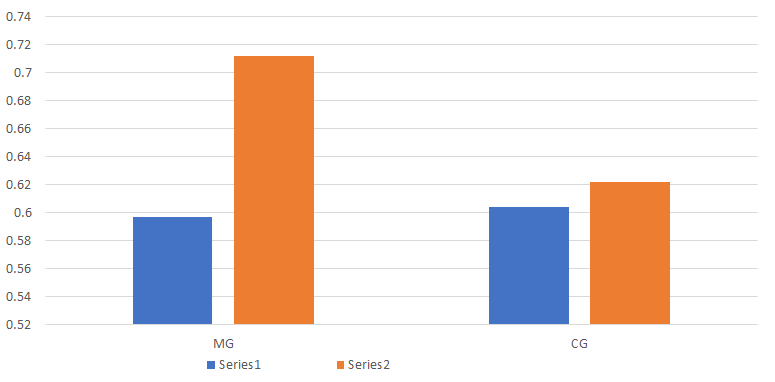
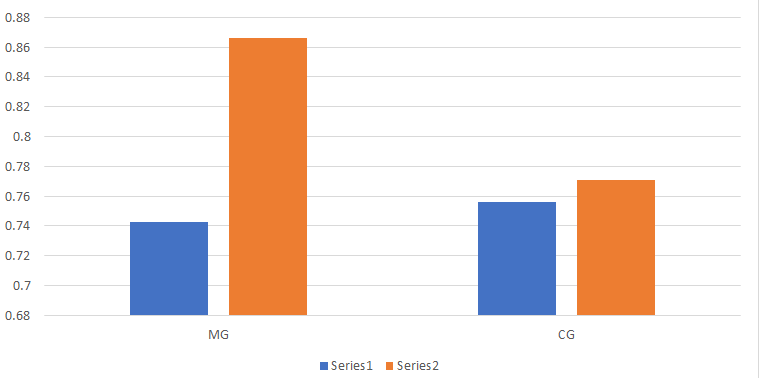
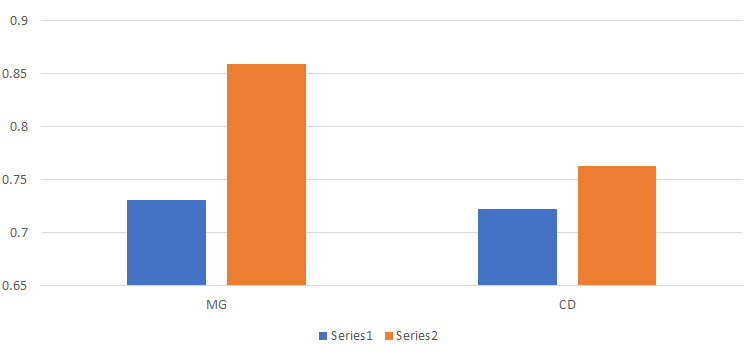
In accordance with the results after administration of vitamin D3 and peroral bisphosphonate during 9-month period of time in the CG women, the indexes of areal BMD over femoral neck increased by 8,9% on average, at the site of trochanter BMD level was 2,9% higher, whereas integrative (total) parameter of bone mineralization on average increased by 5,7% (Figure 1). The same indexes in women who underwent stem cell therapy in combination with the same dose of vitamin D3 and bisphosphonate drugs composed-19,2%, 16,5% and 17,5% respectively. BMD index on femoral neck in the MG women who had been administered FSCs was significantly higher (р<0.005).
Besides, doctors observed a significant increase of BMD in the region of trochanter (р<0.005) and higher levels of the total levels of BMD (р<0.005), whereas CG women shown changes of all such indexes which were not statistically significant (Figures 2&3).
Percentage of growing BMD on the femoral neck in the MG women was also significantly higher (р<0.05)-increased by 33,4%. Elevation of BMD on the trochanter and total mineral density were not significant in both of the groups under study. However, tendency to increasing was marked in the MG women who along with traditional therapy underwent treatment by use of FSCs. If T score (trochanter) in the CG had been increasing on average by 9,5%, women of the MG revealed elevation of this parameter by 37%. On average, T score among the CG patients was higher by 9,5%. Patients of the MG showed this score increasing by 42,3%. Most probably, lack of significance in this case was stipulated by not so large number of cases among the women who were randomized to the study. The obtained results of treatment in the patients still demand further studies and supervision in future.
10-year chance of femoral neck fractures decreased in the MG patients by 23,2%, whereas in the CG women it was lower by 6,4%. The risk of generalized osteoporosis progression decreased by 21,6% in the MG, and was 8,8% lower in the CG. Difference between the parameters of high risk in the CG and the MG women by FRAX scale had not been statistically significant (p> 0.05). However, tendency to a 10-year high risk of fractures decreasing in the group of patients who received therapy by use of FSCs preparations if compared to the results in the CG patients. BMD level elevation in the MG was most likely associated with differentiation of progenitor stromal cells into osteoblasts and faster replacement of the bone resorption sites with osseous tissue.
Conclusion
Increasing number of old and elderly people in the XXI century is an essential medical and economic problem for today. One of the supreme tasks of contemporary health care consists in both making the patient’s life span longer to continue healthier and efficient living in the elderly. On our opinion, FSCs administration, including a complex of multipotent (containing multipotent mesenchymal cells among them) and unipotent stem cells in women contributes to activation of osteogenesis processes. FSCs are much sensitive to mitogenic and paracrine signals of the organism in the women suffering from osteoporosis, if compared to the patient’s proper stem cells. Process of stem cells differentiation shifts in the direction to osteoblasts and osteocytes, but not towards adipogenesis. Therefore, production of extra-cellular matrix and type I collagen is increased.
A statistically significant decrease of a 10-year risk of femoral neck fractures and development of generalized osteoporosis have been also observed in the group of postmenopausal women, who underwent a combined therapy using FSCs along with use of vitamin D3 and bisphosphonate medicines if compared to the group of randomized patients who received only traditional treatment by such medicines. Most probably, it is associated with an activation of reparative processes in the bone tissue under the influence of progenitor stromal cells differentiation to osteoblasts. With regard to a small study volume and methodology restrictions in existing data of research, as well as degree of persuasive scientific evidence on increasing BMD and decreasing a 10- year risk of fractures which are not sufficient for present day. Nevertheless, a method of supplementary administration of FSCs together with conventional therapy methods used for treatment of osteoporosis and osteopenia in the patients tends to be a perspective direction of therapy but still requires future research in this direction.
References
-
Kanis JA, Johnell O, Oden A, Sembo I, Johnell IR, et al. (2000) Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 11(8): 669-674.
-
Riggs BL, Melton L (1986) Involutional osteoporosis. N Engl J Med 314(26): 1676-1686.
-
Povoroznyuk VV (2014) Osteoporosis in practice of intern-medical doctor. pp: 198.
-
Kanis JA, Johnell O, Laet CD, Johansson H, Oden A, et al. (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35(2): 375-382.
-
Chen HT, Lee MJ, Chen CH, Chuang SC, Chang LF, et al. (2012) Proliferation and differentiation potential of human adipose‐derived mesenchymal stem cells isolated from elderly patients with osteoporotic fractures. J Cell Mol Med 16(3): 582-592.
-
Saeed H, Abdallah BM, Ditzel N, Lehnen PC, Qiu W, et al. (2011) Telomerase‐deficient mice exhibit bone loss owing to defects in osteoblasts and increased osteoclastogenesis by inflammatory microenvironment. J Bone Miner Res 26(7): 1494-1505.
-
Shen J, Tsai YT, DiMarco NM, Long MA, Sun X, et al. (2011) Transplantation of mesenchymal stem cells from young donors delays aging in mice. Sci Rep 1: 67.
-
Ambrosi TH, Marecic O, McArdle A, Sinha R, Gulati GS, et al. (2021) Aged skeletal stem cells generate an inflammatory degenerative niche. Nature 597(7878): 256-262.
-
Haasters F, Docheva D, Gassner C, Popov C, Böcker W, et al. (2014) Mesenchymal stem cells from osteoporotic patients reveal reduced migration and invasion upon stimulation with BMP-2 or BMP-7. Biochem Biophys Res Commun 452(1): 118-123.
-
Pino AM, Rosen CJ, Rodríguez JP (2012) In osteoporosis, differentiation of mesenchymal stem cells (MSCs) improves bone marrow adipogenesis. Biol Res 45(3): 279-287.
-
Shoback D (2007) Update in osteoporosis and metabolic bone disorders. J Clin Endocrinol Metab 92(3): 747-753.
-
Stenderup K, Justesen J, Eriksen EF, Rattan SI, Kassem M (2001) Number and proliferative capacity of osteogenic stem cells are maintained during aging and in patients with osteoporosis. J Bone Miner Res 16(6): 1120-1129.
-
Papadimitriou DT (2017) The Big Vitamin D Mistake. J Prev Med Public Health 50(4): 278-281.
-
Giuggioli D, Colaci M, Cassone G, Fallahi P, Lumetti F, et al. (2017) Serum 25-OH vitamin D levels in systemic sclerosis: analysis of 140 patients and review of the literature. Clinical Rheumatology 36: 583-590.
-
Smikodub OI, Novytska AV, Markov IS (2001) Harvesting of hematopoietic stem cells from human embryonic hematopoietic organs. Ukraine.
-
(2003) Civil Code of Ukraine. CIS Legislation.
-
Smikodub OI, Arkhipenko IV, Bushnyeva VO, Demchuk MP, Novytska AV, et al. (2004) Ethical issues and norms at work with human embryonic tissues: Method. Recommendations. Kyiv, pp: 1-20.
-
(1999) Law of Ukraine about organ transplantation and other anatomic materials to the person. CIS Legislation.
- Research Progress of Induced Pluripotent Stem Cells and Their Clinical Application Prospects
- Nishan Al-Kamal is the Starting Point of A Feminist Scientist
- Current Concepts and Future Perspectives of Stem Cell Therapy in Peripheral Arterial Disease
- Stem Cell and Oxidative Stress-Inflammation Cycle
- Adipose Derived Mesenchymal Stem Cells Origin, Characteristics and Promises
- Mitochondria Targeted Antioxidants can Improve In Vitro Embryo Production in Buffalo