Two Rare Complications of Acute Bacterial Meningitis Subarachnoid Hemorrhage and Intraventricular Hemorrhage in a Single Frame: A Case Report
Meningitis can lead to severe and disabling neurological consequences if diagnosis and treatment is delayed. There are multiple complications associated with meningitis including cerebrovascular accidents. Subarachnoid hemorrhage is one of the rarest complications and carries worse prognosis. Early diagnosis and immediate management is the key for survival in patients with intracranial hemorrhage secondary to meningitis. This is a case of 65-year-old male with no established premorbid who presented with 2 weeks history of high-grade fever and altered sensorium for 3 days. On examination he was vitally stable but irritable with Glasgow coma scale of 11/15. Neck stiffness was positive with negative Kernig’s and Brudzinski’s sign. There was no other focal neurological deficit. Respiratory, CVS, GIT and Musculoskeletal examination was unremarkable. Complete blood picture showed raised leucocyte count. C-reactive protein and Erythrocyte sedimentation were also raised. Liver function tests, Renal function tests, Electrolytes, Urine routine examination, Electrocardiography and chest x-ray was normal. CT brain was done which was normal. Lumber Puncture was done which was suggestive of bacterial meningitis. Antibiotics were started and the patient’s GCS improved to 15/15. After 3 days patient GCS suddenly dropped to 8/15. CT brain was repeated which showed subarachnoid hemorrhage with intraventricular extension and mild obstructive hydrocephalous. External Ventricular Drain was placed and patient improved significantly.
Background
Acute pyogenic meningitis is a central nervous system infection and is a medical emergency with approximately one-third of the patients suffering from complications and very few developing long term sequalae. Neurological complications secondary to pyogenic meningitis can lead to significant mortality and morbidity. Both ischemic and hemorrhagic strokes can occur in bacterial meningitis with hemorrhage relatively uncommon compared to ischemia. Subarachnoid hemorrhage is an exceedingly rare complication associated with bacterial meningitis which occurs mainly due to ruptured aneurysms or inflammatory arteritis. Early detection and proper antibiotic treatment usually improve survival outcomes. This is one such case of bacterial meningitis that developed subarachnoid hemorrhage.
Case Presentation
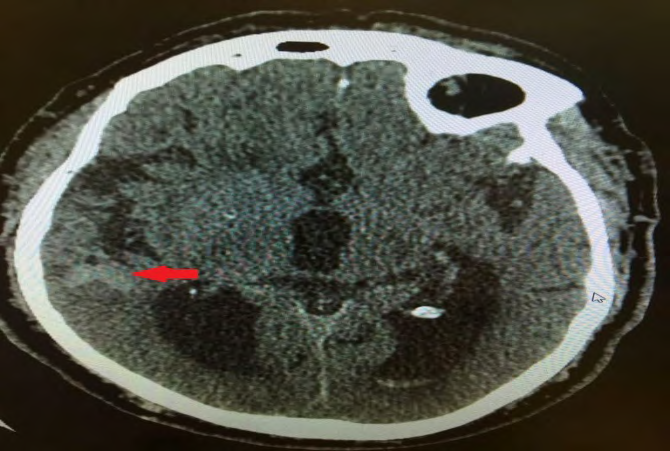
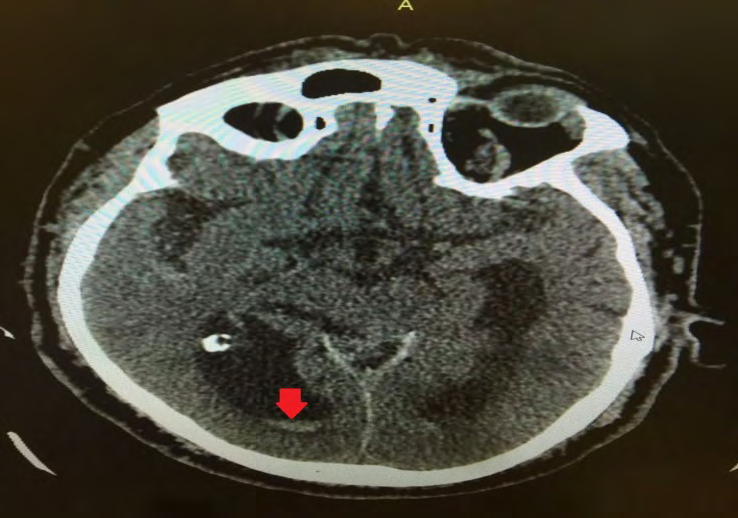
A 65-year-old male old male with no established premorbid presented with high-grade fever for last 2 weeks and altered sensorium for 3 days. At presentation he had vitals of BP 130/80, Pulse 102, Temperature 102F, and Oxygen saturations 98% at Room air. He was irritable with Glasgow coma scale of 11/15. Neck stiffness was positive with negative Kernig’s and Brudzinski’s sign. There was no other focal neurological deficit. Respiratory, CVS, GIT and Musculoskeletal examination was unremarkable. Complete blood picture showed raised leucocyte count of 21,000 with normal hemoglobin and platelet count. C-reactive protein was 205 and Erythrocyte sedimentation rate was 69. Serum glucose random was 158 mg/dl. Liver function tests, Renal function tests, Electrolytes, Urine routine examination, Electrocardiography and chest x-ray was normal. CT brain was done which was normal. Patient was admitted and Lumber Puncture was done. Cerebrospinal Fluid Analysis showed WBC count 1000/cmm with Neutrophils 80%, Glucose 40mg/dl, Proteins 121mg/dl, Gram stain No organism, ZN stain No acid-fast bacilli seen. Cerebrospinal fluid culture showed growth of Staphylococcus aureus. Antibiotics were started and the patient’s GCS improved to 15/15. After 3 days patient GCS suddenly dropped to 8/15 again. CT brain was repeated which showed subarachnoid hemorrhage (Figure 1) with intraventricular extension and mild obstructive hydrocephalous (Figure 2). External Ventricular Drain was placed and patient condition improved. EVD was removed after 3 days. Patient then developed Hospital acquired pneumonia and sepsis. Currently patient is under treatment for this.
Discussion
Meningitis is a central nervous system infection with rare complications. To best of author’s knowledge cases till yet showed subarachnoid hemorrhage as sequalae with high morbidity and mortality. Unusual about our case was that patient developed both subarachnoid hemorrhage and intraventricular hemorrhage which were managed in time along with treatment of meningitis with improved outcomes.
Acute bacterial meningitis has high risk of complications with fatal outcomes and is considered as a medical emergency [1]. Local complications associated with meningitis include tonsillar herniation, myelitis, cord infarction, arachnoiditis, epidural abscess formation while systemic include shock, respiratory failure, septicemia and coagulation disorders [1, 2].
Morbidity and mortality due to local complications usually occur within 2 weeks of admission while late deaths i.e. more than 2 weeks are mostly due to systemic complications [1]. Various studies have showed that in elderly patients, septicemia and respiratory failure are the most common causes of death in pyogenic meningitis while in young patients, local complications like brain herniation is the most common cause [1].
Arterial infarction and cerebral vein thrombosis are commonly identified complications of meningitis. Although subarachnoid hemorrhage can be associated with viral encephalitis particularly HSV but it is an extremely rare recognized complication of pyogenic meningitis [3, 4]. Most of the cerebrovascular accidents in meningitis are ischemic strokes with hemorrhagic strokes occurring very rarely [4].
Exact cause of ischemic stroke is not known but proposed mechanisms include focal hypoperfusion, vasospasms, septic embolization and diffuse cerebral intravascular coagulation [4]. The basic pathogenic mechanism involved in the development of SAH is hypothesized to be vasculitis or ruptured mycotic aneurysms secondary to dysregulation of coagulation and fibrinolytic pathways, vascular endothelial cell swelling and activation, and acute inflammation of subarachnoid space from meningitis [3, 4, 5].
Patients who present with non-traumatic or non- aneurysmal SAH meningitis should be ruled out as one of the differential diagnosis as both have completely different management [3]. Brain damage caused by hemorrhage in pyogenic meningitis carries high risk of morbidity and mortality [4, 5]. Better outcomes can be obtained with early diagnosis and prompt institution of antimicrobial therapy [4].
Conclusion
Meningitis remains an important global health ailment despite of effective availability of antibiotics and vaccines. Despite of effective antibiotics mortality due to meningitis is still significant. Mortality and morbidity increase with development of fatal complications. If the complications are picked up early on radiology and necessary management is started immediately deaths and permanent disability can be avoided with excellent survival outcomes.
References
-
Sharew A, Bodilsen J, Hansen BR, Nielsen H, Brandt CT (2020) The cause of death in bacterial meningitis. BMC Infect Dis 20(1): 182.
-
Vyas V, Kanagalingam G, Siddique Z (2020) Pneumococcal Meningitis Complicated by Subarachnoid Hemorrhage and Tonsillar Herniation. Cureus 12(8): e9994.
-
Julayanont P, Wang H, Laengvejkal P, Tantikittichaikul S, DeToledo J (2015) Subarachnoid hemorrhage: a rare complication of pyogenic bacterial meningitis (P6.312). Neurology 84(Suppl 14).
-
Matsumoto A, Mino S, Nishiyama T (2019) Intracranial Hemorrhage Caused by Bacterial Meningitis: Case Report and Review of the Literature. Asian J Neurosurg 14(1): 234-236.
-
Gerstein S, Gautam-Goyal P, Goyal S (2020) A case of Listeria monocytogenes meningitis complicated by Hydrocephalus and Intraventricular hemorrhage: A review of treatment options and outcomes 19: e00704.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey