Extra Pulmonary Manifestations of COVID-19
COVID-19 is a pandemic impacting the world. SARS-CoV-2 is the 7th coronavirus to infect humans and the 3rd zoonotic virus after SARS-CoV and MERS-CoV. The full spectrum of clinical features of COVID-19 are yet to be investigated. The symptoms and signs of the COVID-19 is not specific. Since much of the information regarding the COVID-19 is still not known there are significant misconceptions regarding the clinical aspects of COVID-19 as a new emerging epidemic. The applicability of the information published regarding the virus in making decisions regarding patient care is uncertain. In this review article we have discussed all the clinical manifestations of COVID-19 by studying the literature published.
Introduction
The history of COVID-19 dates back to early November of 2019 when the literature available is studied. Formerly it was termed as “pneumonia of unknown etiology” because the cause of this disease was unknown. In early February the WHO named it as new CoV; “COVID-19 (coronavirus disease 2019).
The world has been struck by two similar corona epidemics previously in the past twenty years: SARS- CoV originating in China and MERS-CoV starting in Saudi Arabia both claiming 800 lives each. The CoVs viruses are vital culprits of respiratory disease outbreaks. These viruses consist of a single-stranded RNA virus that can be transmitted through various animals. These viruses can jump from animals to humans and cause diseases with symptoms ranging from mild to severe [1]. The pandemic originated from the wet market in Wuhan and soared like fire involving the entire globe. However, this particular virus is very potent, and the number of the affected individuals has largely outnumbered its brother coronaviruses. As compared to SARS and MERS, it would take a much longer time to bring the COVID-19 cases to half the number and controlling the disease. All over the globe research studies are underway to understand the virus and its transmissibility, severity, and other features [2]. Soon, following it was noticed that the virus spread in those individuals who never visited the wet market thus indicating a human to human transmission of the disease. Many clinicians have also contracted the virus while treating the infected individuals.
COVID-19 infection is acquired when a person is exposed to the virus. The vulnerable population that is the immunosuppressed and elderly are more susceptible to the disease. The age distribution of COVID -19 is ranging from twenty-five to eighty-nine years old [3]. It frequently involves the elderly and is less prevalent in the young population especially the children and infants [3, 4]. The median age is considered to be fifty-nine years of age. This virus generally has a male predominance (59%) [5]. COVID-19 is spread through droplets, contact with an infected individual through aerosol transmission. When an infected individual coughs or sneezes, the droplets disperse in the air and the other person may ingest or inhale those dispersed aerosols thus contracting the disease [6, 7]. Since COVID-19 can cause diarrhea and abdominal pain a few studies point out that there could be a transmission through the fecal-oral route as well. Thus, postulating that ACE2 is markedly present on the enterocytes from ileum and colon and COVID 19 works by binding to the ACE2 receptor [8]. Pneumonia caused by COVID-19 is known as severe acute respiratory syndrome coronavirus2(SARS-CoV2). The CoV2 virus has an envelope and granules. This pneumonia is highly infectious, and it is diagnosed by clinical manifestations, along with CT scan and nucleic acid detection of SARS-Cov2. The mortality rate of COVID-19 is increasing leaps and bounds with the number of deaths climbing to over fifty-three thousand by 3rd April 2020, with a case fatality rate of 2-3% [9, 10].
Clinical Features
COVID‐19 symptoms range in severity. They are divided into four classes: mild, moderate, severe, and critical. Mild patients present only with slight symptoms with no Chest Xray findings. Moderate patients present with modest fever, dry cough, and radiographical findings. Severe symptoms should include either dyspnea, respiratory rate greater than 30 per minute, or a PaO2/FiO2 less than 300 mm Hg. Whereas the critical patients should have either respiratory failure, multi- organ failure or septic shock, these patients usually have a grave prognosis. Hence concluding the spectrum of COVID-19 symptoms is very vast. The basic clinical symptoms of the disease consist of cough, malaise, decreased energy, and at times diarrhea accompanied by abdominal pain. Patients who are immunocompromised and the elderly tend to suffer from a more serious disease and are usually associated with acute respiratory distress syndrome (ARDS) and cytokine storm.
The mode of transmission of COVID-19 is by respiratory droplets [5]. Early in February 2020 COVID-19 was also found in the fecal swabs of patients suffering from COVID 19 pneumonia at Sun Yat-Sen University, Guangdong, China. Zhang et al. also found COVID 19 virus in samples taken from blood and feces of the subjects suffering from active COVID 19 infection thus indicating multiple routes of transmission [11]. ACE2 protein is present in the vast majority in the epithelial cells of the alveoli of the lungs as well as the enterocytes of small gut thus pointing out to the two primary presumed routes of transmission. The incubation period of the disease is approximately one day to two weeks. The disease is even transmissible during the latency period.
Young patients suffering from SARS-CoV-2, COVID-19 presented with a few complaints of fever, malaise, and cough and flu-like disease in the majority of cases [12]. Whereas a few presented with more gruesome disease rapidly deteriorating to acute respiratory distress syndrome, respiratory failure, multiple organ failure, thus ultimately culminating to death [10]. Due to the large variability in the spectrum of symptoms the disease there is no ultimate pathognomonic clinical picture of the disease. Though many studies claimed that this disease usually presents with fever but a large cohort study claimed that fever was only present on 44 percent of the patients with COVID 19 at the time of hospital admission thus highly questioning fever as a primary symptom of the disease [10]. In several cases diarrhea may precede fever and can be the first symptom to appear in some individuals followed by fever. Thus, pointing out that fever is the most dominant symptom of the disease but not the primary one. Following fever, the second most commonly experienced symptom is a cough that is usually dry in character.
Usually symptoms of the COVID around the world are mild with a study indicating that more than eighty percent of the cases were mild [13]. However, on the other hand ten percent were in critical condition. The cause of the range of symptoms is not known. The clinical progression of the disease should be well studied. The disease can come in phases with the first phase usually consisting of fever, cough, and malaise; with fever being the most common finding. Guan et al. performed a study in which almost half (43.8%) of the patients had a fever while they presented to the hospital and almost 87.9% acquired it following hospitalization. Thus, pointing out that the patients can be afebrile during the early phase of the disease [10]. The fever of COVID 19 was prolonged as compared to SARS (11.4 days), MERS (8 days) [14, 15, 16]. Patients with SARS have a recurrent fever spike during the second week of the disease whereas in COVID 19 the patient became afebrile thereafter [17]. Prof. Nan-Shan Zhong’s performed a study on approximately thousand individuals with this disease and stated that fever (88.7%), cough (67.8%), fatigue (38.1%), sputum production (33.4%), shortness of breath (18.6%), sore throat (13.9%), and headache (13.6%) [10]. Some patients also complained of having sneezing, rhinorrhea, and a sore throat. These symptoms point out that the target cells of the COVID 19 virus may be found in the lower airway tract.
A few studies show that COVID 19 was not found in the urine samples of the disease, but urine samples should be tested further to look for the different modes of transmission of the disease. The other major symptoms are fatigue. A study showing fatigue in approximately (69.6%) of the individuals with the disease, and diarrhea [18, 19]. Less common symptoms included malaise, pain in muscles and joints, headache, and altered consciousness, confusion and chest pain and productive cough, nausea, and vomiting [18, 19]. A handful of patients with COVID-19 also complain of a stuffy nose and productive cough. Patients with advanced age and co-morbidities including hypertension, diabetes, cardiovascular diseases, and chronic obstructive pulmonary diseases and asthma have a chance of rapidly deteriorating into acute respiratory distress syndrome, septic shock, electrolyte disturbances, and metabolic acidosis. Affected individuals can even suffer from abnormalities of the coagulation system thus ultimately leading to stroke. Whereas most young patients and even children have a good prognosis. Patients with 2019-nCoV can even develop severe pneumonia and pulmonary edema.
A slight number of patients also presented with headache or hemoptysis and even with no symptoms [20, 21]. Roughly around every 4th individual contracting the disease (5% of all infected patients), is critically ill either with shock, ARDS and needing ventilatory support.
Some individuals with SARS-CoV-2 do not exhibit any symptoms but are found to be the transmitters of the disease and can act as carriers [10]. Symptoms and signs of COVID 19 are not specific [22].
Many of the ear nose throat specialists around the world found that one of the symptoms that the infected individuals experienced was decreased or complete loss of sense of smell. This symptom occurred in approximately 2/3rd of the patients [23, 24].
COVID 19 is also found to cause inflammation of the conjunctiva leading to conjunctivitis [25, 26]. Thus, it is presumed it has an ocular spread too. A few infected cases also reported cutaneous lesions. A cohort study performed on eighty-eight patient subjects showed that the cases had an erythematous rash, vesicles, or urticaria. The area most commonly involved was the trunk. Itching was less pronounceable. These lesions were self-resolving not requiring any intervention [27]. Another study performed stated the common features of the disease were fever, cough, fatigue, along with shortness of breath in 15-20 percent of the cases. A few cases had palpitations and chest tightness [28].
Middle East respiratory syndrome-related coronavirus (MERS-CoV) can lead to myocardial inflammation and heart failure. Since SARS-CoV-2 and MERS-CoV have similar pathogenicity, COVID 19 can also lead to similar outcomes. Myocardial damage was reported in approximately 5 of the 41 patients with COVID-19 in Wuhan. This was detected as a spike in the cardiac troponin 1 levels (>28 pg/ml) [20]. 80 % of the patients with myocardial damage were admitted in the intensive-care unit (ICU), thus pointing to the gruesome nature of the disease. Even the blood-pressure levels were significantly higher as compared to those not treated in the ICU [20]. ACE2 is found to be present in excessive amounts even in the cardiovascular system thus pointing to the possible mechanism of the spread of the disease leading to myocarditis and injury to the heart. A few other cardiac complications were recent or deterioration of existent heart failure, arrhythmia, or myocardial infarction especially in critically ill patients. Cardiac arrest was reported in approximately 3% of the individuals with pneumonia.
Disease spectrum in neonates, infants, and children were comparatively milder. Usually the affected children barely have any symptoms. No critical cases were seen. The most frequent findings were fever and cough. The prognosis is good. Only one child was reported to have severe pneumonia and multi-organ failure [29]. But no deaths are reported. Similarly, the neonatal cases had only mild symptoms [30].
COVID-19 patients with involvement of the gastrointestinal tract system complaining of diarrhea and abdominal pain have a bad clinical outcome and these symptoms put them at higher risk of mortality compared to those without these symptoms. Thus, diagnosing these in time can help with patient care and outcome.
Liver injury can also be associated with COVID 19, whereas some studies point out to the opposite [31, 32, 33]. It is yet unknown if there is any association with the COVID 19 leading to liver abnormalities but these variations should be further investigated. Usually the patients experiencing the gastrointestinal symptoms of the virus had elevated liver tests, such an AST and ALT. This is a topic worthy of attention. Huang et al. reported the derangement of aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, lactate dehydrogenase, and prothrombin time (PT) in patients with COVID 19 pneumonia [19]. Xu, et al. performed a liver biopsy of patients with COVID 19 thus reported steatosis and liver injury in a few of the affected individuals [34]. A recent case study performed on a Washington nursing home, showed nearly 1/3 of the inhabitants tested positive for the virus, and ½ had no symptoms. A few among those reported malaise, discomfort, uneasiness, and feeling queasy.
In some cases, COVID-19 may also present with symptoms of altered mentation or exhaustion. A case report on a 79-year-old man with COVID 19 and no history of hypertension or being on anticoagulants presented to the emergency with acute loss of consciousness. A CT scan showed massive Intracerebral hemorrhage, Intraventricular, and subarachnoid hemorrhage [35]. Thus, pointing out that COVID 19 can also lead to neurological outcomes.
Patients with COVID-19 may suffer from grave sepsis and these patients have a poor prognosis. The signs of sepsis in these patients include shortness of breath, low oxygen saturation, decreased urinary output, increased heart rate, hypotension, cold extremities, skin, and altered consciousness [36]. The laboratory tests include acidosis, increased lactate levels, increased bilirubin, decreased platelet count, and coagulation dysfunction [36].
Kidney is one of the organs that is affected in the COVID 19 cases. Studies point out that kidney tubules are damaged by the virus, altering the glomerular filtration rate and mounting the blood creatinine and blood urea nitrogen levels [37, 38]. The symptoms of patients with COVID 19 and associated kidney damage had hematuria, proteinuria and kidney dysfunction. The patients with kidney involvement had a bad prognosis. Clinicians should raise their knowledge regarding the kidney damage associated with the infection [39].
Usually COVID 19 patients present with a common complaint of fatigue, malaise, and generalized tiredness but in some patient’s focal muscular pain. Thus, pointing out that rhabdomyolysis may be caused by the virus. A case report indicated a 60-year-old man having rhabdomyolysis due to COVID 19 points out to the musculoskeletal involvement of the disease [40].
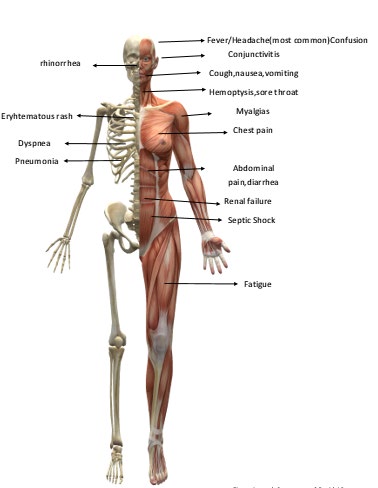
Many studies point to the coagulation dysfunction caused by coronavirus 2019 (COVID-19). The patients have markedly elevated D-dimer levels and thus are associated with a poor prognosis [41]. Patients usually have higher D‐ dimer and fibrin degradation product (FDP) levels, longer prothrombin time, and activated partial thromboplastin time. Patients infected with 2019-nCoV also had high amounts of IL1B, IFNγ, IP10, and MCP1, GCSF, IP10, MCP1, MIP1A, and TNFα probably leading to activated T-helper-1 (Th1) cell responses. Thus, an indication that the cytokine storm was linked to disease severity. COVID 19 also causes increased secretion of T helper 2 cytokines that hamper inflammation. Serologic tests in some patients may be positive for anticardiolipin IgA, anti–β2-glycoprotein I antibodies. There is also evidence of a destroyed immune system revealed by atrophy of spleen and lymph nodes. Another study pointed out that approximately 36 percent of the individuals had involvement of the central or peripheral nervous system and skeletal muscle involvement. Severe patients experienced acute cerebrovascular is disease, conscious disturbance, and muscle injury [42]. COVID 19 can also cause muscle involvement leading to skeletal muscle injury, indicated by increased creatine kinase and lactate dehydrogenase levels. The neuro-invasive proneness is seen in all βCoVs. Accumulating evidence suggests that patients with severe COVID-19 might have a cytokine storm syndrome [43]. SARS-CoV-2 infection is responsible for various neurological manifestations. A case report has been published linking COVID 19 to the development of Guillain-Barré syndrome [44]. Figure 1 showing symptoms of COVID 19.
Conclusion
Misinterpreting the evidence in clinical practice leads to wrong decisions thus affecting the clinical outcomes during the initial stages of this epidemic. The disease spectrum varies, and the non-resolving fever, lung damage, and disease progression can be explained by unrestrained viral replication. Thus, an appropriate potent antiviral that effectively reduces the viral load may play a vital role in the halt of disease progression. Several drugs that inhibit the virus replication, including remdesivir are under investigation. Recently it has shown to speed recovery with the disease. Since there is a wide variability in the disease presentation, diagnosis of certain biomarkers and a clinical criterion should be established that helps identify and prioritize the cases that require prompt treatment.
COVID 19 affects the cardiovascular and renal function and proper cardiovascular protection should be taken in account while treating the disease. Acute kidney injury is also associated with a poor prognosis. Therefore, in the clinical diagnosis and treatment of COVID-19, acute kidney injury should be taken in account as well. The war against COVID-19 has set foot into a critical phase. More extensive and detailed studies are required to understand the full range of spectrum of ailments caused by this virus, its pathogenesis, and the longer-term morbidity. The possibility of persistent and relapsing infections is still not known. More information is urgently needed on the disease in pregnancy, immunocompromised, and fetal infection. We still must investigate the outcome of past exposure to other CoV viruses on modifying current COVID 19 disease severity.
The coagulation dysfunction is crucial and should be monitored sharply. Currently role of anticoagulation therapy is under investigation. Fecal and urine samples should be investigated and tested promptly to look for another route of transmission that is unknown at this point. This virus requires deep study as it is a global health threat. Reliable quick testing should be available. Surveillance is essential to look for host adaption, viral evolution, infectivity, and transmissibility. The neurological manifestations of the disease should also be taken into account as they carry a poor prognosis. 2019- nCoV infection may be associated with cellular immune deficiency, coagulation activation, myocardial, kidney and hepatic involvement. SARS-CoV-2 spread can be decreased by social distancing but proper vaccination in necessary. Gradually it will attenuate to the status of being another virus like a common cold. Early diagnosis and improved treatment of severe cases hold the key to reduce mortality. As more research accrues on the prevention and control measures the outcomes will improve. The extreme of ages and those that are immunocompromised are at the most significant risk. All clinicians should understand the presentation of the disease, its clinical features, workup, and treatment. Further, clinicians should be aware of the precautions vital to avoid acquiring the disease. COVID -19 pandemic is a vital test for the medical community. Dealing with COVID 19 with limited resources and insufficient data is tough. Human and material resources should all be put forward in helping to diagnose and fight off the disease together.
References
-
Perlman S, Netland J (2009) Coronaviruses post-SARS: update on replication and pathogenesis. Nat Rev Microbiol 7(6): 439-50.
-
CDC (2020) 2019 Novel coronavirus, Wuhan, China.
-
Medical expert group of Tongji hospital (2020) Quick guide to the diagnosis and treatment of pneumonia for novel coronavirus infections (third edition). Herald Med.
-
Wang C, Wang X (2020) Prevalence, nosocomial infection and psychological prevention of novel coronavirus infection. Chin General Pract Nurs 18: 2-3.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med 382(13): 1199-1207.
-
(2020) National Health Commission of People’s Republic of China. Prevent guideline of 2019-nCoV.
-
(2020) National Health Commission of People’s Republic of China. Pneumonia diagnosis and treatment of 2019- nCoV infection from Chinese NHC and CDC 2020.
-
Zhang H, Kang Z, Gong H, Xu D, Wang J, et al. (2020) The digestive system is a potential route of 2019-nCov infection: a bioinformatics analysis based on single-cell transcriptomes. bioRxiv.
-
Wuhan Coronavirus (2019-nCoV) Global Cases (by Johns Hopkins CSSE).
-
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. The New England journal of medicine 382: 1708- 1720.
-
Zhang W, Du RH, Li B, Zheng XS, Yang XL, et al. (2020) Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerg Microbes Infect 9(1): 386-389.
-
Poutanen SM, Low DE, Henry B, Finkelstein S, Rose D, et al. (2003) Identification of severe acute respiratory syndrome in Canada. N Engl J Med 348(20):1995-2005.
-
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA 323(13): 1239-1242.
-
Zhong NS, Zheng BJ, Li YM, Poon Xie ZH, Chan KH (2003) Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, people’s republic of China, in February, 2003. Lancet 362(9393): 1353-1358.
-
Choi WS, Kang CI, Kim Y, Choi JP, Joh JS, et al. (2016) Clinical presentation and outcomes of middle east respiratory syndrome in the republic of Korea. Infect Chemother 48(2): 118-126.
-
Lau SK, Woo PC, Yip CC, Tse H, Tsoi HW, et al. (2006) Coronavirus HKU1 and other coronavirus infections in Hong Kong. J Clin Microbiol 44(6): 2063-2071.
-
Peiris JS, Chu CM, Cheng VC, Chan KS, Hung IF, et al. (2003) Clinical progression and viral load in a community outbreak of coronavirus-associated sars pneumonia: a prospective study. Lancet 361(9371): 1767-1772.
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507‐513.
-
Huang C, Wang Y, Li X, Lili Ren, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497‐ 506.
-
Wang D, Bo Hu, Chang Hu, Fangfang Zhu, Xing Liu, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 323(11):1061-1069.
-
Chan JF, Yuan S, Kok KH, Kelvin Kai-Wang To, Chu H, et al. (2020) A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to- person transmission: a study of a family cluster. Lancet 6736(20): 30154-30159.
-
WHO (2020) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) Report. World Health Organization (WHO).
-
Hopkins C, Kumar N (2020) Loss of sense of smell as marker of COVID-19 infection (letter). ENT UK, pp: 1-2.
-
Lüers JC, Klußmann JP, Guntinas-Lichius O (2020) The COVID-19 pandemic and otolaryngology: What it comes down to?. Laryngo- rhino- otologie 99(5): 287-291.
-
Ping Wu, Fang Duan, Chunhua Luo, Qiang Liu, Xingguang Qu, et al. (2020) Characteristics of Ocular Findings of Patients With Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmology 138(5): 575-578.
-
Chen L, Liu M, Zhang Z, Qiao K, Huang T, et al. (2020) Ocular manifestations of a hospitalised patient with confirmed 2019 novel coronavirus disease. The British journal of ophthalmology 104(6): 748-751.
-
Recalcati S (2020) Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol 34(5): e212-e213.
-
Zheng YY, Ma YT, Zhang JY, Xie X (2020) COVID-19 and the cardiovascular system. Nature reviews. Cardiology 17: 259-260.
-
Chen F, Liu ZS, Zhang FR, Rui-hua X, Chen Y, et al. (2020) First case of severe childhood novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 58(0): E005.
-
Zeng LK, Tao XW, Yuan WH, Wang J, Liu X, et al. (2020) First case of neonate infected with novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 58(0): E009.
-
Yao N, Wang SN, Lian JQ, Sun YT, Zhang GF, et al. (2020) Clinical characteristics and influencing factors of patients with novel coronavirus pneumonia combined with liver injury in Shaanxi region. Zhonghua Gan Zang Bing Za Zhi 28(3): 234-239.
-
Hu LL, Wang WJ, Zhu QJ, Yang L (2020) Novel coronavirus pneumonia related liver injury: etiological analysis and treatment strategy. Zhonghua Gan Zang Bing Za Zhi 28(2): 97-99.
-
Wu J, Liu J, Zhao X, Liu C, Wang W, et al. (2020) Clinical Characteristics of Imported Cases of COVID-19 in Jiangsu Province: A Multicenter Descriptive Study. Clin Infect Dis.
-
Xu Z, Shi L, Wang Y, Zhang J, Huang L, et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med 8(4): 420-422.
-
Sharifi-Razavi A, Karimi N, Rouhani N (2020) COVID 19 and Intra cerebral hemorrhage: Causative or Coincidental, New Microbes and New Infections 35.
-
Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Napoli RD (2020) Features, Evaluation and Treatment Coronavirus (COVID-19). Stat Pearls Publishing, Treasure Island.
-
Hui DSC, Zumla A (2019) Severe acute respiratory syndrome: historical, epidemiologic, and clinical features. Infect Dis Clin North Am 33 (4): 869-889.
-
Joob B, Wiwanitkit V (2014) Novel Middle East respiratory syndrome and renal failure. Ren Fail 36(1): 147.
-
Cheng YC, Luo R, Wang K, Zhang M, Wang Z, et al. (2020) Kidney impairment is associated with in-hospital death of COVID-19 patients. medRxiv.
-
Jin M, Tong Q (2020) Rhabdomyolysis as potential late complication associated with 2019 novel coronavirus disease. Emerg Infect Dis 26(7): 1618-1620.
-
Gibson WJ, Nafee T, Travis R, Yee M, Kerneis M, et al. (2020) Machine learning versus traditional risk stratification methods in acute coronary syndrome: a pooled randomized clinical trial analysis. J Thromb Thrombolysis 49(1): 1-9.
-
Mao L, Wang M, Chen S, He Q, Chang J, et al. (2020) Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. medRxiv.
-
Poyiadji N, Shahin G, Noujaim D, Stone M, Patel S, et al. (2020) COVID-19–associated Acute Hemorrhagic Necrotizing Encephalopathy: Imaging Features Radiology 296: 2.
-
Zhao H, Shen D, Zhou H, Liu J, Chen S (2020) Guillain- Barré syndrome associated with SARS-CoV-2 infection: causality or coincidence?,. The Lancet Neurology 19(5): 383-384.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey