Assessment of Fatty Liver Diseases Based on Serum Ck18 Fragment, Gamma Glutamyl Transferase and Aspartate Aminotransfease /Alanine Aminotransferase Ratio
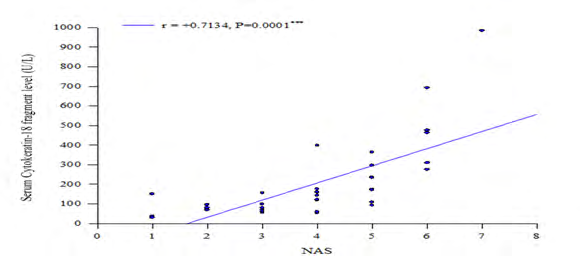
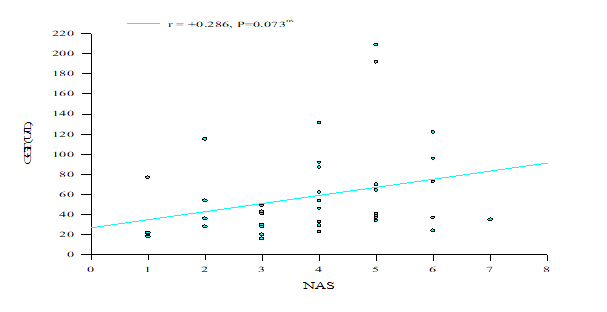
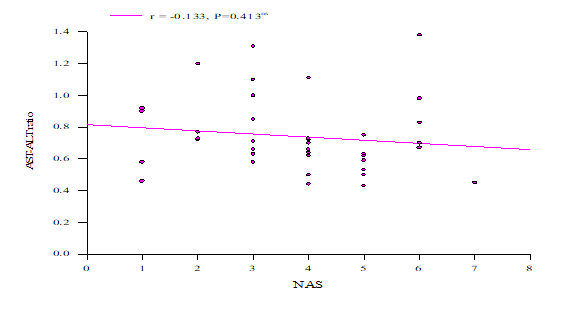
Background: Nonalcoholic fatty liver disease (NAFLD) is a serious clinical problem because of its worldwide distribution and potential adverse sequel. The global prevalence of NAFLD is increasing gradually. NAFLD can be estimated by both invasive and non-invasive methods. Objective: The aim of this study was to determine the role of serum cytokeratin-18 (CK-18) fragment, gamma glutamyl transferase (GGT) and aspartate aminotransfease (AST)/alanine aminotransferase (ALT) ratio (AAR) in the assessment of different types of NAFLD patients especially NASH. Methods: This cross sectional study was conducted in the Department of Clinical Pathology, Bangabandhu Sheikh Mujib Medical University. Forty patients who fulfilled the criteria of NAFLD were enrolled in this study. Serum CK-18 fragment level was measured by enzyme linked immune sorbent assay (ELISA) method. Serum gamma glutamyl transferase (GGT) and aspartate aminotransfease (AST)/alanine aminotransferase (ALT) ratio (AAR) reports were collected from patient’s file. Biopsy material was sent to the Department of Pathology, BSMMU for complete histopathological examination. Results: Positive and significant co-relation was found between serum CK-18 fragment with NAS whereas positive but not significant correlation was seen between serum GGT and NAS and negative and not significant correlation was found between serum (AAR) and NAS. Conclusion: Serum CK-18 fragment level may be used for assessing NASH in NAFLD patients.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is one of the common forms of chronic liver diseases. It is currently estimated that the global prevalence of NAFLD is one billion [1]. This prevalence is increasing gradually which will become the major economic burden [1]. In a study Nonalcoholic steatohepatitis (NASH) was observed in 42.4% of NAFLD cases in Bangladesh [2, 1]. Histologically nonalcoholic fatty liver disease is classified into nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH) [3]. Among them NASH may be present in one third of NAFLD [4]. Nonalcoholic steatohepatitis is a potentially serious condition [5]. The prevalence of NAFLD is 15% in Asian population and 20 to 30% in United States. It is thought to be the hepatic manifestation of metabolic syndrome [6]. The detection of CK18 fragment can differentiate NASH from NAFL or simple steatosis in this way [7].
Materials and Methods
The research protocol of this study was approved by the Ethical Institutional Review Board of BSMMU, Dhaka prior to the commencement of it. This cross sectional study was conducted in the Department of Clinical Pathology, in collaboration with Department of Hepatology and Department of Pathology, in Bangabandhu Sheikh Mujib Medical University, Dhaka from March’ 2014 to February’ 2015. 40 NAFLD patients of above 18 years old ages of both sexes who admitted in the Department of Hepatology were included in the study. Patients having history of alcoholism more than 210gm/wk for male and 140gm/wk for female, any condition like decompensated cirrhosis of liver, infected with hepatitis B and C virus infection, drug induced fatty liver, hepatocellular carcinoma, autoimmune liver diseases, hemochromatosis, wilson’s disease and patients with hypothyroidism were excluded from the study. Total NAFLD patients were divided into three groups according to the NAFLD activity score (NAS); NASH Clinical Research Network histological scoring system which is based on histopathological examination. After taking informed written consent, a careful history was taken and the detailed information was recorded by the investigator in a predesigned questionnaire [8].
The serum separation, storing and ELISA procedure were done in the Clinical Pathology Department, BSMMU. CK-18 fragment level is measured by Enzyme linked Immuno Sorbent Assay (ELISA) based on double antibody sandwich technology. Hematoxylin & Eosin and Masson’s Trichome stains were used and evaluated using NASH Clinical Research Network histological scoring system to diagnosis the NAFLD. All data were recorded systematically in a preformed data collection sheets and expressed as mean±SD. For all statistical tests we considered p value <0.05 as statistically significant. Statistical analyses of the results were obtained by Pearson’s correlation coefficient test. All statistical computations were performed by using window based computer software devised with Statistical Packages for Social Sciences (SPSS 17.0).
Results
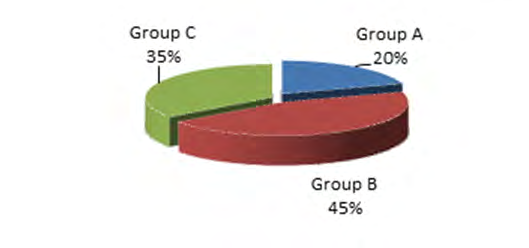
A total of 40 patients with NAFLD were included in this study. In this study, histopathology was considered as gold standard to divide the patients into 3 groups based on Nonalcoholic fatty liver disease activity score (NAS), including Group A : 1 to 2 = simple fatty liver disease; Group B: 3 or 4 = Borderline NASH Patients and Group C: 5 to 8 = Definite NASH.
| Group A No. (%) | Group B No. (%) | Group C No. (%) | p Value | |
|---|---|---|---|---|
| 26-40 | 4 (50.0) | 11 (61.1) | 7 (50.0) | 0.710ns |
| 41-50 | 2 (25.0) | 6 (33.3) | 5 (35.7) | 0.710ns |
| 51-60 | 2 (25.0) | 1 (5.6) | 2 (14.3) | 0.710ns |
| Total | 8 (20.0) | 18 (45.0) | 14 (35.0) | |
| Mean±SD | 42.63±10.07 | 40.06±7.88 | 0.492ns | |
| Range | 30.00-56.00 | 26.00-56.00 | 0.492ns | |
| Mean±SD | 42.63±10.07 | 43.43±8.97 | 0.836ns | |
| Range | 30.00-56.00 | 30.00-60.00 | 0.836ns | |
| Mean±SD | 40.06±7.88 | 43.43±8.97 | 0.285ns | |
| Range | 26.00-56.00 | 30.00-60.00 | 0.285ns |
Table 1: Age distribution of the study patients according to groups of nonalcoholic fatty liver disease (NAFLD) (n=40).
Chi-square test/ANOVA (PostHoc) test, ns= not significant Table 1: Age distribution of the study patients according to groups of nonalcoholic fatty liver disease (NAFLD) (n=40).
| Gender | Group A No. (%) | Group B No. (%) | Group C No. (%) | p Value |
|---|---|---|---|---|
| Male | 3 (37.5) | 4 (22.2) | 5 (35.7) | 0.622ns |
| Female | 5 (62.5) | 14 (77.8) | 9 (64.3) | |
| Total | 8 (20.0) | 18 (45.0) | 14 (35.0) |
Table 2: Gender distribution of the study patients according to groups of NAFLD (n=40).
Chi-square test, ns= not significant Table 2: Gender distribution of the study patients according to groups of NAFLD (n=40).
Discussion
This cross sectional study was conducted in the department of Clinical Pathology in collaboration with department of Hepatology, BSMMU, Dhaka. In this study, we investigated 40 NAFLD patients who fulfilled the inclusion criteria of the study. In this study, out of 40 patients of NAFLD, histopathological examination showed that 8 (20%) patients had simple fatty liver (Gr-A), 18 (45%) had borderline NASH (Gr-B) and 14 (35%) had NASH (Gr-C). Regarding the age, in this study, out of 40 patients, the mean (±SD) age of Group A (=simple fatty liver) patients was 42.63±10.07 (range 30-
56) years, Group B (= borderline diagnosis) was 40.06±7.88 (range 26-56) years and Group C (=NASH) was 43.43±8.97 (range 30-60) years. In this study, patients with NASH were found at 30-60 years age group. Alam, et al. mentioned that NASH affects the population with mean age 40±9.7 with range from 30-50 of Bangladesh. Aktas, et al. observed that the mean age of NAFLD patients was 47±12 (years) with range from 35-59 in his study [3]. Papatheodoridis, et al. showed that mean age of NASH patients in his study was 48±13 (35-61) [9]. Our study findings were similar with these studies [10]. Analysis of gender distribution showed out of 40 NAFLD patients 12 were male and 28 were females. Male female ratio was 1:2∙3. Out of 8 patients of Group A, 3(37.5%) were male and 5(62.5%) were female; out of 18 patients of Group B, 4(22.2%) were male and 14(77.8%) were female; and out of 14 Group C patients, 5(35.7%) were male and 9(64.3%) were female. In this study females were predominant among three Groups. Alam, et al. observed that female were predominant in NAFLD patients in Bangladesh. Aida, et al. also noticed female predominance in NAFLD patients in Japan [3].
Our study findings were consistent with these studies [11]. In this study, Pearson’s correlation-coefficient (r) test was performed to compare the relationship between the levels of CK-18 fragment with NAFLD Activity Score (NAS). We observed a positive correlation between GGT and NAS but not significant. Pearson’s correlation coefficient was +0.286, p>0.05. Feldstein, et al., Papatheodoridis, et al. and Grigorescu, et al. also found no significant correlation between GGT and NAS. So, our study was consistent with these studies [8, 10, 12]. In the present study, we found a negative correlation between AST-ALT ratio and NAS, not significant Pearson’s correlation coefficient was -0.133, (p>0.05). In the study Feldstein, et al. there was also no significant correlation found between AST-ALT ratio and NAS. This finding supported our study [8].
Conclusion
Our data revealed that there was statistically significant correlation between serum CK-18 fragments level with different types of NAFLD whereas, serum GGT and ALT- AST ratio were not significant statistically. In this aspect, we concluded that Serum CK-18 fragment level can be used for early detection; reduce progression, assessment of the prognosis of NASH in NAFLD patients.
Acknowledgement
Authors of this study are thankful to the authority of the Department of Hepatology, BSMMU, Department Pathology, BSMMU and the Department of Clinical Pathology, BSMMU, for their nice cooperation during sample collection, laboratory procedure and also thankful to the study subjects for their active and enthusiastic participation.
References
-
Perumpail BJ, Khan MA, Yoo ER, Cholankeril G, Kim D, et al. (2017) Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J Gastroenterology 23(47): 8263-8276.
-
Zhou JH, Cai JJ, She ZG, Li HL (2019) Noninvasive evaluation of nonalcoholic fatty liver disease: Current evidence and practice. World J Gastroenterology 25(11): 1307-1326.
-
Alam S, Noor-E-Alam S, Chowdhury ZR, Alam M, Kabir J (2013) Nonalcoholic steatohepatitis in nonalcoholic fatty liver disease patients of Bangladesh. World J Hepatology 5(5): 281-287.
-
Yilmaz Y, Dolar E, Ulukaya E, Akgoz S, Keskin M, et al. (2007) Soluble forms of extracellular cytokeratin 18 may differentiate simple steatosis from nonalcoholic steatohepatitis. World Journal of Gastroenterology 13(6): 837-844.
-
Athinarayanan S, Liu W (2012) Non-Alcoholic Fatty Liver Disease: Current Perspectives and Future Direction in Disease pathogenesis, Treatment and Diagnosis. Med chem 2: e104.
-
Fracanzani AL, Valenti L, Bugianesi E, Andreoletti M, Colli A, et al. (2008) Risk of Severe Liver Disease in Nonalcoholic Fatty Liver Disease with Normal Aminotransferase Levels: A Role for Insulin Resistance and Diabetes. Hepatology 48(3): 792-799.
-
Baršić N, Lerotić I, Duvnjak LS, Tomašić V, Duvnjak M (2012) Overview and developments in noninvasive diagnosis of nonalcoholic fatty liver disease. World J Gastroenterol 18(30): 3945-3954.
-
Feldstein A, Wieckowska A, Lopez R, Liu Y, Zein NN, Mc Cullough J (2009) Cytokeratin-18 Fragment Levels as Noninvasive Biomarkers for Nonalcoholic Steatohepatitis: A Multicenter Validation Study. Hepatology 50(4): 1074-1078.
-
Aktas G, Alcelik A, Tekce B, Savli H, Uyeturk U, et al. (2013) Mean Platelet Volume And Red Cell Distribution Width In Hepatosteatosis. National Journal of Medical Research 3(3): 264-266.
-
Papatheodoridis GV, Hadziyannis E, Tsochatzis E, Georgiou A, Kafiri G, et al. (2010) Serum apoptotic caspase activity in chronic hepatitis C and nonalcoholic Fatty liver disease. Journal of Clinical Gastroenterology 44(4): e87-95.
-
Aida Y, Abe H, Tomita Y, Nagano T, Seki N, et al. (2014) Serum cytokeratin 18 fragment level as a noninvasive biomarker for non-alcoholic fatty liver disease. Int J Clin Exp Med 7(11): 4191-4198.
-
Grigorescu M, Crisan D, Radu C, Grigorescu MD, Sparchez Z (2012) A Novel Pathophysiological-Based Panel of Biomarkers for the Diagnosis of Nonalcoholic Steatohepatitis. J Physiol Pharmacol 63(4): 347-353.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey