An Audit of CSF Examination Turnaround Time for all Indoor Patients in the Hospital for Past Six Months at Tertiary Care Hospital
Cerebrospinal fluid is an emergency test which requires stringent monitoring from sample collection, transport, acceptance and release of report. These all must be in time framework .Our audit was regarding the turn around time of cerebrospinal fluid and found that TAT for CSF testing was actually falsely high due post analytical errors. Our study provides glaring evidence that can be used as a basis for making relevant changes in establishing laboratory TAT.
Introduction
Laboratory based clinical audit is an important process in obtaining feedback for continual improvement. It involves measuring laboratory performance using selected quality indicators and defined benchmarks. Audits in the laboratory are used to determine the root causes of non- conformities and assess the effectiveness of changes made. Timeliness of laboratory results as a quality indicator assess the effectiveness and efficiency of the total testing process and is expressed as turnaround time (TAT) for laboratory tests. The impact of TAT on hospital stay is well documented. An improvement of TAT may require increased manpower and use of sophisticated equipment with greater through output but is often not a practical solution especially in low income countries. Redesigning the workflow to utilize time efficiently is often necessary for addressing challenges of high TAT. Understanding the root causes of high TAT using evidence based methods is therefore imperative for planning improvements as a result the regulatory and accreditation bodies regularly advise clinical laboratories to target TAT in their continual improvement process [1, 2].
Test like Cerebrospinal fluid examination (CSF) is an emergency test that requires stringent monitoring as untimely laboratory results affect patient care. In addition to this the stability of CSF sample further adds to the need for rapid analysis. Sample transport times, type of patient i.e inpatient versus outpatient are some of the factors that influence TAT [3].
CSF examination as such is a unique challenge to laboratory as it encompasses CSF glucose, protein, chloride, microbiology and microscopic examination to diagnose suspected neurological infection. The complete set of CSF results is required for meaningful interpretation and this may affect TAT. CSF samples are often shared between different sections of the laboratory such as microbiology and clinical chemistry leading to increased TAT [4].
Aims & Objectives: The aim of the study was to examine the three phases of CSF testing – preanalytical, analytical and post analytical phase and if required change the current practice to improve TAT and customer satisfaction. The objective of the audit was to determine the percentage of CSF samples reported out of range with an agreed time interval from sample collection to final report printing.
Standards: Criteria range: Complete avoidance of delayed reporting of CSF should be an ideal target.
Laboratory procedure for test requesting, analysis and reporting:
- The laboratory has a procedure that lists all critical test results that pertains to tests that require prompt clinical action.
- The laboratory has all written policies and procedures for CSF examination including preanalytical, analytical, post analytical, report authorization, release of report, laboratory software user authorization, and dispatch of reports as well as handling of non conformities.
Material and Method
The retrospective study was conducted on the CSF examination requests during six month period from January 1, 2017 till June, 30, 2017 for all inpatients at Brig T K Narayan, Department of Pathology & Transfusion Medicine, Santokba Durlabhji Memorial Hospital and Research Center, a tertiary care hospital in Jaipur, India. The study was approved by the Ethics Committee of the hospital. A waiver of consent was obtained as the study was retrospective and no patient results were used. Patient confidentiality was maintained at all times [5].
The study was carried using information derived from the laboratory LIS database. The time taken for complete analysis from sample acceptance to analytical phase, to final authorization and report printing at the clinical areas was retrieved from the laboratory LIS (e-laboratory software). The LIS system captures information at relevant time points determined by the operational workflow of the laboratory. The information extracted from the LIS was used to compute the TAT to reflect the four stages, described in Table 1. The in house delayed samples for CSF examination were further examined to know the reasons of poor TAT [6]. Missing entries or errors occurred whenever the laboratory staff at any operational point failed to register the appropriate sample details on the LIS and such cases were excluded from the study. The total TAT refers to the time, from collection of the sample to the time of delivery of reports at the end user. The within-laboratory TAT refers to the time, from receipt of sample at laboratory reception to authorization of final result by doctor. The TATs of CSF chemistry (a STAT test) and plasma glucose (a routine test) were compared to determine if the measures put in place to fast track STAT samples in our laboratory were successful. Routine plasma glucose was used in this study since glucose is also a component of CSF panel. The agreed TAT for routine glucose in our laboratory was 120 minutes [7]. Data from LIS was exported to Microscoft Excel® 2013, version 15.0. Thereafter, analysis was done using online free statistical calculator (http://www.xuru. org/st/DS) Assessment of normality of data was done using the Shapiro-Wilk test at P < 0.05 significance level. The relationship between high TAT CSF samples and the Plasma glucose was tested for significance using Fisher’s exact test. A P value < 0.05 was considered significant.
| Operational period | Starting point | End point | Time defined as per SOP (180 min ) | Redefined Time after audit (120 min) |
|---|---|---|---|---|
| Sample transport ( Collection- Acceptance) | Time on LIS | Time of sample received in laboratory | 30 Minutes | 5 minutes |
| Sample processing ( Acceptance-Complete) | Receiving time | Test completion time | 90 Minutes | 90 minutes |
| Sample authentication ( Complete- Authenticate) | Test completion time | Report authentication time | 30 Minutes | 20 minutes |
| Report printing ( Authentication- Printing) | Report authentication time | Printed report received by end user | 20 Minutes | 5 minutes |
Table 1: The various operational periods in CSF testing (Total 180 minutes).
Results
A total of 1011 CSF samples were received for examination during the study period (6 months). 417 (41.25%) were in patients and 592 (58.75%) were from outside the hospital. In 247 (59.23%) of the in patients the TAT exceeded 2 hour limit. These delayed CSF samples were further analyzed. Plasma glucose was also compared with delayed CSF samples as it is the most frequent test ordered with CSF. As seen in table 2 the majority of delay was due to lag in the printing of the reports in the clinical areas after authentication. The number of CSF samples received in study period from Jan 1, 2017 till Jun 30, 2017 was 1011. 417 (41.25%) were in patients and 592 (58.75%) were from outside the hospital. The accepted TAT for reporting CSF samples is 2 hours.
In 247 (59.23%) of the in house patients the TAT exceeded 2 hour limit. Three patients having delayed CSF TAT were excluded from the study due to lack of data relating to completion and authentication times. Of the 244
delayed CSF TAT samples, we performed Shapiro Wilk test to ascertain the normality of data. (Table 2) The test showed normal distribution of data. The median time for delayed CSF samples were 1 minutes for Collection – Acceptance (Normal time -30 minutes), 74.5 minutes for Acceptance- Completion (Normal time – 90 minutes), 12.5 minutes for Completion – authentication (Normal time – 30 minutes) and 55.5 minutes for Authentication –Printing (Normal time – 20 minutes) [8, 9].
| Collection – Acceptance( 30 min) | Acceptance – Completion ( 90 min) | Completion – Authentication ( 30 min) | Authentication – Printing ( 20 min) | |
|---|---|---|---|---|
| Sample size | 244 | 244 | 244 | 244 |
| Mean | 13.07786 | 83.88114 | 29.43.327 | 102.29918 |
| Median | 1 | 74.5 | 12.5 | 55.5 |
| Standard deviation | 25.42668 | 65.662485 | 44.03533 | 154.26695 |
| 90% Completion time | 10.39 | 76.94 | 24.77 | 85.99 |
Table 2: Shapiro-Wilk test at P<0.05, the distribution of samples CSF were normal.
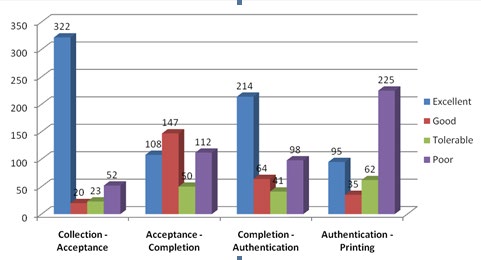
The comparison of four steps of CSF examination with the prescribed Upper limit time as per laboratory policy showed a clear cut delay in the final step of examination ie Authentication – Printing of report. The results were statistically significant with p value <0.00001 (Table 3, Figure 1). The total laboratory TAT for both CSF (177.5 minutes) and Plasma Glucose (Table 4). (82.5 minutes) were acceptable. The median within laboratory TAT for CSF was 107 minutes minutes and 110.95 minutes. Of the 244 samples with delayed CSF non complaint with our Standard operating procedure, in 87 (36.44%) the actual within Laboratory TAT was increased. In the remaining 157 (63.56%) samples with in laboratory TAT was within acceptable range although total TAT was increased.
| Median of delayed CSF samples (Minutes ) | Median of Glucose samples (Minutes) | |
|---|---|---|
| Collection – Acceptance | 1 | 4 |
| Acceptance – Completion | 74.5 | 40 |
| Completion – Authentication | 12.5 | 1 |
| Authentication – Printing | 55.5 | 4 |
Table 3: Comparison with defined TAT as in department policy.
Discussion
The laboratory performs routine CSF protein, glucose and chloride analysis along with Grams stain and Acid Fast Bacilli staining as a panel. Other biochemical tests such as lactate or adenosine deaminase were performed on special request. The CSF samples were collected in minimum three vials: one fluoride tube (glucose), one plain tube (protein and chloride) and another plain tube (microbiology).
Samples go through the processes of registration and labeling followed by immediate transport to the laboratory for analysis. The result of analysis is available for the clinicians after review and authorization through the laboratory information system (LIS). The laboratory aims to fast-track all STAT samples (including CSF samples) and to release the results within two hours. Emergency samples are marked as “STAT” and given preference through all the phases of the testing cycle. The analysis of 417 delayed samples revealed that laboratory was responsible for 87(36.44%) of samples because in 157 (63.56%) samples there was delayed printing of the report at the user end and the reports were informed to clinicians without taking print outs of the report.
The laboratory often describes TAT starting from the time of receiving the sample to the time of dispatch of the results. There are however certain steps in total testing cycle that are beyond control of laboratory like- time difference between ordering of test and sample collection. Likewise the time between dispatch of the test result and physician analyzing the result for taking clinical decisions.
Our audit showed that the median total laboratory TAT in our laboratory for CSF chemistry was 177.5 minutes which exceeded our target (170 minutes) marginally. The analysis of 244 samples that were delayed was done from laboratory values using non parametric values like median and tail size (skewness) taken into consideration as the distribution was non Gaussian.
The inter laboratory TAT for CSF chemistry for our laboratory was 107 minutes. The breakdown of total TAT into 4 stages of testing cycle showed that it was the last step ( authentication- printing) that was main culprit fort high TAT- 55.5minutes (target-20 minutes).
CSF been an emergency test and its report at all times is informed to clinician as per our laboratory policy. We gathered information from critical value communication data log and found that 227 of the delayed reports were actually informed to treating doctors telephonically within the time frame although the printing was delayed due to printing problem in the software. Our data included 24x7 samples from indoor patients and few clinical areas were not closely monitored by IT personnel for adequacy of papers in printers and whether printers are ready or not at the time of giving print command resulting in back drop of command by software, ultimately hampering the TAT. Post audit we redefined our CSF testing TAT to 120 minutes from 170 minutes (Table 1).
The effective communication in 227 delayed samples resulted in timely clinical decision without any effect on patient care. Of the 17 delayed reports – 2 were due to repeat sampling, and in further 15 cases there was printer failure. The printer failure was in newly constructed building where dedicated IT personnel were lacking.
We also found that our efforts have fast tracked the preanalytical handling of emergency samples like CSF and were effective for step 1 as evidenced by shorter median duration – 1 minute of this period of CSF examination as compared to routine glucose estimation (4 minutes).
The time taken for second phase (acceptance – completion) was satisfactory as per our standard operating procedure. This phase in comparison to routine blood glucose was extended (74.5 minutes in CSF to 40 minutes in glucose testing) as it involved preparation of Neubauer chamber, geimsa stain, gram’s stain and AFB staining for complete CSF examination.
Stage III (completion-authentication) was complaint with our SOP with median TAT being 12.5 minutes (30 minutes) Stage IV presenting phase exceeded our SOP desired TAT of 20 minutes as it showed median TAT of 55.5 minutes.
A careful study of all four phases of testing cycle gave us opportunity to redefine our laboratory CSF TAT from 170 minutes to 120 minutes (Table 1). This will require follow up and re audit after instituting the suggested changes.
Our study provides glaring evidence that can be used as a basis for making relevant changes in establishing laboratory TAT.
To conclude, TAT is an important parameter for the laboratory as well as for the hospital assessing the laboratory service. Hospitals need to evolve their own TAT in consultation with the laboratory personnel and the clinicians. Computerization and hospital information system are key ingredients in the process but above all is the review of TAT outliers and periodic audits. We found that TAT for CSF testing was actually falsely high in our cases where in spite of delay in printing, timely telephonic communication was done. Repeat sampling and printer problem were minor constraints. Laboratory TAT for CSF was redefined at much shorter span with the aim of improving customer satisfaction.
| Median TAT CSF samples (Minutes ) | Median TAT Glucose samples (Minutes) | |
|---|---|---|
| Within Laboratory | 107 | 46 |
| Total TAT | 177.5 | 82.5 |
Table 4: Comparisons of Total TAT and within Lab TAT for CSF and Plasma Glucose.
Recommendations
The following interventions to minimize the number of specimens delayed in reporting are suggested:
- The TAT for laboratory should include sample acceptance to sample authentication time only, sample collection to acceptance and sample authentication to printing should not be included as the factors responsible are beyond laboratory control involving clinical areas and software (printing).
- Faster preanalytical identification at laboratory reception.
- Improvement in report printing options in clinical areas to improve TAT.
- Redefined within Laboratory TAT : Total time- 60minutes ( Sample acceptance – Completion-45 minutes and Completion –Authentication-15 minutes)
- A re audit after 4 months for observing the effectiveness of interventions done as well as to summarize the current performance and consider potential interventions or more focused audits.
References
-
International Organization for Standardization (2012) ISO 15189:2012: Medical laboratories – requirements for quality and competence. Geneva, Switzerland: International Organization for Standardization.
-
College of American Pathologists. Laboratory Accreditation Program. Laboratory general checklist (components GEN 20316).
-
Plebani M, Sciacovelli L, Marinova M, Marcuccitti J, Chiozza ML (2013) Quality indicators in laboratory medicine: A fundamental tool for quality and patient safety. Clin Biochem 46(13-14): 1170-1174.
-
Goswami B, Singh B, Chawla R, Gupta VK, Mallika V (2010) Turnaround time (TAT) as a benchmark of laboratory performance. Ind J Clin Biochem 25(4): 376- 379.
-
Hawkins RC (2007) Laboratory turnaround time. Clin Biochem Rev 28(4): 179-194.
-
Pati HP, Singh G (2014) Turnaround time (TAT): difference in concept for laboratory and clinician. Indian J Hematol Blood Transfus 30(2): 81-84.
-
Steindel SJ, Howanitz PJ (2001) Physician satisfaction and emergency department laboratory test turnaround time. Arch Pathol Lab Med 125(7): 863-871.
-
Fei Y, Zeng R, Wang W, He F, Zhong K, Wang Z (2015) National survey on intra-laboratory turnaround time for some most common routine and stat laboratory analyses in 479 laboratories in China. Biochem Med (Zagreb) 25(2): 213-221.
-
Ricós C, García-Victoria M, de la Fuente B (2004) Quality indicators and specifications for the extra-analytical phases in clinical laboratory management. Clin Chem Lab Med 42(6): 578-582.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey