Orthodontically Replacement of Canine with Congenitally Missing Maxillary Lateral Incisor – A Case Report
Substitution of canine in place of lateral incisor is one of the best treatment approaches in cases with congenitally missing or accidental exfoliation of lateral incisors. Next most commonly used is restoring missing with an implant or prosthetic bridge. Aim: The main of this article is to implicate canine substitution method for replacing missing lateral incisors without a future prosthesis. Case Report: A 17-year-old girl came with the chief complaint of irregularly erupted teeth with one side shift in an upper front region of the mouth. On Intra-oral examination, molars are in angle's class I relation, canine class I on right side and cross bite on the left side, middle line shifted on patient's left side in the maxillary arch. In the mandible, canines are into-lingual rotations. Treatment Plan: Based on the clinical situation and obtained cephalometric and model analysis values, it was planned to treat the case by space closing method. Thus, the case was planned for fixed orthodontic appliances with an extraction of three first premolars. Treatment progress: Multibracket appliance prescription of MBT TM, slot size 0.022X0.028 inches brackets were fixed with Enlight (Ormco US) primer and adhesive were used for its best strength, following manufacturer’s instructions. Canine contouring procedure: The canine tip flattened and converted in lateral incisor incisal edge, the mesial and distal edge was reduced to simulated lateral incisor. Labial prominence was flattening as a lateral incisor. A similar procedure was followed to convert canine's palatal surface to lateral incisor. Conclusion: Substituting canine with missing lateral is one of the best approaches. However, it should match color, dimensions with lateral.
Introduction
Insufficient development of tooth germ unable to differentiate dental tissue inhibits the development of teeth and resulting in to missing teeth. Various studies have been done to estimate the rate of prevalence pertaining to gender, has reported that tooth agenesis in either gender varies between 0.3 per cent and 11.3 per cent, without including third molars [1, 2, 3]. The prevalence rate of maxillary lateral incisors in south Asian countries were 3.4% found in Japanese populations, 2.7% chine, and 1.6% in Indian population. These reports conclude that one fifth of the population seen with missing lateral incisors [4, 5, 6, 7]. Etiological factor for congenitally missing lateral incisors is Heredity, ectodermal dysplasia conditions such as rickets, syphilis, and expression of evolutionary changes in the dentition. Furthermore, the possible cause may be pathologic condition or accidents [4, 5]. Treatment option for missing maxillary lateral incisors includes canine protraction or space reopening for prosthesis (implant, bridge). However, the choice of treatment depends up on the occlusal relation, profile, arch length, and tooth size discrepancies and patients desire [6, 7, 8]. The most accepted traditional method was to reopen space and close with a prosthesis, a deliberate closure may result in temporal mandibular dysfunction. Recent studies report that space closure should carry out to preserve clock wise rotation of jaw. Furthermore, space opening should be preferred in retruded jaw condition to improve the labial sagittal relationship [9, 10, 11, 12]. Present case reports suggest that molar and canine relation should be given priorities, such as in a case of molar class I or class III with canine class I should be treated with space opening. However, in the case of class II space closure is preferred; in a case of excessive crowding or arch length deficiencies extractions should be considered to obtain molar and canine in class I relationship [11, 12, 13]. Through this case report, we would like to present management of missing lateral incisor with replacing canine, with the extraction of three premolars to maintain occlusal balance and facial harmony.
Case Report
History and Etiology: A 17-year-old girl came with the chief complaint of irregularly erupted teeth with one side shift in an upper front region of the mouth. On extra oral examination, orthognathic profile, slightly anterior divergent chin with horizontal growth pattern; the lips were incompetence, shallow mento-labial sulcus, and a hyperactive mentalis. On Intra-oral examination, molars are in angle's class I relation, canine class I on right side and cross bite on a left side, middle line shifted on patient's left side in the maxillary arch. In the mandible, canines are distolingual rotations.
Diagnosis
Skeletally: Maxillary protrusion, retrusive mandible (SNA 83o, SNB 82o, ANB 1o). Dental: component Class I molar relationship, middle line shift on left side.
Treatment objectives
Skeletal components: - minimal correction were needed, safeguarding all the planes of a face such as a transverse plane, sagittal plane, and anteroposterior plane; retraction and intrusion of the anteroposterior and vertical component mandible respectively have to be done. Dental components: de-rotation, middle line shifting and retraction and intrusion, of anterior teeth with maintaining class I molars relationship.
Treatment Plan
Based on the clinical situation and obtained cephalometric and model analysis values, it was planned to treat the case by space closing method. Thus, a case was planned for fixed orthodontic appliances with an extraction of three first premolars. Transpalatal arch was given for anchorage to achieve treatment objective with no anchor loss. The permanent lingual retainer was planned after a case was debonded.
Treatment progress
Multibracket appliance prescription of MBT TM, slot size 0.022X0.028 inches brackets were fixed with Enlight (Ormco US) primer and adhesive were used for its best strength, following manufacturer’s instructions. The first phase of leveling and alignment was achieved with o.016 NITI wires. Phase second was initiated with the use of 0.019X0.025 inch gauge of NITI wire for at least two months, followed by 0.019X0.025 inch gauge of SS wire for at least two months. A primary objective was achieved with walking off canine on the right side with 0.0009 SS ligature wire (activating lace back). After right canine walked off into extracted space, with following the instruction given in MBT TM text book, the conventional maxillary arch form was fabricated and mesial to right canine omega loop was given and single tooth shifting was done to correct middle line shift from left to its original position. Left side canine was retracted in place of a left lateral incisor. In the final phase, the initial stage of this root parallelism was obtained with use of 0.019X0.025 inch gauge of NITI wire for at least two months, followed by 0.022X0.028 inch gauge of NITI wire for at least two months. Fixed lingual retainer was given in both upper and lower arch and debonding and composite removed and scaling and polishing were done. Enamel plasty was carried out with the left maxillary canine to reshape into left lateral incisor.
Canine Contouring Procedure
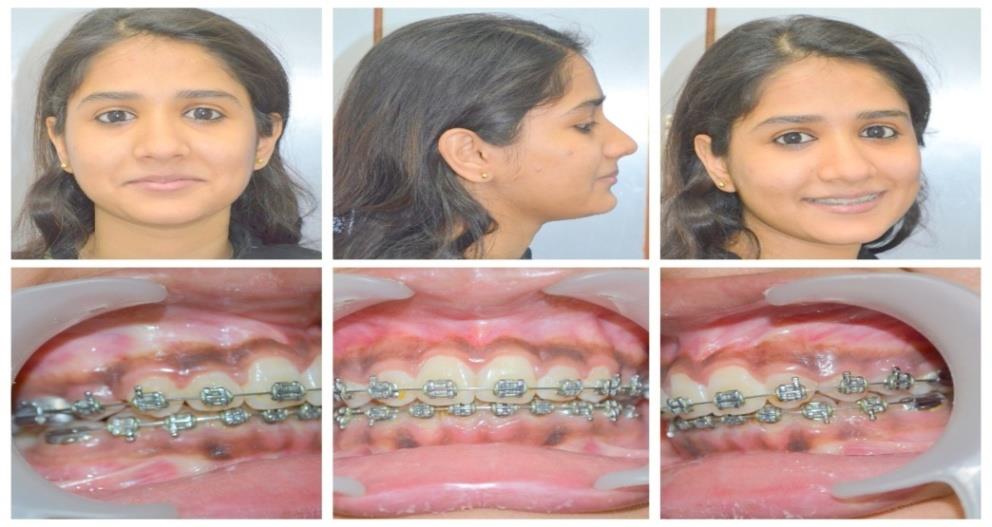
The canine tip flattened and converted in lateral incisor incisal edge, the mesial and distal edge was reduced to simulated lateral incisor. Labial prominence was flattening as a lateral incisor. A similar procedure was followed to convert canine's palatal surface to lateral incisor [14] (Figures 1-3).

Figure1: Pre treatment photographs.

Discussion
The main objective of replacing canine in place of missing later incisor was achieved along with maintaining occlusion, over jet, and overbite within the norms with; molars and canine in class I. Most of the studies have suggested that substituting canine should posses basic properties like easy to re-contour, color; labial surface should match with replacing lateral incisor. Few case reports have been suggested those high mandibular angles are more favorable than low angle [11, 12, 13, 14]. In our case we had canine shape, prominence and color were approximately similar to adjacent central incisors. Hence during enemaloplasty substituting canine became easy to simulate missing lateral incisor. Various case reports on peg shape lateral incisors suggest that extraction of peg shape lateral incisors and premolars instead of protraction of canine distal into premolar space and restore lateral incisor space with implants or other prosthetic means. Furthermore, few case reports disagree, as in a case of microdontia; reshaping was the best choice to adapt [14, 15, 16]. In our case, lateral incisor space was closed and a middle line was shifted to the left side, hence, extraction of three premolars was decided to correct middle line shift, de- rotation lower canines. Recent studies have reported that space opening should be done only in low angle cases and space closure in high angle cases. Space closing low angle case may result in clock wise rotation of lower jaw. Furthermore, in the case of retruded profiles best option was to re-open the space and restore with prosthesis 16. In our case, the profile was orthognathic and space opening would have created clock wise rotation of jaw and prognathism of complete dentoalveolar segment.
Conclusion
In situations of missing laterals choice of canine was the best option because of larger in dimension compared to lateral incisor, facilitate the significant amount of reduction to achieve acceptable esthetics and a stable occlusion. Canine has two shades, can be managed with bleaching or veneers.
References
-
O’Dowling IB, McNamara TG (1990) Congenital absence of permanent teeth among Irish school- children. J Ir Dent Assoc 36: 136-138.
-
Rosenzweig KA, Garbarski D (1965) Numerical aberrations in the permanent teeth of grade school children in Jerusalem. Am J Phys Anthropol 23(3): 277-283.
-
Fekonja A (2005) Hypodontia in orthodontically treated children. Eur J Orthod 27(5): 457-460.
-
Robert E Moyers (1988) Early treatment, handbook of orthodontics. 4th (Edn.).
-
chin-yin lin, ya-hui yang i chen, chi-ying huang, sang- heng kok, yi-jane chen, et al. (2006) Orthodontic treatment with canines substitution for lateral incisors ── cases report. J dent science 1(2): 79-87.
-
Niswander JD, Sujaku C (1963) Congenital anomalies of teeth in Japanese children. Am J Phys Anthropol 21: 569-574.
-
Davis PJ (1987) Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dent Oral Epidemiol 15(4): 218-220.
-
Haavikko K (1971) Hypodontia of permanent teeth. An orthopantomographic study. Suom Hammaslaak Toim 67(4): 219-225.
-
Wriedt S, Werner P, Wehrbein H (2007) Tooth shape and color as criteria for or against orthodontic space closure in case of a missing lateral incisor. J Orofac Orthop 68(1): 47-55.
-
Richardson G, Russell KA (2001) Congenitally missing maxillary lateral incisors and orthodontic treatment considerations for the single-tooth implant. J Can Dent Assoc 67(1): 25-28.
-
Millar BJ, Taylor NG (1995) Lateral thinking: the management of missing upper lateral incisors. Br Dent J 179(3): 99-106.
-
Argyropoulos E, Payne G (1988) Techniques for improving orthodontic results in the treatment of missing maxillary lateral incisors A case report with literature review. Am J Orthod Dentofacial Orthop 94(2): 150-165.
-
Rosa M, Zachrisson BU (2010) The space-closure alternative for missing maxillary lateral incisors :an update. J Clin Orthod 44(9): 540-561.
-
Tuverson DL (1970) Orthodontic treatment using canines in place of missing maxillary lateral incisors. Am J Orthod 58(2): 109-127.
-
Rosa M, Zachrisson BU (2001) Integrating esthetic dentistry and space closure in patients with missing maxillary lateral incisors. J Clin Orthod 35(4): 221- 234.
-
Kokich VO Jr, Kinzer GA (2005) Managing congenitally missing lateral incisors. Part I: Canine substitution. J Esthet Restor Den 17(1): 5-10.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey