Hepatotoxicity Associated with Methylstenbolone and Stanozolol Abuse
Background & Objectives: Drug hepatotoxicity is a major cause of liver disease. Many drugs are well known to induce liver damage. Some toxic products, like anabolic androgenic steroids, that are pharmaceutical preparations since they contain pharmaceutically active substance, are available as nutritional supplements. Many patients are used to consume these like dietary stuff. Methods: We introduce a case series of two patients who developed hepatic damage after the consumption of anabolicandrogenic steroids, accompanied by a detailed bibliographic research on this topic. Results: We present two young men who developed significant liver damage, both with hyperbilirubinemia pattern after consumption of anabolic-androgenic steroids. This was associated with considerable morbidity, although both recovered without liver transplantation. The two anabolic-androgenic steroids were being marketed as dietary supplements. Conclusions: Although not well controlled substances in Brazil, anabolic-androgenic steroids are cause of severe hepatotoxicity. Whereas the National Sanitary Surveillance Agency acts in the regulation of such substances, some of these products are still marketed as dietary supplements, requiring a more rigorous surveillance by health professionals.
Gismondi R and Esberard EBC
karenarcevar@gmail.com these like dietary stuff.
androgenic steroids, accompanied by a detailed bibliographic research on this topic.
Keywords: Hepatoxicity; Anabolic steroids; Methylstenbolone; Stanozolol
Abbreviation: AAS: Anabolic-Androgenic Steroids; AP: Alkaline Phosphatase; GGT: Gamma-Glutamyltransferase; BT: Total Bilirrubin; DB: Direct Bilirubin; IB: Indirect Bilirrubin.
Introduction
| 2,17a-Dimethyl-17b-hydroxy-5a- | |||
|---|---|---|---|
| androst-1-en-3-one | ) which contains ultradrol, a | ||
| prohormone that, once consumed, is metabolized as a | |||
| steroid, and WINSTROL (stanozolol), considered a pure | |||
| anabolic-androgenic steroid [6]. |
Table 1: Viral serologic tests for hepatitis A, B and C, Epstein-Barr virus, cytomegalovirus as well as antinuclear antibody tite
Patient 1
A 21-year-old male construction worker was referred to Antônio Pedro University Hospital in January 2014 with a history of diffuse abdominal pain, jaundice, choluria, acholic feces and severe pruritus, as well as an 18-kilogram weight loss in the last three months. There was no history of altered mental status. There was a report of illicit drug use from age 14 to 16, and former smoker 10 packs • year (quit five years ago); without associated diseases. He admitted to using M-STANE one month prior to the start of his clinical condition, 2 capsules a day (dose recommended by the manufacturer) for a total of four weeks from October to November 2013. M-STANE was obtained from a “natural products” store, according to the patient's report. The patient denied any prior liver disease, excessive alcohol intake, medication use or travel; as well as family history of liver disease.
At admission the patient was hemodynamically stable, but had a marked conjunctival icterus. His liver was palpable 2 cm below the right costal border. However, there was no evidence of fluid overload or hepatic encephalopathy. Initial laboratory results are shown in Table 1. Viral serologic tests for hepatitis A, B and C, Epstein-Barr virus, cytomegalovirus as well as antinuclear antibody titers, antimitochondrial antibody, and anti- smooth muscle antibody were all negative. Urea and creatinine were within normal range. Chest radiograph and electrocardiogram were normal. Ultrasonography showed no evidence of biliary obstruction or chronic liver disease. Hepatic biopsy was performed, which histopathology study revealed cholestatic liver disease with marked cholestasis and porto-portal fibrosis, in addition to the presence of portal venous ectasia (Figures 1A &1B). We chose a conservative treatment with ursodeoxycholic acid 900mg/day. The patient had jaundice (4+/4+) when he was discharged, without signs of encephalopathy, with a prothrombin time of 100% and in a good physical status. Figures 2A & 2B show the course of hyperbilirubinemia as well as an isolated peak of alkaline phosphatase reaching a level of 701 U/L in the absence of a change in the level of gamma-glutamil transferase. Jaundice resolved over a period of 8 weeks. At this time ursodeoxycholic acid was finished because patient had no pruritus. At the last follow-up evaluation, 18 months after admission, the total bilirubin level was 0.34 mg/dL with alkaline phosphatase of 122U/L.
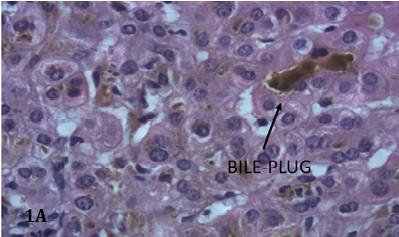
Figure 1A: Cholestatic liver disease (H.E. stain 20x), bile- plug dark arrow.
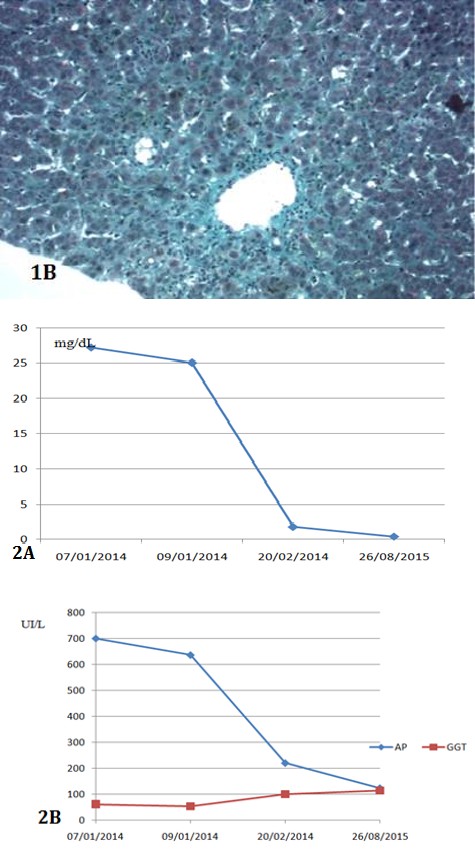
Figure 1B: Portal venous ectasia and fibrosis (Masson Trichrome stain; 10x).
Figure 2A: Total Bilirrubin.
Figure 2B: Alkaline phosphatase (AP) and gamma- glutamyltransferase (GGT).
| Case 1 | Case 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| AST (UI/L) | 38 | 83 (45) | ||||||
| ALT (UI/L) | 54 | 156 (50) | ||||||
| AP (UI/L) | 701 (136) | 200 (129) | ||||||
| GGT (UI/L) | 61 (85) | 42 (60) | ||||||
| TB (mg/dL) | 27.2 | 18.8 | ||||||
| DB (mg/dL) | 21.2 | 11.9 | ||||||
| IB (mg/dL) | 5.9 | 6.8 | ||||||
| Creatinine (mg/dL) | 0.79 | 0.98 | ||||||
| Albumin (mg/dL) | 2.3 | 4.2 | ||||||
| INR | 1.1 | 1.1 |
Patient 2
The second patient was a 28-year-old man, a bricklayer, who was referred to the hepatology department of Antônio Pedro University Hospital in January 2017 for diagnostic elucidation. He presented as symptoms: progressive jaundice, choluria, acholic feces and also reported a weight loss of 10 kilograms in the last three months and pruritus. He reported using Winstrol (stanozolol) for three weeks, in October 2016. He obtained the product from a professional at the gym. The patient denied any prior liver disease and had a history of eventual smoking and social drinking, although he denied any significant ingestion in the four weeks preceding the condition. On physical examination, he had a significant conjunctival icterus and hepatomegaly (18cm). He was alert and oriented. Laboratory values at hospital admission are shown in Table 1, viral serologies and autoantibodies were negative. Urea and creatinine were within normal range. Chest radiograph and electrocardiogram were normal. Ultrasonographic imaging showed a regular and homogeneous enlarged liver (reaching the right flank), with no evidence of intra or extra-hepatic dilatation. Computed tomography showed no perfusional or vascular alterations of the liver. The patient was treated conservatively with symptomatic treatment, as an outpatient. However, there was no significant improvement in bilirubin levels even with the AAS suspension since the onset of the clinical condition. A hepatic biopsy with subsequent histopathological study (Figures 3A & 3B) revealed cholestatic hepatitis with sinusoidal dilatation, Budd-Chiari simile, compatible with anabolic use, in addition to coexisting lobular and interface hepatitis suggestive of autoimmune hepatitis, possibly induced by the substance. In addition, there was the presence of portal fibrosis with short fibrous septa (F2). He was discharged with cholestyramine, hydroxyzine, ursodeoxycholic acid; the use of latter two being suspended by the patient himself two weeks later, due to diarrhea. The total bilirubin level reached a peak of 37.5 mg/dL (Figure 4). Later on, hyperbilirubinemia showed a gradual decrease. At the last clinic appointment, one month after initial evaluation, total serum bilirubin levels were 2.55 mg/dL and transaminases were within normal limits.
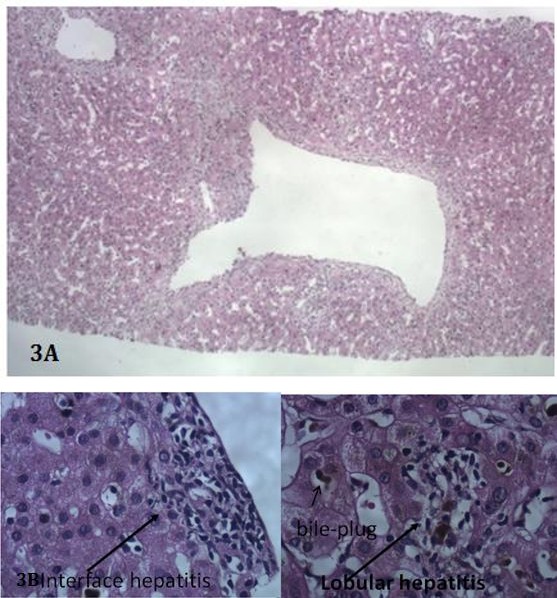
Figure 3A: Sinusoidal dilatation and central vein Budd – Chiari simile (H.E. Stain; 10x).
Figure 3B: Cholestatic hepatitis with coexistence of lobular and interface hepatitis (H.E.; 20X).
The two patients mentioned presented an important hepatic injury due to the use of AAS. Our first patient was consuming M-STANE (Methylstenbolone), which contains a prohormone called ultradrol that causes a high hormonal load, being like an AAS. Our second patient used Winstrol. It contains a synthetic steroid derived from testosterone called Stanozolol, which increases free testosterone in bloodstream [6]. Because of the serological and epidemiological exclusion of other causes and the compatibility in liver histopathology, the AAS consumed by these two patients was the most likely cause of hepatotoxicity. Initially, other causes of liver disease were excluded. Imaging studies revealed no evidence of biliary obstruction or vascular disease. The second patient had a history of alcohol consumption, but the biopsy was not compatible with an alcohol-induced injury. We should consider that alcohol may have increased susceptibility to hepatic injury induced by AAS
in our second patient [2]. The hepatic biopsy in both patients was consistent with AAS-induced hepatotoxicity, and in addition transaminases results showed spontaneous improvement after discontinuation of the substance. Our patients didn’t show evidence from another kind of tissue damage [7]. Currently, AASs are classified as controlled substances, and it’s illegal to possess, manufacture and distribute these products, except in case of medical prescription. However, these products are easily available on the internet and in “natural products” stores as dietary supplements. Misuse of AAS is a public health issue. Under the influence of the body builder culture and the body image valorization, we see the indiscriminate consumption of these substances. Studies show that anabolic steroid use among high school seniors increased in the last years in the United States [6, 8, 9, 10]. Also, men are more likely to use AAS compared to women [11]. Muscle dysmorphia is the new term used by Psychiatric researchers to describe people with an excessive fitness behavior, which can include toxic products consumption, with health risks [4, 12, 13]. AAS users practice unsafe injections and almost all report subjective side effects after the use of these drugs. Case reports linking AAS with others side effects have been reported including a bad lipid profile and atherogenesis [14], suppressed testicular function, cardiotoxicity, growth retardation, neuropsychiatric effects, nephrotoxicity including rare Wilms' tumors, acute kidney injury, acute renal failure as a complication of rhabdomyolisis [11, 12, 14, 15, 16].
Also a handful of animal studies provides evidence that the use of these pharmaceutical substance could lead to alterations of renal structure and function and a many cardiovascular complications such as focal fibrosis, inflammatory infiltrations of cardiac tissue [17, 18]. Hepatic complications include peliosishepatis, hepatic adenomas, hepatocellular carcinomas, and hepatotoxicity [17, 18]. These side effects abides a multi-factorial, partly irreversible effect that includes augmented tissue oxidative status [15, 19, 20]. In our patients, there was no evidence of cardiac or renal damage, but they developed cholestasis and hepatocellular injury [17, 18]. Cholestasis has been described as benign, but fatal cases have been reported. In most of cases, cholestasis induced by AAS is a result of a change in hepatocyte biliary secretion and generally is not associated with hepatocellular damage [21, 22, 23]. However, hepatitis may occur. Studies in rats showed that hepatotoxicity and increased levels of liver enzymes were drug-specific changes and that AAS had direct toxic effects on hepatocytes and that oxidative stress play a role, in impairment of the canalicular bile salt export pump [17, 18, 22, 23, 24, 25]. Structural changes induced by AAS include degenerative effects on mitochondria and lysosomes [26]. Animal studies exhibited that also cardiotoxicity and nefrotoxicity are associated with an increase of oxidative stress biomarkers [27]. In the present study, both patients demonstrated cholestasis that improved after AAS discontinuation [17, 18]. The differential diagnosis of hepatocellular injury with cholestasis includes viral hepatitis, drugs including alcohol, autoimmune disease and biliary duct obstruction. Family history of hepatic diseases was also analyzed. In our study, we investigated these diseases and there was no other explanation for the cholestasis and hepatic damage besides the use of AAS.
Conclusion
In conclusion, AAS consumption is a current tendency around the world, encouraged by body building culture. Although AAS-induced cholestasis is not very common, it is potentially fatal and associated with significant morbidity. Health professionals need to maintain a high level of vigilance over this scenario. Frequently, patients don’t tell about AAS consumption. It is important to regularly inquire patients about the consumption of AAS or dietary supplements. Also, it is imperative to educate our patients and health care professionals about the hepatotoxicity and other risks associated with the use of these products. Also, public health authorities must find strategies to control AAS market and consumption.
References
-
Butenandt A, Hanisch G (1935) Uber die umwandlung des dehydroandrosterons in _4 androstenol-(17)-on (3) (testosteron) un we gzurdarstellung des testosteronsauscholesterins (vorlaufmitteilung). Ber Dtsch Chem Ges 68: 1859-1862.
-
Shahidi NT (2001) A review of the chemistry, biological action, and clinical applications of anabolic- androgenic steroids. Clin Ther 23(9): 1355-1390.
-
Hengge UR, Baumann M, Maleba R, Brockmeyer NH, Goos M (1996) Oxymetholone promotes weight gain in patients with advanced human immunodeficiency virus (HIV-1) infection. Br J Nutr 75(1): 129-138.
-
Shahidi NT, Diamond LK (1961) Testosterone- induced remission in aplastic anemia of both acquired and congenital types. Further observations in 24 cases. N Engl J Med 264: 953-967.
-
Yesalis C (1993) Incidence of anabolic steroid use: a discussion of methodological issues. In: Anabolic steroids in sport and exercise. Champaign, IL: Human Kinetic Publishers, Inc.
-
Brown GA, Vukovich M, King DS (2006) Testosterone prohormone supplements. Med Sci Sports Exerc 38(8): 1451-1461.
-
Neri M, Bello S, Bonsignore A, Cantatore S, Riezzo I, et al. (2011) Anabolic androgenic steroids abuse and liver toxicity. Mini Rev Med Chem 11(5): 430-437.
-
Shipley A (2005) Steroids detected in dietary tablets. The Washington Post.
-
Parr MK, Geyer H, Hoffman B, Köhler K, Mareck U, et al. (2007) High amounts of 17-methylated anabolic- androgenic steroids in effervescent tablets on the dietary supplement market. Biomed Chromatogr 21(2): 164-168.
-
Striegel H, Simon P, Wurster C, Niess AM, Ulrich R (2006) The use of nutritional supplements among master athletes. Int J Sports Med 27(3): 236-241.
-
Anonymous (2000) Steroid (anabolic-androgenic). National Institute on Drug Abuse Info Facts, pp: 1-3.
-
Parkinson AB, Evans NA (2006) Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc 38(4): 644-651.
-
Pope HG Jr, Katz DL, Hudson JI (1993) Anorexia nervosa and “reverse anorexia” among 108 male bodybuilders. Compr Psychiatry 34(6): 406-409.
-
Hartgens F, Rietjens G, Keizer HA, Kuipers H, Wolffenbuttel BH (2004) Effects of androgenic- anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 38(3): 253-259.
-
Hartgens F, Kuipers H (2004) Effects of androgenic- anabolic steroids in athletes. Sports Med 34(8): 513- 554.
-
Modlinski R, Fields KB (2006) The effect of anabolic steroids on the gastrointestinal system, kidneys, and adrenal glands. Curr Sports Med Rep 5(2): 104-109.
-
Vasilakia F, Tsitsimpikou C, Tsarouhas K, Germanakis I, Tzardi M, et al. (2016) Toxicol Lett 241: 143-151.
-
Tsitsimpikou C, Vasilaki F, Tsarouhas K, Fragkiadaki P, Tzardi M, et al. (2016) Toxicol Lett 259: 21-27.
-
Walter E, Mockel J (1997) Images in clinical medicine. Peliosishepatis. N Engl J Med 337: 1603.
-
Tsukamoto N, Uchiyama T, Takeuchi T, Sato S, Naruse T, et al. (1993) Fatal outcome of a patient with severe aplastic anemia after treatment with metenolone acetate. Ann Hematol 67(1): 41-43.
-
Gurakar A, Caraceni P, FagiuoliS, Van Thiel DH (1994) Androgenic/anabolic steroid-induced intrahepatic cholestasis: a review with four additional case reports. J Okla State Med Assoc 87(9): 399-404.
-
Stimac D, Milic S, Dintinjana RD, Kovac D, Ristić S (2002) Androgenic/anabolic steroid-induced toxic hepatitis. J Clin Gastroenterol 35(4): 350-352.
-
Erlinger S (1997) Drug-induced cholestasis. J Hepatol 26(1):1-4.
-
Welder AA, Robertson JW, Melchert RB (1995) Toxic effects of anabolic androgenic steroids in primary rat hepatic cell cultures. J Pharmacol Toxicol Methods 33(4): 187-195.
-
Pey A, Saborido A, Blazquez AI, Delgado J, Megías A (2003) Effects of prolonged stanozolol treatment on antioxidant enzyme activities, oxidative stress markers, and heat shock protein HSP72 levels in rat liver. J Steroid Biochem Mol Biol 87(4-5): 269-277.
-
Perez LM, Milkiewicz P, Elias E, Coleman R, Sánchez Pozzi EJ, et al. (2006) Oxidative stress induces internalization of the bile salt export pump, Bsep, and bile salt secretory failure in isolated rat hepatocyte couplets: a role for protein kinase C and prevention by protein kinase A. Toxicol Sci 91(1): 150-158.
-
Gragera R, Saborido A, Molano F, Jiménez L, Muñiz E, et al. (1993) Ultrastructural changes induced by anabolic steroids in liver of trained rats. Histol Histopathol 8(3): 449-455.
-
Pecking A, Lejolly JM, Najean Y (1980) Liver toxicity of androgen therapy in aplastic anemia. Nouv Rev Fr Hematol 22(3): 257-265.
-
Friedl K (1990) Reappraisal of the health risks associated with the use of high doses of oral and injectable androgenic steroids. 102 (Vol), In: Li GC, Erinoff L, eds. Anabolic steroid abuse. Maryland: National Institute on Drug Abuse, pp: 142-177.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey