Adenoid Cystic Carcinoma of Breast: A Rare Entity
Adenoid cystic carcinoma (ACC) is a rare form of breast cancer (BC) with favourable prognosis. Clinically adenoid cystic carcinoma of breast (BACC) can be confused with phyllodes tumour as both may have an indolent course and present as a discreet mass without evidence of distant spread which might lead to dilemma in diagnosis of this rare form of BC. It is characterized by being ER-negative/PR-negative and rare axillary lymph node involvement. Due to its rarity, a treatment guideline of this form of breast cancer has not been established. Herein we report a case of ACC to create an awareness of this less known entity.
Introduction
Long standing tumours of the breast in females in their fourth and fifth decades are usually thought to be benign in nature, although malignancies are reported more and more in this age group [1]. One such is the phyllodes tumour, which commonly presents between 35- 55 years of age [1]. It usually presents as a moderately large tumour of slow growth that may be apparent for many months without significant complaints. While the median size is usually 4 cm, about 20% of these tumours may grow to more than 10 cm in size. With advancing age, the breast lumps tend to be malignant in nature, with varying degrees of invasiveness. Carcinoma of the breast typically presents in the 6th and 7th decade of life and a number of pathological variants have been reported, depending on their clinical course, malignant potential, cell types and metastatic potential [1]. Adenoid cystic carcinoma (ACC) is a rare group of malignant tumour which accounts for about 0.1% of all breast cancers [1]. Although the age of presentation of ACC is similar to that of other invasive BC, the hallmark of its presentation is slow growth and lesser risk of invasiveness and spread. So, when it presents in a premenopausal female, it mimics a benign lesion such a benign phyllodes tumor, which is common for that age group and also has an indolent course [1]. Due its rarity, biological behaviour, clinical course and treatment outcome, definite guidelines of management of breast ACC are not well established [2]. Accurate preoperative diagnosis of BACC allows correct surgical planning and optimum treatment. We present a case of BACC which had a clinical presentation mimicking a benign lesion and review the literature of this rare entity.
Case Report
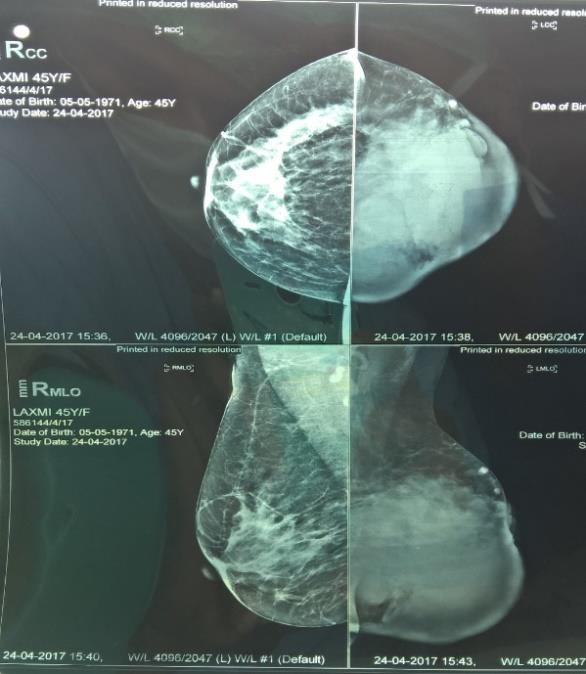
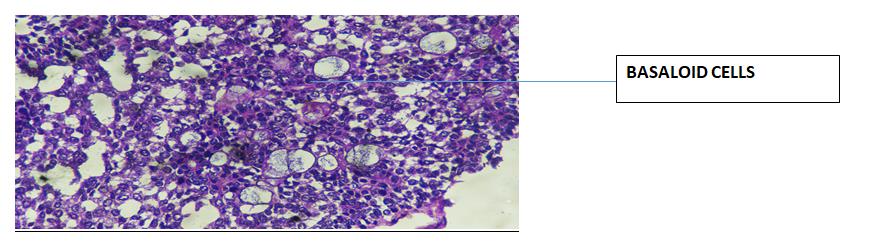
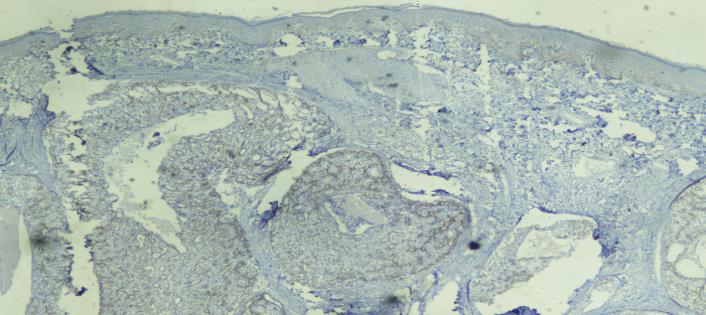
A premenopausal woman of 45 years presented with a lump in the left breast of 4 years’ duration and which had a rapid growth phase in the past 6 months. She denied any history of pain in the lump, discharge from the nipple, any surgery to the breast, any history of hormonal contraceptive pill intake or previous irradiation to the breast. No family history of similar disease was available. She was of average build and her BMI was 19 kg/m2. Examination of the left breast revealed a large lump of 15cm x10cm, which had nodular surface and firm consistency. Retraction of left nipple was seen (Figure 1). The ipsilateral axillary lymph nodes could not be palpated. Her systemic examination was unremarkable. A mammogram revealed retraction of the nipple with underlying well circumscribed, lobulated lesion with smooth margins involving the lower quadrants and retroareolar region along with thickening of overlying skin. No microcalcifications were observed (Figure 2). Clinical findings suggested a diagnosis of benign phyllodes tumor. A trucut biopsy was advised, which confirmed the diagnosis of ACC of breast. Due to its large size almost whole of the breast was involved and a simple mastectomy with axillary lymph node dissection was planned. The resected specimen showed a tumour of size 15 x 11 x 15 cm3 occupying almost the whole of the breast with predominant involvement of the lower quadrants. Microscopic examination revealed basaloid cells with hyperchromatic nuclei and a second type of cells with round vesicular nuclei lining the glandular lumen. Few tumour cells showed ductal carcinoma in situ (DCIS) component as well (Figure 3). The resected margins were free of tumor and there was no perineural invasion. The tumour cells were ER/PR/Her2neu negative but were positive for CD117 (Figure 4). She also received 34 Gy of adjuvant radiotherapy to the ipsilateral breast. The patient is on follow up for the last 6 months and is disease free both locally and systemically.

Farhanul H, et al. Adenoid Cystic Carcinoma of Breast: A Rare Entity. Med J Clin Trials Case Stud 2019, 3(5): 000238.
Discussion
ACC of the breast was first described by Geschikter1 and accounts for 0.1% of all breast cancers. It is more Copyright© Farhanul H, et al.
frequent in postmenopausal females in the sixth decade of life [2, 3]. The most common presentation of this entity is a palpable mass and a number of studies have reported an average tumor size of 3.0 cm [4, 5, 6, 7]. The size of the lump in the present case was 15 cm in its greatest dimension, presented in the premenopausal period and had a very much indolent course. Axillary lymph node involvement in ACC of the breast is uncommon [2]. According to Sumpio, et al. [3] axillary lymph node involvement occurs in 6.6% of the breast ACCs. The axillary lymph node were both clinically and histologically negative for malignancy in the present case.
Mammography features of breast ACC include a smooth or lobulated pattern that may or may not have sharp margins and microcalcifications are usually absent [8]. Mammographic features in our patient revealed retraction of the nipple with a underlying well circumscribed, lobulated mass with smooth margins involving mainly the lower quadrant and retroareolar region with no microcalcification which in concordance with previous studies [8], and which gave a benign look to the mass.
Distant metastasis is rare with breast ACC. Sumpio, et al. [3] reported distant metastasis in 6.6% in their series and the commonest site of metastasis was lung. Leeming, et al. [9] also reported metastases in 7.1% of the patients they had reviewed. A complete workup in our patient was negative for distant metastasis. ACC of the breast is characteristically negative for ER/PR/Her2 Neu and positive for CD117 [10], as was also found in the present case. Interestingly phyllodes tumours are also positive for CD117 along with mdm2 and cdk4, which are more specific markers while breast sarcomas tend to show positivity for CD31 [10].
Uniform treatment guidelines of ACC of the breast are lacking. There is no consensus whether it should be treated with a modified radical mastectomy or wide local excision. In a study by Aprino, et al. [2], 78.6% patients developed local recurrence after lumpectomy and 21.4% after mastectomy. In another study [10] it was found that the five-year postoperative rates of local recurrence were better following mastectomy. Wang et al argue that the rate of local recurrence after surgery alone is very high, but improves when it is combined with adjuvant radiotherapy (RT) [11]. In another study by Sun JY, et al. [12], both the disease specific survival and the overall survival were better in patients who received adjuvant RT compared to patients who received lumpectomy alone or Farhanul H, et al. Adenoid Cystic Carcinoma of Breast: A Rare Entity. Med J Clin Trials Case Stud 2019, 3(5): 000238.
mastectomy alone. Our patient underwent a mastectomy followed by adjuvant RT as the tumour was present for more than 4 years, was more than 10 cm in size and was involving the whole of the breast.
The incidence of axillary lymph node involvement in breast ACC is very less and routine management of axilla is controversial. The risk of axillary lymph node involvement increases with larger tumours, concomitant invasive carcinoma or “solid basaloid” variant [13]. According to Kumar, et al. [14] axillary lymph node dissection is indicated only in the presence of risk factors like clinically palpable lymph nodes, concomitant invasive carcinoma or “solid basaloid” variant. Martelotto, et al. have recommended a sentinel lymph node biopsy in tumours larger than 3.0 cm [15]. In our patient axillary lymph node dissection was done due to the large size of the tumour and long standing disease. Although all the lymph nodes were negative for malignancy, in retrospect we believe the axillary was justified due to the presence of concomitant ductal carcinoma components in situ in histological examination.
Conclusion
ACC is a very rare form of primary BC and has a favourable prognosis despite being negative for hormone receptors. Although, it is a disease of postmenopausal females in the sixth decade of life, but very exceptionally it can occur in premenopausal, young females. A high index of clinical suspicion is warranted to prevent delay in diagnosis. The concomitant ductal carcinoma component is a cause of concern as its presence is with timely diagnosis and treatment BACC has an excellent prognosis. As the best management of BACC is still controversial, the treatment has to be individualised.
References
-
Geschickter CF (1945) Diseases of the Breast: Diagnosis, Pathology, and Treatment Philadelphia, PA: J.B. Lippincott.
-
Grazia Arpino, Gary MC, Syed M, Valerie JB, Richard ME (2002) Adenoid Cystic Carcinoma of the Breast Molecular Markers, Treatment, and Clinical Outcome. Cancer 94(8): 2119-2127.
-
Bauer ES, Timothy A, Merino MJ, Sullivan PD (1987) Adenoid Cystic Carcinoma of the Breast Data from the Connecticut Tumor Registry and a Review of the Literature. Ann Surg 205(3): 295-301. Copyright© Farhanul H, et al.
-
McClenathan JH, de la Roza G (2002) Adenoid cystic breast cancer. Am J Surg 183(6): 646-649.
-
Millar BA, Kerba M, Youngson B, Lockwood GA, Liu FF (2004) The potential role of breast conservation surgery and adjuvant breast radiation for adenoid cystic carcinoma of the breast. Breast Cancer Res Treat 87(3): 225-232.
-
Rosen PP (1989) Adenoid cystic carcinoma of the breast. A morphologically heterogeneous neoplasm. Pathol Annu 24(Pt 2): 237-254.
-
Peters GN, Wolff M (1983) Adenoid cystic carcinoma of breast. Report of 11 new cases: review of literature and discussion of biological behaviour. Cancer 52(4): 680-686.
-
Santamaría G, Velasco M, Zanón G, Farrús B, Molina R, et al. (1998) Adenoid cystic carcinoma of the breast: mammographic appearance and pathologic correlation. AJR 171(6): 1679-1683.
-
Leeming R, Jenkins M, Mendelson G (1992) Adenoid cystic carcinoma of the breast. Arch Surg 127(2): 233- 235.
-
Khanfir K, Kallel A, Villette S, Belkacémi Y, Vautravers C, et al. (2012) Management of adenoid cystic Farhanul H, et al. Adenoid Cystic Carcinoma of Breast: A Rare Entity. Med J Clin Trials Case Stud 2019, 3(5): 000238. carcinoma of the breast: a Rare Cancer Network study. Int J Radiat Oncol Biol Phys 82(5): 2118- 2124.
-
Wang S, Ji X, Wei Y, Yu Z, Li N (2012) Adenoid cystic carcinoma of the breast: Review of the literature and report of two cases. Oncol Lett 4(4): 701-704.
-
Jia-Yuan Sun, San-Gang Wu, Shan-Yu Chen, Feng-Yan Li, Huan-Xin Lin, et al. (2017) Adjuvant radiation therapy and survival for adenoid cystic carcinoma of the breast. Breast 31: 214-218.
-
Thompson K, Grabowski J, Saltzstein SL, Sadler GR, Blair S (2011) Adenoid cystic breast carcinoma: is axillary staging necessary in all cases? Results from the California Cancer Registry. Breast J 17(5): 485- 489.
-
Kumar BR, Padmanabhan N, Bose G, Paneer V (2015) A case report of adenoid cystic carcinoma of breast - so close yet so far from triple negative breast cancer. Journal Clin Diagnos Res 9(7): 1-3.
-
Martelotto LG, De Filippo MR, Ng CK, Natrajan R, Fuhrmann L, et al. (2015) Genomic landscape of adenoid cystic carcinoma of the breast. J Pathol 237(2): 179-189. Copyright© Farhanul H, et al.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey