Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus
The study was undertaken to investigate the differences in the disease demographics and associated co-morbidities in working men and working women with Type 2 Diabetes Mellitus (T2DM). The study was carried out in 292 working men and working women from Bellary and Davangere districts of Karnataka state of India. The results indicate that a sex and gender difference does exist in treatment, management and prevalence of associated co-morbidities among working women and working men. Working women had higher prevalence of co-morbidities than men indicating a positive role of T2DM and its effect on dealing with multiple tasks of managing their regular activities, disease associated care and job related activities. The results re-emphasizes inclusion of sex and gender dimension in treatment modalities (pharmacological, dietary and quality of life) of T2DM in working men and working women separately
Introduction
Diabetes Mellitus (DM) is a community health issue which evidently stands out amongst the most serious illness affecting many individuals around the world. The prevalence of type 2 diabetes is growing worldwide; approximately 382 million people (8.3% of the global population) had the disease in 2013, and this number is estimated to exceed 592 million in less than 25 years [1, 2]. In recent years, male sex has been regarded as a risk factor for the development of type 2 diabetes [3].
There is increasing evidence that sex and gender differences are significantly important in pathophysiology, epidemiology, treatment and outcomes in many diseases, particularly for non-communicable diseases, specially type 2 diabetes mellitus (T2DM). Many organizations are now emphasizing inclusion of sex and gender dimension in biomedical research, to improve the scientific quality and societal relevance of the knowledge produced, technology, and innovation generated in treatment modalities [4, 5]. In the domain of endocrinology, pathophysiology, metabolism and clinical nutrition, the greatest body of evidence for important clinical implications of sexual dimorphisms comes from studies in the field of T2DM.
The relevant body of literature reports differences in diabetes management experiences between men and women, particularly in their beliefs, attitudes, fears and concerns about the disease. Women, more often than men, view diabetes as negatively affecting their lives. At diagnosis, more women reported fearing loss of health, diabetes-related morbidity, and early mortality compared to men [6]. Women worry more about both acute and chronic diabetes complications such as hypoglycaemia [7], cardiovascular and renal disease [6]. Women also report significantly more depressive symptoms [8], which can lower their participation in diabetes education and medication compliance [9]. Men are more concerned that diabetes will constrain their lifestyles [7] but believe it is controllable [10]. Men report being more concerned about how diabetes affects their provider role [11], whereas women worry more about how self-care will hinder their familial responsibilities [12], and they also tend to sacrifice their dietary regimen for their family’s food preferences [12].
Women exposed to high job demands and low job control (job strain) had a higher risk of complications in T2DM compared with those not exposed to this combination of work stressors. Women also exposed to low work social support had twofold higher risk of T2DM co-morbidities. High job demands, low job control, and low work social support were not individually associated with type 2 diabetes, supporting the theory that the combination of the three is toxic to health [13, 14]. Genetic background, lifestyle, environment and work related stress contribute to the pandemic increase of T2DM and its associated complications, presenting a challenge for healthcare systems [15]. Sex and gender differences are equally important in development, awareness, presentation, diagnosis and therapy, as well as prevention of the lifestyle-associated disease T2DM. Hence the study was taken up to study the disease demographic differences between working men and working women with T2DM
Materials and Methods
The study was carried out in 292 subjects who were chosen from outpatient / in patient departments in hospitals/clinics from Bellary and Davangere districts of Karnataka State. A purposive sampling technique was used to select type 2 diabetic patients based on inclusion Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
(Type 2 diabetes patients confirmed by WHO criteria, Age - 20 years and above, Engaged in work with a regular income, Duration of diabetes more than 6 months, Patients giving informed consent for the study) and exclusion criteria (Acute cases with compromised renal, hepatic, pulmonary and cardiac function, which requires the patient to be admitted for more than 2 weeks, Gestational diabetes mellitus, Inability to communicate due to physical or mental disability). Sample size was calculated using the formula: n= z2p (1 - p)/(d)2 Where n = Desired sample size, z = Confidence level (1.75) with 95% confidence interval, p = prevalence 60%, d = 0.05 acceptable error.
The diabetic patients recruited for this study is a set of T2DM working men and women who were willing to participate and may not represent all working T2DM men and women in the selected geographic location. However, this restriction does not threaten the internal validity of the analysis and findings may be generalizable among the Indian work force only (both men and women). The age groups selected for the present study are 20 – 40 years (Economically active age group), 41 – 60 years (Economically stabilized age group) and 61 – 80 years (Retired from service but still work for various reasons).
Study Tool
QOLID (Quality of Life Instrument for Indian Diabetes Patients) is a reliable, valid and sensitive tool for the assessment of diabetes specific quality of life in Indian subjects developed by Nagpal, et al. [16] with an overall Cronbach's Alpha value of 0.894 (subscale- 0.55 to 0.85) showing high internal consistency, good concordance (product moment correlation 0.724; p = 0.001; subscale correlation - 0.457 to 0.779) and DQL-CTQ. The QOLID questionnaire was selected for the present study as it was already subjected to expert panel review, item analysis, reliability analysis, concordant validity and discriminant validity by Nagpal, et al. [16] and is aptly suitable for studying Indian T2DM subjects with overall standardized questionnaire score and good responsiveness to metabolic control and co-morbidities establishing discriminant validity. The same questionnaire was used by the present study group to validate the data obtained on 384 T2DM subjects as a pilot work [17].
Self-administered questionnaires were provided and data was collected after willingness to participate was sought, and written consent was taken from all the Copyright© Kuna A, et al.
working men and women. Data entry was done using Epidata software. Double data entry was done to ensure accuracy and validate the process of data entry. Statistical analysis software SPSS for Windows 10.0 was used for the analysis of data. Demographic characters of the population was expressed as percentages.
Results and Discussion
Demographic Profile of Participants (N=292)
A study on Health related quality of life among working men and women with T2DM subjects was carried out on 292 subjects in Bellary & Davangere districts of Karnataka state. The demographic characteristics of participants of the study are presented in Table 1. Out of
| (n = 130) & 84.44% (n = 114)]. | Ramachandran, et al. [18] | ||
|---|---|---|---|
| have reported that the prevalence of diabetes, in patients | |||
| aged <40 years, has increased from 13.9% in 2000 to 18.6% | |||
| in 2006. | Studies have also observed the relationship |
| Number (%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Subject characteristics | ||||||||
| Men | Women | |||||||
| Age | ||||||||
| 20 - 40 years | 45 (28.7%) | 19 (14.07%) | ||||||
| 41 - 60 years | 103 (65.6%) | 103 (76.3%) | ||||||
| 61 - 80 years | 9 (5.7%) | 14 (10.4%) | ||||||
| > 81 years | - | - | ||||||
| Gender | ||||||||
| Male | 157 | - | ||||||
| Female | - | 135 | ||||||
| Education | ||||||||
| Primary | 26 (16.6%) | 22 (16.3%) | ||||||
| Secondary | 68 (43.31%) | 34 (25.2%) | ||||||
| College or higher | 63 (40.12%) | 80 (59.25%) | ||||||
| Occupation | ||||||||
| Sedentary | 30 (19.1%) | 47 (34.81%) | ||||||
| Moderate | 93 (59.23%) | 87 (64.44%) | ||||||
| Heavy | 34 (21.65%) | 2 (1.5%) | ||||||
| Marital status | ||||||||
| Married in partnership | 130 (82.8%) | 114 (84.44%) | ||||||
| Widowed | 11 (7%) | 12 (8.9%) | ||||||
| Divorced | 4 (2.54%) | 2 (1.5%) | ||||||
| Alone | 12 (7.64%) | 7 (5.2%) | ||||||
| Residence | ||||||||
| Own house | 61 (38.85%) | 53 (39.3%) | ||||||
| Rented house | 82 (52.22%) | 74 (54.8%) | ||||||
| Relatives | 14 (8.9%) | 9 (6.7%) | ||||||
| Monthly income | ||||||||
| < 10,000 | 37 (23.6%) | 17 (12.6%) | ||||||
| 11,000 - 19,000 | 51 (32.5%) | 54 (40%) | ||||||
| 20,000 - 29,000 | 61 (38.9%) | 52 (38.5%) | ||||||
| > 30,000 | 8 (5.09%) | 13 (9.62%) | ||||||
| Type of work |
Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
Copyright© Kuna A, et al.
| Field work | 29 (18.5%) | 11 (8.14%) |
|---|---|---|
| Desktop work | 41 (26.11%) | 81 (60%) |
| Both field & desktop work Labour work | 63 (40.12%) | 41 (30.4%) |
| 24 (15.3%) | 3 (2.22%) | |
| Hours of Work | ||
| 6 - 7 hours | 93 (59.23%) | 72 (53.33%) |
| 7 - 8 hours | 62 (39.5%) | 32 (23.7%) |
| 8 - 9 hours | 2 (1.3%) | 32 (23.7%) |
| 9 - 10 hours | - | - |
Table 3: Demographic profile of study respondents (N=292).
Results on level of education among the study respondents showed that 40.12% (n = 63) of working men completed college or higher education and 43.31% (n = 68) completed secondary education. Working women were better educated than working men with 59.25% (n = 80) of them who completed college or higher education and 25.2% (n = 34) completing secondary education. Kapur [20] reported that general education level seems very important and that diagnosis can be delayed by 3-7 years in the less and uneducated sections of the population. Actively working people are diagnosed almost a decade earlier, either because of better affordability of care or the need to remain fit to earn a livelihood for the family. Majority of respondents participated in the present study were all newly diagnosed with diabetes (between 6 months to 5 years).
Results on type of occupation showed that, 59.23% of men (n = 93) and 64.44% of women (n = 87) were involved in moderate work and most them were working for 6 to7 hours / day. Majority of working men (40.12%; n = 63) were involved in both field and desktop type of work compared to women who were involved in desktop type of work (60%; n = 81). Majority of the subjects i.e., 32.5% of working men (n=51) and 40% of working women (n=54) had monthly income between 11,000 to 19,000 income per month; 38.9% of men (n=61) and 38.5% of women (n=52) had income between 20,000 to 29,000 per month, which is reasonably good earning and could help the subjects with proper treatment for diabetes. Kapur [21] reported that many socio-economic factors and health care delivery related issues impact the outcome of diabetes and consequently the costs and vice- versa. Occupation carries the specific environmental exposures, and it may be of limited value in measuring socioeconomic status for women who have not been in the paid workforce for much of their adult lives. Socioeconomic status is associated with type 2 diabetes prevalence among women, but not consistently among Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
men. Diabetes prevalence is more strongly associated with psychological insulin resistance (PIR) than with education or occupational status [22]. It is well established fact that patient contributions are very important for better management of diabetes [23]. Lack of knowledge of diabetes care among patients can have adverse effects on their capabilities to control diabetes and in turn, on the quality of life. As most of the study respondents of present study were educated and working, they were all diagnosed with diabetes early and also have capability to control diabetes with their level of education and earning capacity.
Demographic Profile on Disease Related Parameters
Information on disease related parameters were collected from all the 292 subjects. Information on disease related parameters (duration of diabetes, family history, health status, treatment, diabetes related hospitalization, visit to physician, associated co-morbidities, following a special diet, visit to dietician & complying with given diet & regularity in blood tests/biochemical parameters) are given in Table 2.
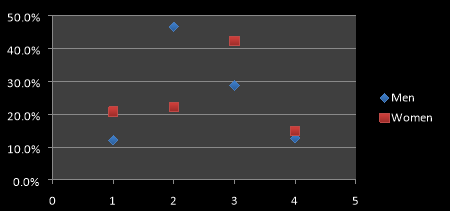
1= < 6 months, 2= 6 - 12 months, 3= 1 – 5 years and 4= > 5 years duration of diabetes Figure 1: Duration of diabetes mellitus among working men and women.
Copyright© Kuna A, et al.
| Number (%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Subject characteristics | ||||||||
| Men | Women | |||||||
| Health status | ||||||||
| Hypertension | 116 (73.9%) | 74 (54.8%) | ||||||
| High cholesterol | 41 (26.1%) | 37 (27.4%) | ||||||
| Poor eye vision | 24 (15.3%) | 28 (20.7%) | ||||||
| Brain stroke | - | - | ||||||
| Heart attack | 7 (4.45%) | 11 (8.2%) | ||||||
| Foot amputation | - | 2 (1.5%) | ||||||
| Kidney dialysis | - | 17 (12.6%) | ||||||
| Treatment | ||||||||
| Diet therapy alone | 13 (8.3%) | 4 (3%) | ||||||
| Oral pills only | 129 (82.2%) | 126 (93.3%) | ||||||
| Insulin only | - | - | ||||||
| Oral pills & insulin | - | - | ||||||
| Diet therapy & pills | 7 (4.5%) | 5 (3.7%) | ||||||
| No treatment | 8 (5.1%) | - | ||||||
| Diabetes related hospitalization in past year | 18 (11.5%) | 48 (35.6%) | ||||||
| Visit to physician | ||||||||
| Monthly twice | 15 (9.6%) | 10 (7.4%) | ||||||
| Once in a month | 91 (58%) | 66 (48.9%) | ||||||
| Once in 2 - 3 months | 22 (14%) | 33 (24.4%) | ||||||
| Once in 6 months | 12 (7.6%) | 20 (14.8%) | ||||||
| Rarely | 9 (5.7%) | 6 (4.4%) | ||||||
| Never | 8 (5.1%) | - | ||||||
| Following a special diet | 38 (24.2%) | 49 (36.3%) | ||||||
| Visit to Dietician & complying with given diet | 15 (9.55%) | 6 (4.44%) | ||||||
| Regularity in blood tests/ biochemical parameter | 143 (91.1%) | 128 (94.8%) |
Table 4: Demographic profile on disease related parameters among working men and women with T2DM.
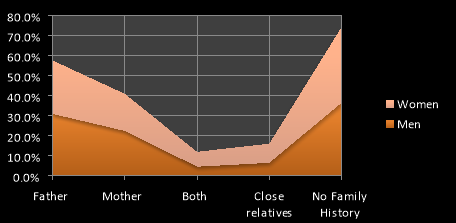
Responses about duration of diabetes (Fig.1) indicated that, 46.5% of working men (n=73) and 22.22% of working women (n=30) respondents reported duration of diabetes between 6 to12 months; 28.7% of men (n=45) and 42.22% of women (n=57) reported that the duration of diabetes was between 1 to 5 years. Majority of the respondents had a family history of diabetes (Fig.2) with either of the parent (father or mother) being diabetic. 36.3% of working men (n=57) and 37.8% of working women (n=51) subjects reported no family history of diabetes.
Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
Results on type of treatment among the study respondents showed that majority of them i.e., 82.2% of working men (n=129) and 93.3% of working women (n=126) were on oral pills. Results on visit to physician showed that, majority of the subjects i.e., 58% of working men (n=91) and 48.9% of working women (n=66) visit physician once in a month. 11.5% of working men (n=18) and 35.6% of working women (n=48) reported diabetes related hospitalization in the past one year indicating that diabetes related hospitalization were high in working women when compared to working men.
Results on T2DM associated problems among the subjects showed that 73.9% of working men (n = 116) and 54.8% of working women (n = 74) had hypertension; 26.1% of working men (n = 41) and 27.4% of working women (n = 37) had high cholesterol; 15.3% of working men (n = 24) and 20.7% of working women (n = 28) had vision related problems. None of the working men or women reported brain stroke. 4.45% of working men (n = 7) and 8.2% of working women (n = 11) had heart attack. 1.5% of women (n = 2) had foot amputation and 12.6% of women (n = 17) were undergoing kidney dialysis, while none of the working men reported any foot amputation or kidney dialysis indicating that women were more prone to nephropathy and neuropathy.
Liu, et al. [24] in their cross sectional hospital based survey in urban China on prevalence of chronic complications of type 2 diabetes mellitus in outpatients reported that, chronic complication is the outcome of type 2 diabetes and that at least one chronic complication was diagnosed in 52% of diabetic respondents, which increased with age. The present study findings are in correlation with the findings of Liu, et al. [24], where more than half of the respondents reported a chronic complication, which was an outcome of type 2 diabetes.
Copyright© Kuna A, et al.
Co-morbidity is defined as the occurrence of one or more chronic conditions in the same person with an index-disease, which occurs frequently among patients with diabetes. Currently, integrated diabetes care programs focus on diabetes related co-morbidities like cardiovascular diseases, retinopathy, nephropathy and neuropathy [25]. However, patients with diabetes do not only have diabetes related co-morbidity, but also have non diabetes related co-morbidity, such as depression, job related stress and other problems. With the on-going population aging in most of the societies, not only the number of patients with diabetes is expected to increase, but also the number of patients with diabetes and associated co-morbidities will increase. This implies that the current single disease management approach is not applicable to a large part of the patients with diabetes in the future [26].
Results on associated co-morbidities (Figure 3) showed that majority of the respondents had hypertension followed by hyper-lipidemia, cardiac disease, visual problems, nerve related problems, sexual dysfunction, peripheral vascular disease, renal problems, erectile dysfunction (working men) and vaginal problem (working women) indicating that co-morbidities are definitely a course of concern in the management of diabetes. Working women had higher prevalence of co- morbidities than men. Women may experience more or less of the same symptoms as men, however, there are several factors that are unique to the female body (physical make up, diabetes affects them differently due to hormones, menstruation and stress of job and household activities etc) which that could be responsible for higher prevalence of T2DM associated co-morbidities.
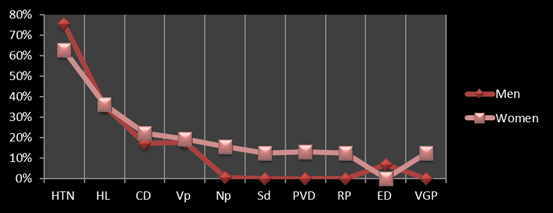
Note: HTN: Hypertension; HL: Hyper lipidemia; CD: Cardiac disease; Vp: Visual problems; Np: Nerve problems; Sd: Sexual dysfunction; PVD: Peripheral vascular disease; RP: Renal problems; ED: Erectile dysfunction and VGP: Vaginal problem.
Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
A study by Agarwal, et al. [27] reported that, among 11,157 subjects, retinopathy was diagnosed in 32.5%, nephropathy was present in 30.2%, peripheral neuropathy was present in 26.8%, coronary heart disease (CHD) was present in 25.8% and peripheral vascular disease (PVD) was present in 28% of the subjects. Microvascular complications from type 2 diabetes are common and include retinopathy and neuropathy as leading complications associated with increasing duration of T2DM [28, 29, 30].
Most adults with diabetes have at least 1 coexisting chronic condition [31], and approximately 40% have 3 or more [32]. As the number of co-morbidities increases, the risks of poor patient outcomes (eg, unnecessary hospitalizations, adverse drug events, mortality) and healthcare costs also increase [33]. Further, the types of co-morbidities have an impact on diabetes care [34]. Although previous studies have shown that the type and severity of co-morbidities matter, not just the number of conditions [35, 36], less attention has been paid to multiple chronic co-morbidities (MCCs) and how they impact diabetes care especially in working men and working women. Patients with MCCs constitute a majority of the diabetes population, and are known to require high levels of healthcare and to account for a significant proportion of healthcare costs [37]. However, it is unclear which MCC clusters in diabetes are most prevalent, or how MCC patterns vary by age and type of work in men and women separately. MCCs are an issue of growing significance not only because of their prevalence, but because they can complicate treatment and increase disease burden and costs [38, 39, 40].
Results on subjects following a special diet indicated that, 36.3% of working women (n = 49) respondents follow a special diet when compared to 24.2% of working men (n = 38). Results on subjects visit to dietician & complying with the given diet showed that, 9.55% of working men (n = 15) and 4.44% of working women (n = 6) visited dietician. Results of present study are similar to the findings of a study conducted on dietary practices by Badreldin, et al. [41] who reported 78.8% not complying with dietician visits in 222 type 2 diabetic Saudi population. Results on subjects regularity in blood tests/ biochemical parameters indicated that, 91.1% of working men (n = 143) and 94.8% of working women (n = 128) had regular blood tests.
Studies have analyzed the relationship between gender and quality of life among diabetes patients. Higher Copyright© Kuna A, et al.
quality of life was found among diabetic male patients than among diabetic female patients [42, 43] due to less physical activity, high obesity and poor socioeconomic condition of women than men [44]. It is evident from the results of the study that, working women had higher prevalence of T2DM associated co-morbidities compared to working men, indicating the multiple vulnerability of job stress, T2DM and management among working women.
Conclusion
Results of the study indicate that working men and women, in spite of having similar onset and duration of T2DM, the associated co-morbidities were higher among women than men which could be due to various factors (poor treatment adherence, job stress and balance between work and family responsibilities). This indicates that working women have to be more precariously treated than working men so that, they can have better treatment outcome and less complications associated with T2DM in the later part of their lives. Strategies have to be designed based on sex and gender differences to aggressively manage co-morbid conditions associated with diabetes, which may not only prevent diabetes- related complications, but also prevent irreversible deterioration of quality of life in diabetic patients, especially working women. Ethical committee approval: Required ethical committee approval was obtained to carry out the study and consent of all the subjects participated in the study was obtained prior to data collection from all the subjects. Conflicts of Interest: The authors report no conflicts of interest
References
-
Anna N, Hadrévi J, Olsson T, Franks PW, Nordström P (2016) Higher Prevalence of Type 2 Diabetes in Men Than in Women Is Associated With Differences in Visceral Fat Mass. The Journal of Clinical Endocrinology & Metabolism 101(10): 3740-3746.
-
Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, et al. (2014) Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Research and Clinical Practice (103): 137-149. Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207. _3._ Chen L, Magliano DJ, Zimmet PZ (2012) The worldwide epidemiology of type 2 diabetes mellitus- Present and future perspectives. Nature Review of Endocrinology (8): 228-236_._
-
Kautzky-Willer A, Harreiter J, Pacini G (2016) Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocrine Reviews 37(3): 278-316.
-
Schiebinger L, Klinge I (2015) Gendered innovation in health and medicine. Gender 1065: 643-654
-
Dietrich UC (1996) Factors influencing the attitudes held by women with type II diabetes: a qualitative study. Patient Education and Counseling 29(1): 13- 23.
-
Jonsson PM, Sterky G, Gafvels C, Ostman J (2000) Gender equity in health care: the case of Swedish diabetes care. Health Care for Women International 21(5): 413-431. _8._ Gucciardi E, Chi-Tyan S, DeMelo WM, Amaral L, Stewart DE (2008) Characteristics of men and women with diabetes: Observations during patients’ initial visit to a diabetes education centre. Canadian Family Physician 54(2): 219-227.
-
Park H, Hong Y, Lee H, Ha E, Sung Y (2004) Individuals with type 2 diabetes and depressive symptoms exhibited lower adherence with self-care. Journal of Clinical Epidemiology 57(9): 978-984.
-
Brown SA, Harrist RB, Villagomez ET, Segura M, Barton SA, et al. (2000) Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes. Diabetes Education 26(3): 425-438.
-
Hjelm KG, Bard K, Nyberg P, Apelqvist J (2005) Beliefs about health and diabetes in Men of difference ethnic origin. Journal of Advanced Nursing 50(1): 47-59.
-
Sarkadi A, Rosenqvist U (2002) Social network and role demands in Women’s type 2 diabetes: a model. Health Care for Women International 23(6-7): 600- 611.
-
Alexandros H, Chandola T, Daniel R, Witte, Brunner EJ (2009) Psychosocial Stress at Work Doubles the Risk of Type 2 Diabetes in Middle-Aged Women. Diabetes Care 32 (12): 2230-2235. Copyright© Kuna A, et al.
-
Karasek R, Theorell T (1990) Healthy Work: Stress, Productivity, and the Reconstruction of Working Life. New York, Basic Books.
-
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, et al. (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945): 766-781.
-
Nagpal J, Kumar A, Kakar S, Bhartiya A (2010) The Development of ‘Quality of Life Instrument for Indian Diabetes Patients (QOLID). A Validation and Reliability Study in Middle and Higher Income Groups. (58): 295-304. **17.** Daivashiromani V, Kuna A, Devi SS, Kumari PA, Sowmya M (2017) Effect of selected demographic characters on Health Related Quality of Life (HRQOL) in Type 2 diabetic subjects of Hyderabad & Rangareddy districts of Telangana State. The Journal of Research PJTSAU 45 (1 & 2): 104-112.
-
Ramachandran A, Mary S, Yamuna A, Murugesan N, Snehalatha C (2008) High prevalence of diabetes and cardiovascular risk factors associated with urbanization in India. Diabetes Care (31): 893-898.
-
Redekop WK, Koopmanschap MA, Stolk RP, Rutten GE, Wolffenbuttel BH , Niessen LW (2002) Health- related quality of life and treatment satisfaction in Dutch patients with type 2 diabetes. Diabetes Care (25): 458-463.
-
Kapur A (2001) Influence of socio-economic factors on diabetes care. Int J Diab Dev Countries 21: 77-85.
-
Kapur A (2007) Economic analysis of diabetes care. Indian Journal of Medical Research 125(3): 473-482.
-
Robbins JM, Viola Vaccarino, Zhang H, Kasl SV (2001) Socioeconomic Status and Type 2 Diabetes in African American and Non-Hispanic White Women and Men: Evidence from the Third National Health and Nutrition Examination Survey. American Journal of Public Health 91(1): 76-83.
-
Suppapitiporn S, Chindavijak B, Onsanit S (2005) “Effect of diabetes drug counseling by pharmacist, diabetic disease booklet and special medication containers on glycemic control of type 2 diabetes Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207. mellitus: a randomized controlled trial. J Med Assoc Thai 88(4): S134-S141.
-
Liu Z, Chaowei Fu, Weibing Wang, Biao Xu (2010) Research Prevalence of chronic complications of type 2 diabetes mellitus in outpatients - a cross-sectional hospital based survey in urban China. Health and Quality of Life Outcomes (8): 62.
-
Francesca V, Tillati S, Zanier L (2013) Prevalence and comorbidities of known diabetes. J Diabetes Investig 4(4): 355-359.
-
Yong D, Heidemann C, Gößwald A, Schmich P, Scheidt NC (2013) BMC Public Health 13: 166.
-
Agrawal RP, Ola V, Bishnoi P, Gothwal S, Sirohi P, et al. (2014) Prevalence of micro and macro vascular complications and their risk factors in type-2 diabetes mellitus. J Assoc Physicians India 62(6): 504-508.
-
Shaw JE, Sicree RA, Zimmet PZ (2010) Global estimation of the prevalence of diabetes for 2030. Diabetes Research and Clinical Practice 87(1): 4-14.
-
Vishwanath K, McGavin DD (2003) Diabetic retinopathy: clinical findings and management. Community Eye Health 16(46): 21-24.
-
Ahmedani MY, Hydrie MZ, Iqbal AG, Mirza A, Basit A, et al. (2005) Prevalence of microalbuminuria in type 2 diabetic patients in Karachi: Pakistan: a multicentre study. J Pak Med Assoc 55(9): 382-386.
-
Druss BG, Marcus SC, Olfson M, Tanielian T, Elinson L, et al. (2001) Comparing the national economic burden of five chronic conditions. Health Affairs (Millwood) (20): 233-241.
-
Wolf JL, Starfield B, Anderson G (2002) Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Archives of Internal Medicine (162): 2269-2276.
-
Struijs JN, Baan CA, Schellevis FG, Westert GP, van den Bos, et al. (2006) Comorbidity in patients with diabetes mellitus: impact on medical health care utilization. BMC Health Serv Res Journal 6: 84.
-
Kerr KCR, Stoeckle MY, Dove CJ, Weigt LA, Franciss CM, et al. (2007) Comprehensive DNA barcode coverage of North American birds. Molecular Ecology Notes 7: 535-543. Copyright© Kuna A, et al.
-
Davydow DS, Katon WJ, Lin EH, Ciechanowski P, Ludman E, et al. (2013) Depression and risk of hospitalizations for ambulatory care-sensitive conditions in patients with diabetes. Journal of General Internal Medicine 28(7): 921-929.
-
Krein SL, Heisler M, Piette JD, Makki F, Kerr EA (2005) The effect of chronic pain on diabetes patients’ self-management. Diabetes Care 28(1): 65- 70.
-
Lochner KA, Cox CS (2010) Prevalence of multiple chronic conditions among Medicare beneficiaries, United States. Preventing Chronic Disease 10: E61.
-
Boyd CM, Darer J, Boult C, Fried LP, Boult L, et al. (2005) Clinical practice guidelines and uality of care for older patients with multiple comorbid diseases: implications for pay for performance. The Journal of the American Medical Association 294(6): 716-724.
-
Tinetti ME, Fried TR, Boyd CM (2012) Designing health care for the most common chronic condition– multimorbidity. Journal of the American Medical Association 307(23): 2493-2494. Kuna A, et al. Differences in Disease Demographics and Associated Co- Morbidities in Working Men and Women with Type 2 Diabetes Mellitus. Med J Clin Trials Case Stud 2019, 3(1): 000207.
-
Anderson G (2010) Chronic Care: Making the Case for On-going Care. Princeton, NJ. Robert Wood Johnson Foundation.
-
Badreldin AM, Almajwal AM, Abdalla A, Saeed, Ibrahim A (2013) Dietary practices among patients with type 2 diabetes in Riyadh, Saudi Arabia. Journal of Food, Agriculture & Environment 11(2): 112.
-
Weiner S, Neugehauer EA (2013) Quality of life of diabetic patients with medical or surgical treatment. Nutricion Hospitalaria 28(2): 66-77.
-
Jacobson AM, Braffett BH, Cleary PA, Gubitosi Klug RA, Larkin ME (2013) DCCT/EDIC Research Group. The long-term effects of type 1 diabetes treatment and complications on health-related quality of life: A 23-year follow-up of the Diabetes Control and Complications/Epidemiology of Diabetes Interventions and Complications cohort. Diabetes Care (36): 3131-3138.
-
Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, et al. (2007) Primary prevention of cardiovascular diseases in people with diabetes mellitus: A scientific statement from the American Heart Association and the American Diabetes Association. Diabetes Care (30): 162-172. Copyright© Kuna A, et al.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey