Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis
Introduction: In adult surgical patients rapid recovery pathways after surgery have shown improvement in postoperative complications and length of hospital stay. Enhanced recovery after surgery is a concept which includes patient management protocols beginning from the preoperative period, continues in the intraoperative period and the postoperative period. This concept aims to improve postoperative outcome. In pediatric patients rapid recovery pathways are beginning to develop. This study was undertaken to analyse whether enhanced recovery after surgery improved postoperative outcome in terms of postoperative complications and length of hospital stay in children. Methods: After registration of this study in Prospero under the number [CRD42018103518], a systematic review and meta-analysis of randomised and non randomised trials was realised in April 2019 using electronic databases in children less than 18 years old where enhanced rapid recovery pathways after surgery were applied and compared to standard care. Statistic analysis was realised with RevMan 5.3 software. Results: 6 studies with 1620 children
Introduction
In adult surgical patients rapid recovery pathways after surgery have shown improvement in postoperative complications and length of hospital stay [1]. Enhanced recovery after surgery (ERAS) is a concept which includes patient management protocols beginning from the preoperative period, continues in the intraoperative period and the postoperative period. For instance preoperatively anticipating blood transfusion in potential hemorraghic interventions by improving preoperative hemoglobin levels by administrating iron or erythropoeitin, anticipating the nutritional patient status, reducing preoperative fasting times [2, 3, 4].
Intraoperatively, ERAS includes titration of fluid therapy to avoid hypovolemia or fluid overload by using means or goals to improve end organ perfusion and oxygen delivery; includes protective invasive or noninvasive lung ventilation if necessary; includes optimal analgesia using non opioid medications (for instance loco-regional analgesia), prevention of postoperative nausea and vomitting, using minimal invasive surgical technics such as laparoscopy, robotic surgery, interventional radiology [5, 6]. Postoperatively ERAS includes rapid oral intake, preferring enteral alimentation, prevention of postoperative nausea and vomiting, rapid mobilisation, physiotherapy, avoiding naso-gastric tubes, urinary bladder catheters or tubes if not necessary, early intravenous access withdrawal if not necessary [7, 8, 9, 10]. The objective of this study was to analyse whether ERAS improved postoperative outcome in pediatric surgical patients.
Methods
This study was registered under the number CRD42018103518 in PROSPERO, the international registration database for systematic reviews and meta- analysis. Since this was a systematic review and meta- analysis ethical approval from the local ethic committee was not necessary. Types of studies included were randomised and non randomised. Types of Participants: Children aged 0-18 years (inclusion criteria) were included and patients above 18 years were excluded (exclusion criteria). Types of Interventions: Surgical pediatric patients in whom rapid recovery pathways after surgery were applied compared to interventions where these protocols were not applied. Primary outcome was morbidity defined as postoperative complications. Secondary outcome was length of hospital stay. Primary outcome measures were defined by the number of patients with postoperative complications defined as organ failure or dysfunction and infections. Secondary outcome measures determined by the number of days spent in hospital after surgery. Titles and abstracts were electronically searched using these keywords ’ Enhanced recovery pathways after surgery in children OR Rapid recovery pathways after surgery in children OR Fast-tracking after surgery in children OR Enhanced recovery pathways after surgery in children and Outcome OR Rapid recovery pathways after surgery in children and outcome OR Fast-tracking after surgery in children and outcome OR ERAS in children OR Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
Enhanced recovery pathways after surgery in children in randomised and non randomised trial OR Rapid recovery pathways after surgery in children in randomised and non randomised trials’. Electronic search was realised in medline, embase, central, Google Scholar, Clinicaltrials.Gov, Abstarct Conference And Dare see flow chart in figure 1.
![Figure 1: Search flow chart according to the PRISMA statement [11].](/fulltextimages/3687/fig_1.png)
Copenhagen the Nordic Cochrane Centre, The Cochrane Collaboration 2014. Assessment of risk of bias in the included studies was realised using the tools proposed by the Cochrane Handbook for Systematic reviews of Interventions included with the software. Measures of treatment effect: Were dichotomous for morbidity (how many patients complicated) and was presented as odds ratio with 95%CI.
Results
6 retrospective studies with 1620 children were included (Table 1) in idiopathic scoliosis surgery (572 patients), in hypospadias (302 patients) and in appendicectomy (746 patients) [13, 14, 15, 16, 17, 18].
Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
| Sanders 2016 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | Wong 2018 [13] | Fletcher 2017 [14] | Gornitzky 2016 [15] | Cundy 2017 [17] | Skarda 2015 [18] | |||||||||||||||
| [16] | ||||||||||||||||||||
| Methods | Retrospective monocentric trial | Retrospective bicentric study | Retrospective monocentric trial | Retrospective monocentric trial | Retrospective/prospective case control trial | Retrospective monocentric trial | ||||||||||||||
| Participants | 302 children aged between 22 months [15- 38] and 36 months [21- 50] hypospadias surgery | 150 children aged between 10-18 years in adolescent idiopathic scoliosis | 138 children aged between 14.8±2.3 and 15±2.3 years in adolescent idiopathic scoliosis surgery | 284 children aged between 10 and 18 years in adolescent idiopathic scoliosis surgery | 166 children aged between 12.0±3.0 and 12.2±2.9 years in appendicitis surgery | 580 children aged between 9.7± 3.4 and 10.3±3.4 years in non non ruptured appendicitis surgery by laparoscopy or open surgery | ||||||||||||||
| Interventions | 176 children (control group) treated with the old service protocol were compared to 126 children (experimental group) treated with the new service protocol =enhanced recovery pathway protocol | 105 children from one center using an accelerated discharge pathway (experimental group) were compared to 45 children from a second center using a traditional discharge pathway (control group) | 80 children in the conventional pathway (control group) were compared to 58 children in the rapid recovery pathway | 194 children in the traditional pathway (control group) were compared to 90 children in the accelerated pathway (experimental group) | 83 children treated before the multidisciplinary criteria-led protocol CLD = preprotocol group or control group, were compared to 83 children treated according to the CLD protocol (experimental group) | 285 children treated prior to the new protocol= control group were compared to 295 children treated according to the new protocol | ||||||||||||||
| Definition of the interventions | old service protocol= patients remained in the hospital until removal of the urethral catheter, IV antibiotics, wound care by medical staff, 6 pediatric surgeons took care of the patients. The new service protocol= | The traditional discharge pathway was defined as the treatment on basis of the surgeon's preferences without a formal pathway i.e patient postoperative surveilliance realised in | Conventional pathway was characterised by pain management with intraoperative methadone and postoperative IV morphine or hydromorphone patient controlled | The Accelerated protocol was defined as where effort was coordinated by nursing, physiotherapy, | The multidisciplinary criteria-led discharge (CLD) protocol consisted of limiting postoperative antibiotics to 2 IV doses, avoidance of postoperative intravenous opioid analgesia, administration of | The new protocol was defined as a criteria- based postoperative treatment management where postoperative antibiotics were avoided and discharge faciliated with bedside |
Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
Copyright© Kumba C, et al.
enhanced recovery the surgical unit, transition to oral pain medications from PCA pump on postoperative analgesia (PCA); transition to oral medication (oxycodone pathway=patients discharged on day 2 or 3 postoperatively with the and acetaminophen ) as tolerated from day 3 urethral catheters, 3 day 3 after tolerating pediatric surgeons specialised in pediatric urology were in charge of the patients, parents oral intake, Foley removed on day 1-2, drain removed on day 2-3, mobilisation with to 4, diazepam for muscle spasme; bed rest on day 1 and physiotherapy and dietary progress on given instructions of wound care with saline instillation at home, oral physiotherapy once daily on day 1, transition to solid diet on day 2 after flatus and day 2; discharge criteria were oral antibiotics and patients oxycodone, acetaminophen, diazepam with bowel regimen (prevention of returned for catheter discharge home after removal a day after.
bowel movement on day 4-5. The accelerated pathway was defined as a highly narcotics side effects).
Rapid recovery pathway included
standardised pathway including patient preoperative gabapentin and acetaminophen; intraoperative IV postoperative surveillance on the surgical floor, transition to oral pain medications from PCA methadone and acetaminophen;
pump from postoperative day 1, postoperative hydromorphine PCA
Foley removed on postoperative day 1,
and diazepam, IV
acetaminophen, drains removed on postoperative day 1-2,
gabapentin and ketorolac on day 1 ; ambulation and full mobilisation with physiotherapy on from diet on day 1;
day 1 twice a day, transistion to solid diet accelerated physiotherapy on day Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
pain management intraoperative non- nurses to evaluate readiness to leave the steroidal anti- inflammatory drugs, early and orthopedic hospital oral intake and surgery to facilitate early ambulation ambulation and standardised pain management Copyright© Kumba C, et al.
on postoperative day 1 and discharge home on
0, 3 times a day bed to chair and walking on day 1; discharge home criteria included drain postoperative day 2-3 removal, same medication as in the conventional pathway Early morbidity [urine/wound swab culture) and/or documentations of urethral catheter dislodgement, wound bleeding, or wound Pain scores, LOS, gaping in the early postoperative period], Length of hospital stay, unplanned hospital stay, long-term complications Lenth of hospital stay, LOS and postoperative remaining postoperative pathway Outcomes complications (removal of PCA and urinary catheter) (=meatal stenosis, neo- urethra dehiscence, urethral fistula, urethral stricture or diverticulum) Early morbidity 28 [3 urinary tract infections, Number of patients with postoperative
2 catheter dislodgements, 24
9 (4 conservative wound, 1 operative wound, 3 revisons, 1
morbidity wound related (infection, bleeding, gaping)] /Long-term
NA (non applicable)
(organ dysfunction or medical) infection) Control group complications 61 [=Overall operative failure]
Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
LOS, complications, total
LOS, complications,
number of antibiotics dosages, postoperative opioid analgesia usage, postoperative anti-emetic requirement and direct in- LOS, costs of care, readmissions and postoperative pain management complications hospital costs
5 (inpatient readmission,
6 ( 1 re-presentation with
25 (return to nausea and vomiting, 1
observation readmission, post discharge emergency, the OR, postoperative re-admission for abdominal pain, 2 wound medical problems, site infections, 1 re- admission for intra- abdominal collection treated with IV antibiotics, abdominal abscess, reoperation, interventional radiology drainage, subcutaneous abscess, wound complications)
1 clostridium difficile ) clostridium difficile Copyright© Kumba C, et al.
colitis, postoperative CT imaging)
9 (inpatient readmission,
- Early morbidity 7 [0 urinary tract infections,
- Number of patients with postoperative
- 4 catheter dislodgements, 3 wound morbidity
- 8 (6 conservative wound, 1 operative related (infection, bleeding, gaping)]
- (organ dysfunction or wound, 1 medical)
- /Long-term complications 22
- [=Overall operative infection)
- Experimental group failure]
- CT imaging)
- Length of hospital stay in days median
- IQR or mean
- 10 [8-12]
- 4.2 [4.04-4.92]
- 5.0±0.8
- 5.0±1.26
- 27.7 [19.6] hours
- 40.1±27.5 hours
- ± SD Control group
- Length of hospital stay in days median
- IQR or mean
- 2 [2-2]
- 2.17 [2.11-2.23]
- 3.5±0.8
- 3.7±0.93
- 19.6 [6.3] hours
- 23.5 ± 20.8
- ± SD
- Experimental group
- Risk of Bias
- High
- High
- High
- High
- High
- High
Table 2: characteristics of the included studies
Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
Copyright© Kumba C, et al.
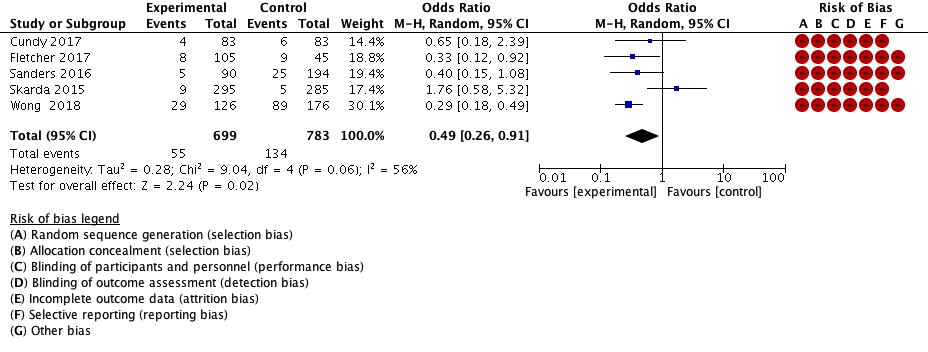
Postoperative Morbidity Defined as Organ Dysfunction or Infections
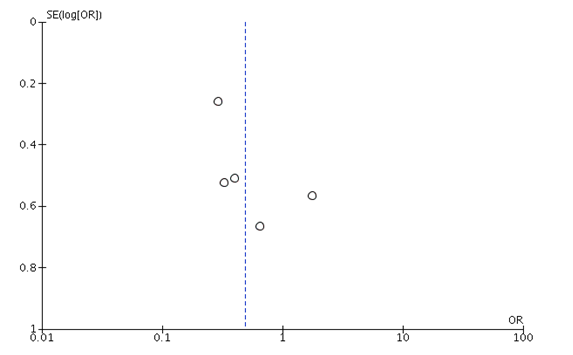
Five studies with 1482 patients analysed this outcome (Figures 2 & 3) [13, 14, 16, 17, 18]. Organ dysfunction or infections (see table 1 for details) were lower in the enhanced rapid recovery group, odds ratio (OR), 0.49 [0.26, 0.91], p=0.02. Heterogeneity was low, the risk of bias was high in all the studies (Figure 2). Publication bias was present see figure 3. The level of evidence (GRADE) was low (bias) to moderate (low heterogeneity and great number of patients) Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
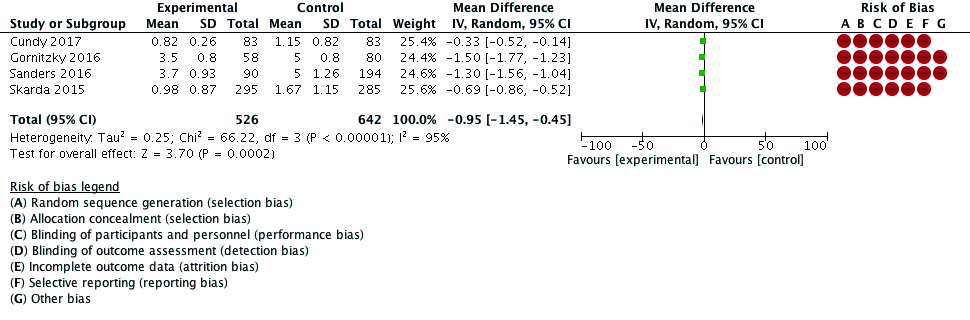
Length of Hospital Stay, LOS
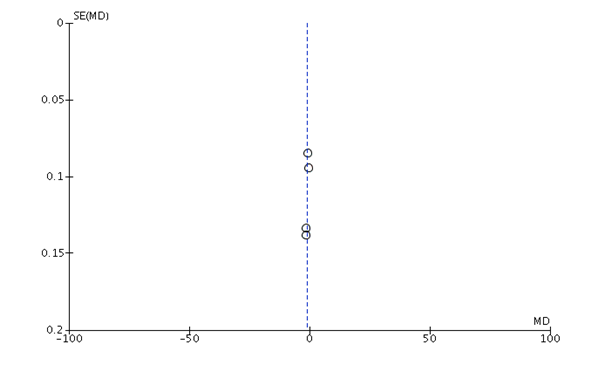
Four studies were included in this analysis with 1168 children (Figure 4) [15, 16, 17, 18]. LOS was lower in the enhanced recovery group, p=0.0002. Heterogeneity was high and all studies had bias. Publication bias was also present (Figure 5). The level of evidence (GRADE) was low.
Discussion
This meta-analysis showed that in hypospadias, idiopathic scoliosis and appendicectomy surgery, the number of patients with postoperative complications in terms of infections, reoperations and bleeding and length of hospital stay were reduced when enhanced recovery pathways were applied. In adult surgery these protocols begun to develop since 20 years and have proven improved postoperative morbidity and length of hospital stay in certain surgical populations [8, 9]. In children rapid recovery protocols after surgery are just beginning to develop [8, 9]. This systematic review and meta-analysis of retrospective trials has brought some evidence that Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
these protocols reduce LOS and complications. It has been shown previously that LOS was a predictive factor of postoperative complications in surgery like scoliosis [19]. Effort must be done to continue to develop this clinical practice to improve patient outcome in children. Future prospective randomised controlled trials will definitely confirm this evidence in the pediatric population. Limits: Only retrospective studies were included. The strength of this study was the great number of patients included.
Conclusion
This study demonstrated that when enhanced recovery protocols were applied in hypospadias, idiopathic scoliosis and appendicitis surgery the number of patients with postoperative complications and length of hospital stay were reduced.
References
-
Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds R, et al. (2005) Early goal directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial [ISRCTN38797445]. Critical Care 9(6): R687-R693.
-
Ross F, Latham G, Joffe D, Richards M, Geiduschek J, et al. (2017) Preoperative malnutrition is associated with increased mortality and adverse outcomes after paediatric cardiac surgery. Cardiol Young 27(9): 1716-1725.
-
Thomas M, Morrisson C, Newton R, Schindler E (2018) Consensus statement on clear fluids fasting for elective pediatirc general anesthesia. Pediatr Anesth 28(5): 411-414.
-
Mesbah A, Thomas M (2017) Preoperative fastening in children. BJA Education 17(10): 346-350.
-
Miller TE, Roche AM, Mythen M (2015) Fluid management and goal-directed therapy as an adjunct to Enhanced Recovery After Surgery (ERAS). Can J Anesth 62(2): 158-168.
-
Thiele RH, Raghunathan K, Brudney CS, Lobo DN, Martin D, et al. (2016) American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on perioperative fluid management within an enhanced recovery pathway for colorectal surgery. Perioperative Med 5: 24.
-
Muhly W, Sankar WN, Ryan K, Norton A, Maxwell LG, et al. (2016) Rapid Recovery Pathway After Spinal Fusion for Idiopathic Scoliosis. Pediatrics 137(4): e20151568.
-
Rove KO, Edney JC, Brockel MA (2018) Enhanced Recovery after surgery in children: Promising evidence-based multidisciplinary care. Pediatr Anesth 28(6): 482-492.
-
George JA, Koka R, Gan TJ, Jerin E, Boss EF, et al. (2018) Review of the enhanced recovery pathway for children: perioperative anesthetic considerations. Can J Anesth 65(5): 569-577.
-
Leeds IL, Boss EF, George JA, Strockbine V, Wick EC, et al. (2016) Preparing Enhanced Recovery After Surgery for implementation in pediatric populations. J Pediatr Surg 51(12): 2126-2129.
-
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses : The PRISMA Statement. PloS Med 6(7): e1000097.
-
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, et al. (2008) GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336(7650): 924-926.
-
Wong YS, Pang KK, Tam YH (2018) Hypospadias surgery in children: improved service model of enhanced recovery pathway and dedicated surgical team. Hong Kong Med J 24(3): 238-244.
-
Fletcher ND, Andras LM, Lazarus DE, Owen RJ, Geddes BJ, et al. (2017) Use of a Novel Pathway for Early Discharge Was Associated With a 48% Shorter Length of Stay After Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis. J Pediatr Orthop 37(2): 92-97.
-
Gornitzky AL, Flynn JM, Muhly WT, Sankar WN (2016) A Rapid Recovery Pathway for Adolescent Idiopathic Scoliosis That Improves Pain Control and Reduces Time to Inpatient Recovery After Posterior Spinal Fusion. Spine Deform 4(4): 288-295.
-
Sanders AE, Andras LM, Sousa T, Kissinger C, Cucchiaro G, et al. (2107) Accelerated Discharge Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211. Protocol for Posterior Spinal Fusion Patients With Adolescent Idiopathic Scoliosis Decreases Hospital Postoperative Charges 22%. Spine (Phila Pa 1976) 42(2): 92-97.
-
Cundy TP, Sierakowski K, Manna A, Cooper CM, Burgoyne LL, et al. (2017) Fast-track surgery for uncomplicated appendicitis in children: a matched case-control study. ANZ J Surg 87(4): 271-276.
-
Skarda DE, Schall K, Rollins M, Andrews S, Olson J, et al. (2015) A dynamic postoperative protocol provides efficient care for pediatric patients with non-ruptured appendicitis. J Pediatr Surg 50(1):149-152.
-
Kumba C (2019) A Retrospective Descriptive Cohort Study of Preoperative, Intraoperative and Postoperative Management of Children in Scoliosis Surgery. EC Anaesthesia 5(2): 20-29. Kumba C, et al. Rapid Recovery Pathways after Surgery in Children: A Systematic Review and Meta-Analysis. Med J Clin Trials Case Stud 2019, 3(2): 000211.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey