Gougerot's Crossed and Confluent Papillomatosis - Carteaud: Report of a Clinical Case
The confluent and reticulated papillomatosis (CRP) described by Gougerot-Carteaud is a rare cutaneous disease of unknown etiology, which occurs mainly in young adults. There are cases of CRP worldwide and in all racial groups; is seen more frequently in women and in the white race. There is currently no accurate estimate of prevalence in the population. The clinical case of a 26-year-old female patient is referred by a hyperpigmented, slightly scaly dermatosis, predominantly in the anterior cervical region, in addition to the anterior and posterior thorax in the intermammary area and in the lumbar area. He received treatment with tetracyclines and topical retinoids with an adequate response to the treatment used.
Introduction
The People's Republic of China was first described by Gougerot and Carteaud in 1927 and 1932, respectively; is a rare and possibly under diagnosed dermatosis. It is usually present in adolescents and young adults, characterized clinically by the slow and progressive appearance of papules and hyperkeratotic plaques, finely desquamative, brown-brown in the upper trunk region: affecting the neck and intermammary area; sometimes armpits [1, 2].
Clinical Case
Reason for consultation: A 26-year-old female patient, who visits the dermatology clinic with a previous diagnosis of Mal Del Pinto. It was sent from a first level care module to the dermatology department due to the presence of hyperchromic lesions in the anterior trunk, posterior trunk, and neck with an approximate evolution time of 3 years. The injury is accompanied by itching that is exacerbated by sweating and hormonal cycles. In his family history, he had only the antecedent of the father died of prostate cancer. In their non-pathological personal history, alcoholism, smoking, and drug addiction are denied.
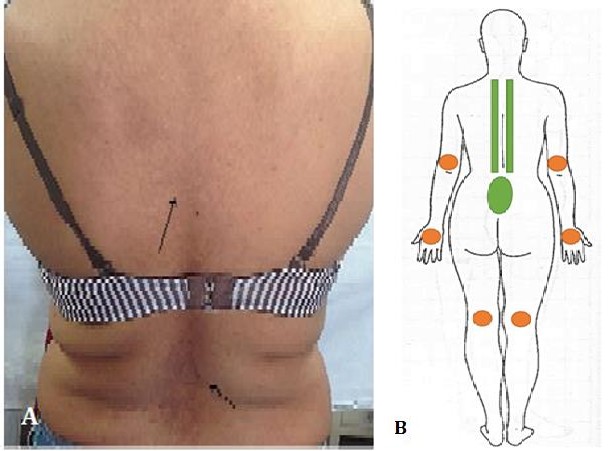
| Physical examination: Physical examination shows | ||
|---|---|---|
| hyperpigmented and scaly skin lesions with | ||
| predominance in the anterior thorax in the | ||
| intermammary area (Figure 1A) in the anterior neck | ||
| (Figure 1B, Figure 1C), in the posterior thorax in | ||
| paravertebral internal scapular lines, as well as at the | ||
| lumbar level (Figures 2A &2B). Light brown, rough-to- | ||
| touch lesions are found that converge in the median plane | ||
| to form a cross-linked papulosquamous plaque on the | ||
| periphery. |

Appropriate Therapeutic Approach
Diagnostic treatment is initiated with 1 capsule of Doxycycline 100 mg every 24 hours for 3 weeks and retinoic acid for topical application in areas affected by night. Three weeks after the start of treatment, the lesions are better observed, however, the remission of the lesion is not reached, the persistence of lesions in the lumbar area is observed.
Discussion
PRC is a rare dermatosis, which can occur mainly in young adults (between the second and third decade) [1, 3]. There have been reported cases of PRC worldwide and in all racial groups, these reports mention that it is more frequent in women, in the white race, as well as in overweight individuals [1, 2, 3, 4, 5]. Nevertheless; because it is a very rare dermatosis, is not always reported and there is currently no accurate estimate of prevalence in the population [1, 2, 3].
The morphology of PRC is usually characterized by primary and secondary lesions that form papulosquamous plaques. The papules are small, solid and circumscribed, usually blackish-brown in color, and elevated that converge in a central site forming laminae and in the periphery these lesions are dispersed maintaining some areas with the same morphology of the rest of the skin giving a cross-linked appearance without limits due to its centrifugal propagation; situation described in the present case [3, 4]. This dermatosis presents hyperkeratosis and a slight desquamation; to the touch, the surface is irregular which gives rise to a warty appearance by the anfractuous lifting of the cornea layer [3, 4, 5, 6]. It can also manifest as atrophic macules with bright features or with the change of surface similar to smoking paper [4]. Topography frequently involves the anterior thorax in the anterior neck, intermammary or sternal, and the epigastric region. In the posterior thorax can be found in the internal scapular line and paravertebral lines, as well as at the lumbar level. Other affected areas are usually the armpits and inguinal region; in rare cases, CRP develops elsewhere, such as the knee, elbow, hand and the antecubital and popliteal fossa [4, 5, 6]. In this case, the lesions were predominant in the anterior thorax and intermammary area.
The pathophysiology of CRP is unknown. Although several authors have linked this pathology to infection by Malassezia furfur which possibly generates an inflammatory response and abnormal keratinization [3, 6]. Other reports mention that histological study and immunohistochemical analysis show altered maturation and keratinization [7, 8]. The first case of partial tetrasomy of the long arm of the 15q chromosome associated with PRC was reported, in which the patient presented with dermal lesions that were clinically and histologically compatible with this disease [7]. Dietzia papillomatosis has been identified as a possible etiological agent [9].
Currently, there are many associated factors for which the disease is exacerbated and remitted [8]. Among them, we can find endocrine factors (Cushing's disease, menstrual irregularity, diabetes mellitus, thyroid dysfunction, pituitary disease, hirsutism, hypertrichosis, and obesity); bacterial (Staphylococcus sp., Propionibacterium acnes); genetic diseases, storage diseases (amyloidosis) and even vitamin A deficiency [1, 2]. In addition to photosensitivity (UV rays); alteration of keratinization; fungal infection (Pityrosporum oval); or finally by the altered response of the host to saprophytic fungi of the skin [2, 4]. The clinical picture is usually characterized by asymptomatic eruptions, but pruriginous eruptions have also been described. In rare cases, PRC can manifest as a wavy reticular erythema in Caucasian individuals [4]. The diagnosis is established by the correlation between the clinical findings and the histopathological findings. In the histopathological study, hyperkeratosis, parakeratosis, increased pigmentation of the basal layer and perivascular lymphohistiocytic infiltrate were observed [5]. In this case, a clinical diagnosis was made with a therapeutic test.
Electron microscopy and immunohistochemical studies show abnormal differentiation of keratinocytes, an increase of basal layer, cells in the transition layer, lamellar granules in the granular layer and melanocytes in the hyperkeratotic horn layer [1, 4]. Other diagnostic methods include dermoscopy, weight control, diet and exercise [3]. As well as the therapeutic diagnosis Clinically the PRC lesions may be confused with other dermatoses; the main dermatoses with PRC-like features are acanthosis nigricans, prurigo pigmentosum and pityriasis versicolor [8]. However, these can be ruled out through the dermatological examination or with the help of other diagnostic methods. Acanthosis nigricans is characterized by velvety plaques with brownish coloration in the armpits and lateral sides of the neck, with hyperkeratosis more marked than in CRP, and associated with states of hyperinsulinism or underlying neoplasms in certain occasions [2, 7]. Prurigo pigmentosum is an inflammatory dermatosis, which can manifest in two phases, an inflammatory phase with lesions of pruritic erythematous plaques and a resolution phase with reticular and pigmented lesions in the back, chest, neck or abdomen [9]. Histopathological features include hyperkeratosis, acanthosis, spongiosis, basal pigmentation, superficial and deep neutrophil perivascular infiltrate; subepidermal vesicles and necrotic keratinocytes can be observed [4, 9]. Pityriasis versicolor, which is characterized by finely desquamative macules in the upper trunk area, usually hypopigmented but occasionally hyperpigmented is distinguished from CRP by the absence of response to antifungal agents [2, 7, 9]. Other differential diagnoses are Darier's disease, macular amyloidosis, seborrheic dermatitis and parapsoriasis [2, 4, 6, 7, 9].
The treatment of PRC mainly focuses on the use of antibiotics such as tetracyclines, whose mechanism of action in the disease is not yet known, although it is suggested that it may have an anti-inflammatory effect and probably could be attributed to an inhibition of neutrophil migration, and subsequent release of reactive oxygen species [5, 6]. Minocycline is the tetracycline most used for its treatment, at doses of between 100 and 200 mg per day for 1 to 3 months [2]. However, Doxycycline has also been reported in a Spanish journal. The usual treatment is at a dose of 100 mg per day of doxycycline for one month, during which resolution of the lesions is obtained [5]. Other less conventional antibiotics for its treatment are amoxicillin, erythromycin, fusidic acid, clarithromycin and azithromycin, which although they have good results in some cases, have not been widely cited in the scientific literature [2, 10]. It is important to mention that they are not the only therapeutics for dermatosis since the studies report a wide range of treatments [1, 4]. Other therapeutics used are tacrolimus, topical retinoids (such as tretinoin and tazarotene) and systemic (isotretinoin and etretinate) derivatives of vitamin D (calcipotriol, tacalcitol), vitamin A derivatives, selenium sulfide, liquid nitrogen, progesterone, coal tar, dermabrasion, hydroquinone, phototherapy, 5- fluorouracil and thyroid extracts, each with a different response to treatment [1, 2, 4, 6, 8]. Valdeolivas-Casillas coincides with the treatment as a diagnostic method due to the evolution of the disease, a 100 mg Doxycycline capsule was given every 24 hours for three weeks and topical retinoid acid for application to the lesions at night.
References
-
Tirado Sánchez A, Ponce Olivera RM (2013) Tacrolimus in confluent and reticulated papillomatosis of Gougerot Carteaud. Int J Dermatol 52(4): 513-514.
-
Cabanillas GM, Monteagudo SB, León ME, De las Heras SC, Cacharrón CJ (2008) Papilomatosis reticulada y confluente de Gougerot-Carteaud. An Pediatr 68(6): 541-651.
-
Bernardes FF, Victoria QM, Coelho RF, Kawa KB, Costa NJ, et al. (2014) Confluent and reticulate papillomatosis of Gougerot-Carteaud and obesity: dermoscopic findings. An Bras Dermatol 89(3): 507- 509.
-
Zhong SM, Cheng T, Ping X, Wen YZ (2014) Confluent and reticulated papillomatosis manifested as vertically rippled and keratotic plaques. Postepy Derm Alergol 31(5): 335-337.
-
Valdeolivas-Casillas N, Trasobares-Marugán L, Medina-Expósito I, García Duarte A (2015) Papilomatosis reticulada y confluente de Gougerot – Carteaud: éxito terapéutico con doxiciclina. Piel (Barc) 30 (8): 533-542.
-
Tamraz H, Raffoul M, Kurban M, Kibbi AG, Abbas O (2013) Confluent and reticulated papillomatosis: clinical and histopathological study of 10 cases from Lebanon. JEADV 27(1): e119-e123.
-
Hanako K, Hideyuki U, Satoru A, Rinko O, Hiroshi S (2013) Confluent and Reticulated Papillomatosis Associated with 15q Tetrasomy Syndrome. Acta Derm Venereol 93(2): 202-203.
-
Neal CB, Lindasusan MM, Robert CM (2010) Gougerot-Carteaud Syndrome Treated with 13-cis- retinoic Acid. Clinical and Aesthetic Dermatology 3 (7): 56-57.
-
Ilkovitch D, Patton TJ (2013) Is prurigo pigmentosa and inflammatory versión of confluent and reticulated papillomatosis?. J Am Acad Dermatol 69 (4): e193-195.
-
Paci JF, Senán MR (2015) Mujer gestante con papilomatosis confluente y reticulada o síndrome de Gougerot y Carteaud. FMC 22(10): 596-597.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey