Advanced Heart Block in a Young Adult: CMR is Savior
Advanced heart block in young adults is rare and more likely to result from non-ischemic cardiovascular diseases. Early identification of conduction disorder and myocardial tissue characterization are important clinical entities for definitive diagnosis, early treatment, and prevention of adverse cardiovascular outcomes. We present a case of cardiac sarcoidosis with no clinical manifestations other than complete heart block rhythm and presyncope. We demonstrated the critical role of CMR in the diagnosis of CS especially when other investigations failed to confirm sarcoid infiltration.
Introduction
Sarcoidosis is a multi-system disorder that involves lymph nodes, lungs, eyes, and skin. However, cardiac manifestations of sarcoidosis are not uncommon. It is now being recognized as one of the important causes of mortality in sarcoidosis patients. Novel cardiac imaging modalities like cardiac MRI have made it possible for the earliest identification of myocardial involvement during and after active sarcoidosis.
Case Report
A 27-year-old nondiabetic nonhypertensive male presented with progressively increasing episodes of presyncope for one month. His blood pressure was 104/68 mmHg and his heart rate was 36-40 bpm. ECG reveals no relationship between P waves and qrs complexes indicating complete heart block rhythm. Patient was conscious and oriented with a relatively asymptomatic period during mild physical activity. Patient also acknowledges the loss of weight over 2 years with insignificant temperature variations. Echocardiography study reveals mild thickening of the interventricular septum (IVS) and normal biventricular systolic function (Figure 1A). Chest X-ray reveals insignificant bronchovascular prominence and no signs of any mediastinal mass or pleural effusion. His hemoglobin level was 14.1 gm%, serum calcium 11.9 mg/dL, leukocyte counts, and serum electrolyte levels were within normal limits and troponin-I was negative.
With suspicion of any underlying atherosclerotic lesion or coronary anomalies, conventional coronary angiography was performed which reveals completely normal epicardial coronary arteries. Considering the uncommon CHB in a young adult in the absence of coronary artery disease or any known systemic diseases, a cardiac magnetic resonance (CMR - Philips Ingenia 3.0T) study was suggested to rule out any underlying myocardial diseases. Interestingly, the CMR study reveals significant subendocardial myocardial edema of the left ventricle on T2-stir-based imaging sequences (Figure 1B). Moreover, the delayed gadolinium enhancement shows a mid-myocardial scar of basal IVS (Figure 1C & Figure 1D white arrows). There was no evidence of subepicardial or subendocardial fibrosis. Pericardial effusion was evident over the basal inferior wall of the right and left ventricular walls (Figure D red arrow). CT thorax study shows marginally enlarged mediastinal lymph nodes without any evidence of active inflammatory changes. Under suspicion of cardiac involvement of active sarcoidosis, angiotensin- converting enzyme (ACE) level was investigated and was found marginally elevated to 48 U/L. Patient was treated medically including steroids. Follow up examination after 1 week, 1 month and 3 months were unremarkable with sinus rhythm on ECG.
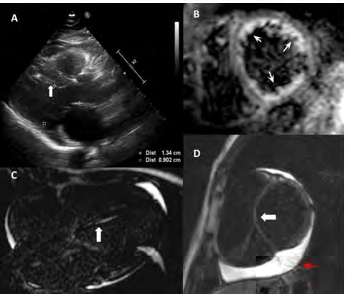
Figure 1A-1D: Nondiabetic Nonhypertensive. Figure 1A: Echocardiography study in apical 3-chamber view - long-axis shows increased thickness of basal IVS. Figure 1B: Significant sub-endocardial edema in basal portion of the LV (T2-stir image). Figure 1C: Gadolinium contrast-enhanced CMR scan; 4-chamber view demonstrating areas of hyperenhancement in basal IVS. Figure 1D: LV Short Axis view demonstrating delayed gadolinium enhancement in mid-myocardium of basal IVS & significant pericardial effusion (depicted by white arrows).
Discussion
Cardiac sarcoidosis (CS) can be almost asymptomatic; however, it is a life-threatening disorder that can cause fatal ventricular tachyarrhythmia, conduction disturbances, left ventricular dysfunction, and sudden death [1]. Complete heart block is the first most common and ventricular tachycardia/fibrillation is the second most common cause of the cardiac involvement of sarcoidosis [2]. Although cardiac involvement is only clinically diagnosed in about 5% of patients with systemic sarcoidosis, the incidence of autopsy-proven sarcoidosis involving the myocardium ranges from 13–27% [1, 3]. Cardiovascular complications are always underdiagnosed in sarcoidosis as the manifestations are unclear and steroid-responsive patients are always benefitted from medical therapy before major cardiovascular complications like LV remodeling and dysfunction occur. However, steroid response might not be possible in fibrotic or scarred myocardial tissue3. As our case depicts, it is unusual for a sarcoid patient to present first with cardiovascular complications like advanced heart block, it paves the way to understand premature cardiovascular complications as a consequence of systemic inflammatory disorders.
It is essential to learn from this case that sarcoidosis with only cardiac manifestations are more likely to have adverse outcomes and early diagnosis is critical for favorable clinical outcome. This case also confirms the previous observations of common locations of late gadolinium enhancement in sarcoidosis at intramural sites of basal IVS as reported by Komada, et al. [4]. Hence, the distribution of late gadolinium enhancement is a more sensitive marker for cardiac sarcoidosis. In the absence of any adverse hemodynamic events, temporary or permanent pacemaker implantation should not be considered for the management of conduction abnormalities until the CMR study is completed as the availability of MRI-compatible pacemakers is uncommon.
The features of sarcoidosis on echocardiography include regional wall motion abnormalities which are nonspecific. Nuclear scintigraphy is also poorly sensitive and specific due to its suboptimal spatial resolution and artifacts whilst despite the requirement for histopathological evidence to make a definite diagnosis of cardiac sarcoidosis, the sensitivity of endomyocardial biopsy is still low due to the patchy nature of infiltration [5]. CMR offers a highly perceptive noninvasive method for the assessment of myocardial fibrosis and infiltration and in some cases eliminates the need for biopsy. In our patient, we demonstrated the critical role of CMR in the diagnosis of CS especially when other investigations failed to confirm sarcoid infiltration [6].
Conclusion
Our case report highlights the role of advanced cardiac imaging in the diagnosis of uncommon cardiomyopathies including suspected cardiac sarcoidosis. Primary management is critical to prevent life-threatening complications of CS. Specifically, timely diagnosis and pharmacological intervention will prevent the development of ventricular dysfunction which is usually the late phase of sarcoid cardiomyopathy. Cardiac MRI should be the choice of modality in cardiac involvement of sarcoidosis for diagnosis and prognostication. Further research addressing the MR pulse sequences to increase the sensitivity of CMR for diagnostic accuracy of CS is essential.
References
-
Silverman KJ, Hutchins GM, Bulkley BH (1978) Cardiac sarcoid: a clinicopathologic study of 84 unselected patients with systemic sarcoidosis. Circulation 58(6): 1204-1211.
-
Kusano KF, Satomi K (2016) Diagnosis and treatment of cardiac sarcoidosis. Heart 102(3):184-190.
-
Sharma OP, Maheshwari A, Thaker K (1993) Myocardial sarcoidosis. Chest 103(1): 253-258.
-
Takaya Y, Fukushima K, Nakamura K, Kaji M, Shinya T, et al. (2014) Reduction of myocardial inflammation with steroid is not necessarily associated with improvement in left ventricular function in patients with cardiac sarcoidosis: predictors of functional improvement. Int J Cardiol 176(2): 522-525.
-
Tomohiro K, Kojiro S, Ishiguchi H, Kawai H, Okumura T, et al. (2016) Magnetic resonance imaging of cardiac sarcoidosis: an evaluation of the cardiac segments and layers that exhibit late gadolinium enhancement. Nagoya J Med Sci 78(4): 437-446.
-
Tsushima T, Sasaki S, Yuda S, Ohta M, Cammack I, et al. (2019) Remaining challenges in the diagnosis of early stage cardiac sarcoidosis. Clin Case Rep 7(5): 1007-1011.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey