Case Report Blunt Trauma: An Uncommon Cause of Bile Duct Injury
Disruption of the biliary tree secondary to blunt trauma is a rare cause for extrahepatic bile duct injury [1-4]. It seldom occurs alone, hence, this type of injury is easily overshadowed by more overt surgical emergencies and may go undiagnosed, leading to complications and potentially adverse outcomes in the later course. The incidence of bile leaks following hepatobiliary trauma ranges from 0.5 to 2.1% depending on the methods used to diagnose the bile leak. We present here a rare case with injury to both IHBR (Intrahepatic Biliary Radicles) and EHBD (Extra hepatic Bile Ducts) as a consequence to abdominal trauma.
Case Report
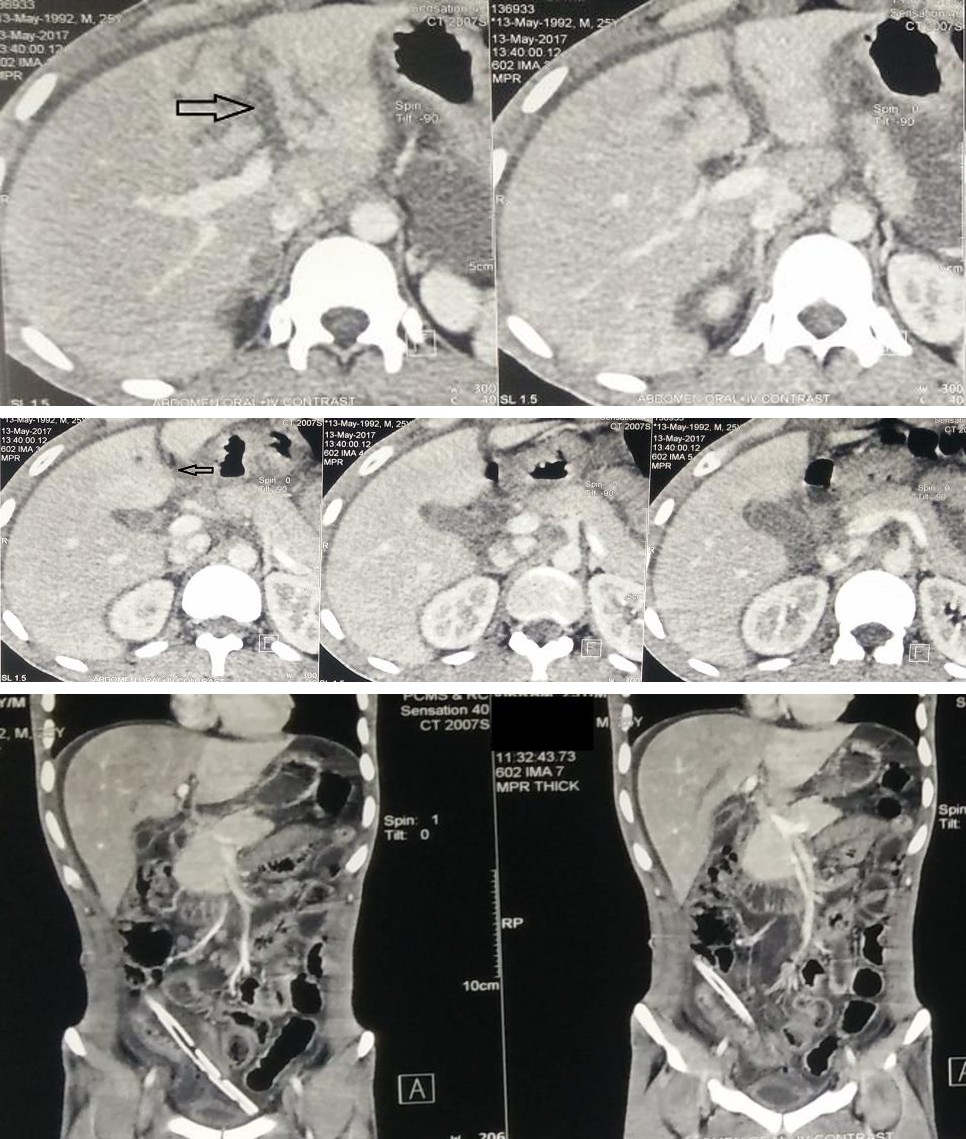
A 25yr old male presented to the emergency at around 3am with an alleged history of road traffic accident due to motorcycle collision with a heavy vehicle. On presentation, Patient was hemodynamically stable. On Gross examination, He was conscious and oriented and had no signs of any head injury. He had mild pallor and no icterus or clubbing at the time of admission.He had multiple facial injuries with unstable mandibular arch along with a split maxilla. Also,there were multiple lacerated wounds intra-orally and extra-orally but no gross injury mark over the abdomen or other regions. On per abdomen examination, the abdomen was soft with no visible distension. There was no guarding or rigidity although the patient had mild tenderness in right hypochondrium. Apart from this, the chest and pelvic compression were negative. USG abdomen suggested a small hypoechoic lesion in left lobe of liver s/o liver contusion. CECT (Contrast Enhanced CT Scan) abdomen was done which revealed a Laceration in the segment 4A of liver (around 4.6 * 3.45 cm) around the left portal vein reaching upto the liver capsule with mild-moderate hemoperitoneum (Figure 1).
Initial Blood investigations revealed Hemoglobin of 8gm/dl, Bilirubin 0.70 mg/dl,raised SGOT – 180.3 IU/L (range 5-40 IU/L) and SGPT – 189.4 IU/L (range 5-40 IU/L) and reduced Serum proteins (Total - 4.56 gm/dl, range 6.0 – 8.0 gm/dl, Albumin – 2.81 gm/dl, Globulin – 1.75 gm/dl). Patient was transfused 1 unit Packed Red blood cells and 4 units of fresh frozen plasma. The patient remained hemodynamically stable and hence was managed conservatively over the next few days. Jaundice which was absent initially developed over the next 2 days with Sr. bilirubin rising to 3.41mg/dl on post admission Day(PAD)-2, (Direct- 1.76mg/dl and indirect 1.65 mg/dl) and 3.86mg/dl on PAD-4. (Direct- 1.62mg/dl, Indirect –
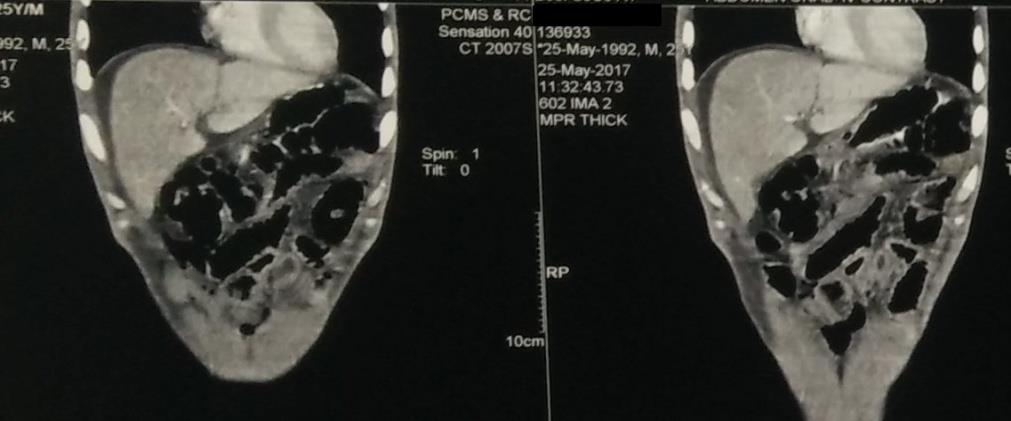
2.24 mg/dl) while the liver enzymes improved and became normal by PAD-5. On PAD-10, the patient complained of heaviness of abdomen with distension and on examination the abdomen was tense and tender. On needle aspiration, contents were bile stained and so an abdominal drain was placed under local anesthesia and around 1-1.5 Litres of bile stained fluid was drained. Repeat CECT abdomen was done which revealed partial resolution of the earlier lesion with altered morphology of the associated IHBR and left portal vein (Figure2).
Discussion
Traumatic injuries of the extrahepatic biliary tract are uncommon, with incidence ranging from 2 to 5 % in abdominal trauma, mainly affecting the gallbladder [2, 3, 5, 6]. Most lesions of extrahepatic bile ducts are caused by penetrating trauma [2, 3, 7] while IBHR injury usually results from blunt trauma with liver involvement.
The exact mechanism of injury to the bile duct after blunt trauma is not well known, but a number of factors are identified as responsible for it: (1) a shear force or stretch or avulsion that intersects the duct at its point of attachment to the pancreas or liver; (2) a short cystic duct, causing rapid emptying of the bladder when force is applied, with a sudden increase in intraductal and subsequent predisposition to injury; (3) a shear force applied to the common duct where it is already strained; (4) a compression of the ductal system against the spinal column [1, 3, 4]. Perhaps a combination of these factors promotes injury of the extrahepatic biliary system. The most frequent sites of injury to the extrahepatic bile ducts in blunt abdominal trauma are at the upper edge of the pancreas, the hepatic duct bifurcation, and in the origin of the left hepatic duct [5, 8, 9]. The clinical presentation virtually divides patients with injuries in the extrahepatic bile ducts into two groups: one with early diagnosis, where laparotomy is indicated because of the presence of hypovolemic shock and signs of peritoneal irritation or associated injuries. The second group is composed of patients with a delayed diagnosis, which are often presented with nausea, vomiting, jaundice, and abdominal pain with distension, as the case in our patient. Ultrasonography and computed tomography can result in false negative [3, 4, 10]. Although US is an operator- dependent exam, abdominal ultrasonography was performed twice bydifferent radiologists in theand no injury concerning the biliary tract was observed. The computed tomography common findings in bile duct injury are swelling in the hepatoduodenal ligament, free fluid in the peritoneal cavity, and associated injuries to the liver and duodenum.
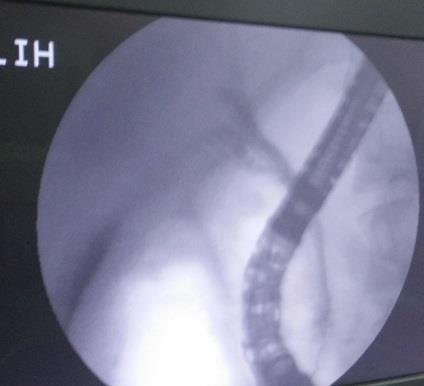
Earlier reports showed that the optimal time period from injury to repeat imaging studies for high-grade liver injuries ranges from 7 to 10 days; the mean time for complications to surface. Most bile leaks are diagnosed when a CT scan shows a collection or intra-abdominal fluid [11]. Although, the presence of free fluid is sensitive, it is non-specific for bile leak. In a recent study of liver lacerated patients, CT scanning showed 98% hemoperitoneum but only 25% had bile leak [12]. If there is no indication for early surgical treatment, the diagnosis of injuries to the extrahepatic bile duct may be delayed, as what had happened in the case [3, 4, 5]. Patients not operated on, early in time, and with a biliary fistula may remain asymptomatic for days, because the bile is a sterile component and can be well tolerated. Patients may present few symptoms including abdominal discomfort, nausea, vomiting, jaundice, ascites, and fever [13, 6]. The presence of jaundice after blunt abdominal trauma is suggestive of a missed bile duct injury, but other common diagnoses should be also considered such as massive blood transfusion, liver disease, hepatic trauma, hematoma absorption, or cholecystitis. Endoscopic retrograde cholangiopancreatography (ERCP) can diagnose and eventually treat bile duct injury with stent even if surgical procedures have been conducted before [6, 14]. Only a few patients have been reported in whom percutaneous transhepatic biliary drainage has been used for biliary leak treatment [15, 16, 17, 18]. Although, the procedure has shown efficacy, limited availability of expertise may have been an important hindrance in lack of widespread popularity. The surgical treatment of injuries to the bile ducts should be individualized, based upon hemodynamic stability, associated injuries, and upon the location and extent of the injury. Complications such as biliary fistulae, abscess, and stenosis may be reduced with early diagnosis and appropriate management during surgery. The high morbidity and mortality of these patients are related to associated injuries and their complications.
References
-
Zago TM, Pereira BMT, Calderan TRA, Hirano ES, Fraga GP (2014) Extrahepatic Duct Injury in Blunt Trauma: Two Case Reports and a Literature Review. The Indian Journal of Surgery 76(4): 303- 307.
-
Brenneman FD, Rizoli SB, Boulanger BR, Hanna SS (1994) Blunt left hepatic duct injury. Injury 25(7): 465-467.
-
Ivatury RR, Rohman M, Nallathambi M, Rao PM, Gunduz Y, et al. (1985) The morbidity of injuries of the extra-hepatic biliary system. J Trauma 25(10): 967-973.
-
Melton SM, McGwin G Jr, Cross JM, Davidson J, Waller H, et al. (2003) Common bile duct transection in blunt abdominal trauma: case report emphasizing mechanism of injury and therapeutic management. J Trauma 54(4): 781-785.
-
Nathan M, Gates J, Ferzoco SJ (2003) Hepatic duct confluence injury in blunt abdominal trauma: case report and synopsis on management. Surg Laparosc Endosc Percutan Tech 13(5): 350-352.
-
Feliciano DV, Bitondo CG, Burch JM, Mattox KL, Beall AC Jr, et al. (1985) Management of traumatic injuries to the extrahepatic biliary ducts. Am J Surg 150(6): 705-709.
-
Gerndt SJ, Seidel SP, Taheri PA, Rodriguez JL (1995) Biliary tract injury following blunt abdominal trauma: case reports. J Trauma 39(3): 612-615.
-
Balzarotti R, Cimbanassi S, Chiara O, Zabbialini G, Smadja C (2012) Isolated extrahepatic bile duct rupture: a rare consequence of blunt abdominal trauma. Case report and review of the literature. World J Emerg Surg 7(1): 16.
-
Posner MC, Moore EE (1985) Extrahepatic biliary tract injury: operative management plan. J Trauma 25(9): 833-837.
-
Ramia JM, Gutiérrez G, Garrote D, Mansilla A, Villar J, et al. (2005) Isolated extrahepatic bile duct rupture in blunt abdominal trauma. Am J Emerg Med 23(2): 231- 232.
-
Cuff RF, Cogbill TH, Lambert PJ (2000) Nonoperative management of blunt liver trauma the value of follow- up abdominal computed tomography scans. Am Surg 66(4): 332-336.
-
LeBedis CA, Anderson SW, Mercier G, Kussman S, Coleman SL, et al. (2015) The utility of CT for predicting umabile leaks in hepatic trauma. Emerg Radiol 22: 101-107.
-
Bourque MD, Spigland N, Bensoussan AL, Garel L, Blanchard H (1989) Isolated complete transection of the common bile duct due to blunt trauma in a child, and review of the literature. J Ped Surg 24(10): 1068- 1070.
-
Jones KB, Thomas E (1985) Traumatic rupture of the hepatic duct demonstrated by endoscopic retrograde cholangiography. J Trauma 25(5): 448-449.
-
Bade PG, Thomson SR, Hirshberg A, Robbs JV (1989) Surgical options in traumatic injury to the extrahepatic biliary tract. Br J Surg 76(3): 256-258.
-
Kaufman SL, Kadir S, Mitchell SE, Chang R, Kinnison ML, et al. (1985) Percutaneous transhepatic biliary drainage for bile leaks and fistulas. AJR 144(5): 1055- 1058.
-
Zuidema GD, Cameron JL, Sitzmann JV, Kadir S, Smith GW, et al. (1983) Percutaneous transhepatic management of complex biliary problems. Ann Surg 197(5): 584-593.
-
Vaccaro JP, Dorfman GS, Lambiase RE (1991) Treatment of biliary leaks and fistulae by simultaneous percutaneous drainage and diversion. Cardiovasc Intervent Radiol 14(2): 109-112.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey