Prenatal Diagnosis of Gall Bladder Duplication
The fetal gallbladder appears as a small, hypoechoic, oval cyst-like structure located at the lower border of the liver. The gallbladder is one of the commonest body organs to have an anatomical variation, it may vary in number, shape or position and affects both the cystic duct and its artery equally. Gallbladder duplication are thought to be benign but are mostly associated with foregut malformations and aberrant hepatic and mesenteric vessels. A 26-year-old; primigravida at 20 weeks of gestation with diamniotic diachorionic (DADC) twins was found to have two fluid-filled; parallel tubular structures in the right upper quadrant of the liver suggestive of Boyden’s – Y shaped duplicated gall bladder in one of the foetuses meanwhile the other twin had a normal singular gall bladder. Preoperative delineation of variations of the hepatobiliary tract is of a paramount importance to avoid any potential damage to the ductal system as it is likely to easily overlooked and missed during surgery. Duplicated gallbladder after being detected prenatally in utero; the patient can be reassured for the benignancy of the outcome and prognosis.
Introduction
The gallbladder appears as a small, hypoechoic, oval cyst- like structure located at the lower border of the liver, close to the intestinal loops, and to the right of the intrahepatic umbilical vein. The fetal gallbladder shall be visualized in 65–82% of fetuses at 24–27 weeks’ gestation, however the detection rate reaches to 99% by transvaginal approach at 14–16 weeks’ gestation [1, 2]. The gallbladder is one of the body organs most subjected to anatomical variations; it may be related to number, shape or position and it might also affect the cystic duct and its artery [1]. Congenital anomalies of the biliary tree are rare; meanwhile the commonest is a choledochal cyst, with an incidence rate of 1 per 100,000 to 150,000 live births [3].
Anomalies of the gallbladder may be found 0.15% in antenatal sonographic examination and which includes abnormal position, agenesis, hypoplasia, duplication, an hourglass configuration, septations, and cysts. Duplication of the gallbladder is a rare congenital malformation, resulting in two separate gallbladder cavities, each with a cystic duct, occurring in about one per 4000 births [1, 4, 5, 6]. Gallbladder duplication have been reported; our review of the medical literature back to 1954 found only 3 reports with a total of 4 cases of describing duplication prenatally [5, 7, 8].
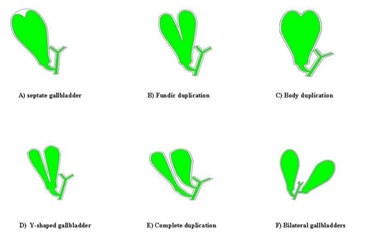
Several classifications have been proposed according to anatomic or embryologic development of the gallbladder; however double gallbladders are classified according to the Boyden’s classification [6].
Boyden’s classic description (Figure 1) defines gallbladder duplication as an embryologic anomaly whereby biliary tract development results in two separate gallbladder cavities and respective cystic duct. Boyden had conducted over 19,000 human cadaveric examination and delineated gallbladder duplication in only 5. The foremost human case of duplication is reported to be a sacrificial victim of the Emperor Augustus in 31 BC [9, 10].
Embryology
Abnormal biliary tract persistence and development of a vestigial out pouching of the biliary tree might lead to gallbladder duplication with two separate gall bladder cavities: with separate cystic ducts [11]. A case of triple gallbladder has also been reported in the literature, meanwhile gall bladder duplications are reported to be more common than bilobation [6, 12].
Associated Anomalies
Quite a few anomalies have been reported to be associated with gallbladder duplication most prominent of them being foregut malformations and aberrant hepatic and mesenteric vessels [9, 13]. A perception of an increased risk for acute and chronic cholecystitis, cholesterolosis, papilloma, carcinoma, biliary cirrhosis and torsion have been postulated but not yet been confirmed. Most notably, detection of gallbladder duplication shall be useful due to high prevalence of cholelithiasis and intermittent cystic duct obstruction [9, 13, 14].
Differential Diagnosis
Gallbladder folds, septum, and diverticulum of the gallbladder - Gallbladder folds are most commonly transverse and thus their ultrasonic appearance shall be different from the longitudinal division. Choledochal cyst - Choledochal cysts are spherical and not expected to lie along the gallbladder as in this case [14]. Gallbladder diverticulum. Hepatic cyst - Congenital hepatic cysts usually occur in the anterior segment of the right lobe. Mesenteric cyst persistence of a right umbilical vein - A persistent right umbilical vein is vascular and lies in the right of the gall bladder instead of parallel to it [7, 15]. In neither of these conditions; the said structure shall be seen lying adjacent and parallel to the gallbladder identified. Its characteristic appearance and unique location are the diagnostic and distinguishes from other pathological entities.
Case Report
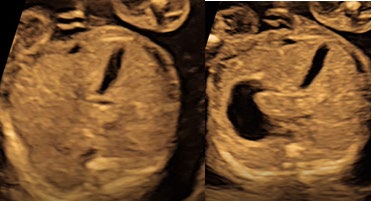
A 26-year-old; primigravida at gestational age of 20 weeks with diamniotic diachorionic (DADC) twins; was scheduled for fetal sonographic anatomic survey. Two fluid- filled; parallel tubular structures with anterior blind ending; were found in the right upper quadrant of the liver in one of the foetuses (Figure 2), other foetus have had a singular gall bladder (Figure 3).
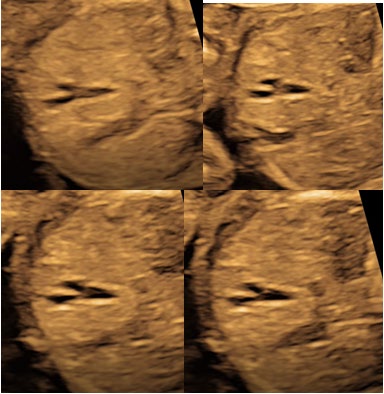
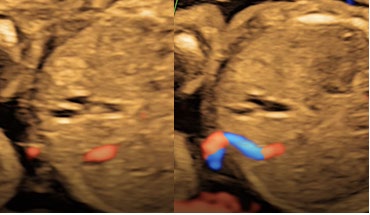
These structures being saccular in morphology; have a unique appearance with its characteristic location corresponded to Boyden’s – Y shaped duplicated gall bladder. Other probable diagnosis for an extracystic structure in the right upper quadrant were choledochal cyst, a mesenteric cyst, or a gastrointestinal duplication. Vascular malformations and a persistent right umbilical vein were excluded because of a lack of detectable blood flow during a routine ultrasound. No other detectable anomalies were found.
Discussion
Rarely, other biliary and foregut anomalies have been reported to be associated with gallbladder duplication postnatally in children and adults. Thus, the importance of gallbladder duplication identification lies in the possible common complications of gallstones and cholecystitis and its surgical or laparoscopic management.
Preoperative delineation of anatomical variations of the hepatobiliary tract is of a paramount importance to avoid potential damage to the duct system as an abnormal anatomy might be easily overlooked and missed during surgery [16].
When a duplicated gallbladder is detected prenatally in utero; the patient can be reassured for the benignancy of the finding as the prognosis for gallbladder duplication is good. The management remains is standard obstetric care.
References
-
Blazer S, Zimmer EZ, Bronshtein M (2002) Non visualization of the fetal gallbladder in early pregnancy: comparison with clinical outcome. Radiology 224(2): 379-382.
-
Hata K, Aoki S, Hata T, Murao F, Kitao M (1987) Ultrasonographic identification of the human fetal gallbladder in utero. Gynecol Obstet Invest 23(2): 79-83.
-
Howard ER (1991) Choledochal cysts. In: Howard ER (Ed.), Surgery of Liver Disease in Children. Oxford, England: Butterworth-Heineman, pp: 78-90
-
Benhidjeb T, Chaoui R, Kalache K, Mau H, Muller JM (1996) Prenatal diagnosis of a choledochal cyst: a case report and review of the literature. Am J Perinatol 13(4): 207-210.
-
Bronshtein M, Weiner Z, Abramovici H, Filmar S, Erlik Y, et al. (1993) Prenatal diagnosis of gall bladder anomalies: report of 17 cases. Prenat Diagn 13(9): 851-861.
-
Boyden EA (1926) The accessory gallbladder: an embryological and comparative study of aberrant biliary vesicles occuring in man and the domestic mammals. Am J Anat 38(2): 177-231.
-
Kinoshita LL, Callen PW, Filly RA, Hill LM (2002) Sonographic detection of gallbladder duplication: two cases discovered in utero. J Ultrasound Med 21(12): 1417-1421.
-
Sifakis S, Mantas N, Koumantakis G, Koukoura O (2007) Prenatal diagnosis of gallbladder duplication. Ultrasound Obstet Gynecol 30(3): 362-363.
-
Udelsman R, Sugarbaker PH (1985) Congenital duplication of gallbladder associated with an anomalous right hepatic artery. Am J Surg 149(6): 812-815.
-
Jastrow M Jr (1912) The liver as the seat of the soul. lr: Lyon, Moore, eds. Studies in the history of religions. New York, MacMillen, pp: 160.
-
Gross RE (1936) Congential anomalies of the gallbladder: a review of 148 cases with a report of double gallbladder. Arch Surg 32(1): 131-162.
-
Kurzewg FT, Cole PA (1979) Triplication of the gallbladder: review of literature and report of a case. Am Surg 45(6): 410-412.
-
Nichols DM (1983) Superior mesentric vein rotation: a CT sign of mid-gut malrotation. AJR Am J Roentgenol 141: 707-708.
-
Granot E, Deckelbaum RJ, Gordon R, Okon E, Sherman Y, et al. (1983) Duplication of the gallbladder associated with childhood obstructive biliary disease and biliary cirrhosis. Gastroenterology 85(4): 946-950.
-
Jeanty P (1990) Persistent right umbilical vein: an ominous prenatal finding?. Radiology 177(3): 735-738.
-
Mazziotti S, Minutoli F, Blandino A, Vinci S, Salamone I, et al. (2001) Gallbladder duplication: MR Cholangiography demonstration. Abdom Imaging 26(3): 287-289.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey