Intravitral Conbercept Injection as a Treatment for Tuberous Sclerosis Complex Retinal Astrocytic Hamartomas A Case Report
Purpose: This report describes our experience treating a patient exhibiting bilateral retinal Astrocytic Hamartomas (RAH) associated with vision loss and macular edema. This patient successfully and rapidly responded to the intravitreal injection of conbercept resulting in reductions in lesion sizes and corresponding improvements in visual acuity. Observation: A-22-year-old male patient that had received a diagnosis of tuberous sclerosis complex (TSC) presented with 1-week history of reduced vision and metamorphosia of the right eye as a consequence of RAH-associated macular edema. The patient underwent treatment in the form of two monthly intravitreal conbercept injections while this condition was in an early stage of progression. As of 6 six months following the start of these injections, monthly OCT imaging through the fovea continues to reveal the alleviation of the serous retinal detachment. These injections also resulted in stable reduction in RAH lesion sizes. Conclusion: Cases of RAH exhibiting clear FFA leakage and significant detachment in OCT imaging require appropriate and timely treatment. In this case, the patient achieved a best-corrected visual acuity of 0.8, presumably owing to the effective resolution of macular edema before substantial permanent damage had occurred. The intravitreal injection of anti-VEGF antibodies thus represents a promising means of treating macular edema and exudative retinal detachment secondary to RAH.
Introduction
Tuberous sclerosis complex (TSC) is an autosomal dominant genetic disease that results in the characteristic development of benign tumors known as hamartomas in the eyes, lungs and kidneys [1]. TSC affects approximately 1 in every 10000-16000 individuals and results from mutations in TSC1 or TSC2 genes respectively encoded on chromosome 9q34 and chromosome 16p13.3 [1, 2], with TSC2 mutations accounting for 75-80% of cases [3]. Retinal astrocytic hamartoma (RAH) formation is the most frequently detected ocular complication of TSC and serves as an important criterion for the diagnosis of this genetic disease [4], affecting roughly half of all TSC patients [5]. RAH cases are classified into three types based on fundus manifestations. Type I RAH lesions are generally circular, flat, semitransparent, light gray pattern, exhibit poorly defined margins, and are typically restricted to the retinal nerve fiber layer; In contrast, type II lesions are nodular and exhibit sharp demarcation, forming prominent mulberry-like masses containing various calcifications; Type III lesions exhibit a mixture of types I and II lesion features [3, 6]. While hamartomas are generally not progressive lesions, there have been reports of instances of progressive lesions associated with the subretinal fluid that can cause severe vision loss and metamorphopsia [3].
To date, no standardized treatments for RAH have been developed, with researchers having explored the clinical utility of mTOR inhibitor treatment [7], intravitreal anti- vascular endothelial growth factor(VEGF) injections [8], laser therapy [8], subthreshold micropulse laser photocoagulation [6], and photodynamic therapy [9]. In this report, we discuss the case of the successful use of intraviral conbercept as a treatment for a patient with RAH and macular edema.
Case Presentation
The 22-year-old male patient presented to the Lou Di Center Hospital complaining of a 1-week history of reduced vision and metamorphosia in the right eye. One month prior, he had been diagnosed with TSC, and underwent treatment to remove renal angiomyolipomas. He also exhibited clearly visible facial angiofibromas, shagreen patches on his lower back, fibrous growths around his toenails, hepatic angiomyolipoma formation, and multiple pulmonary micronodular. He was also found the harbor a pathogenic TSC2 mutation (NM_000548.5). During an initial ophthalmic examination, his best-corrected visual acuity (BCVA) in the right and left eye was 0.4 and 1.0 respectively. The ocular media and anterior segments of both eyes were unremarkable. Dilated fundus examination revealed multiple yellow-gray lesions from 1/2PD to 1PD in size in the peripheral retina of the left eye (Figure 1).
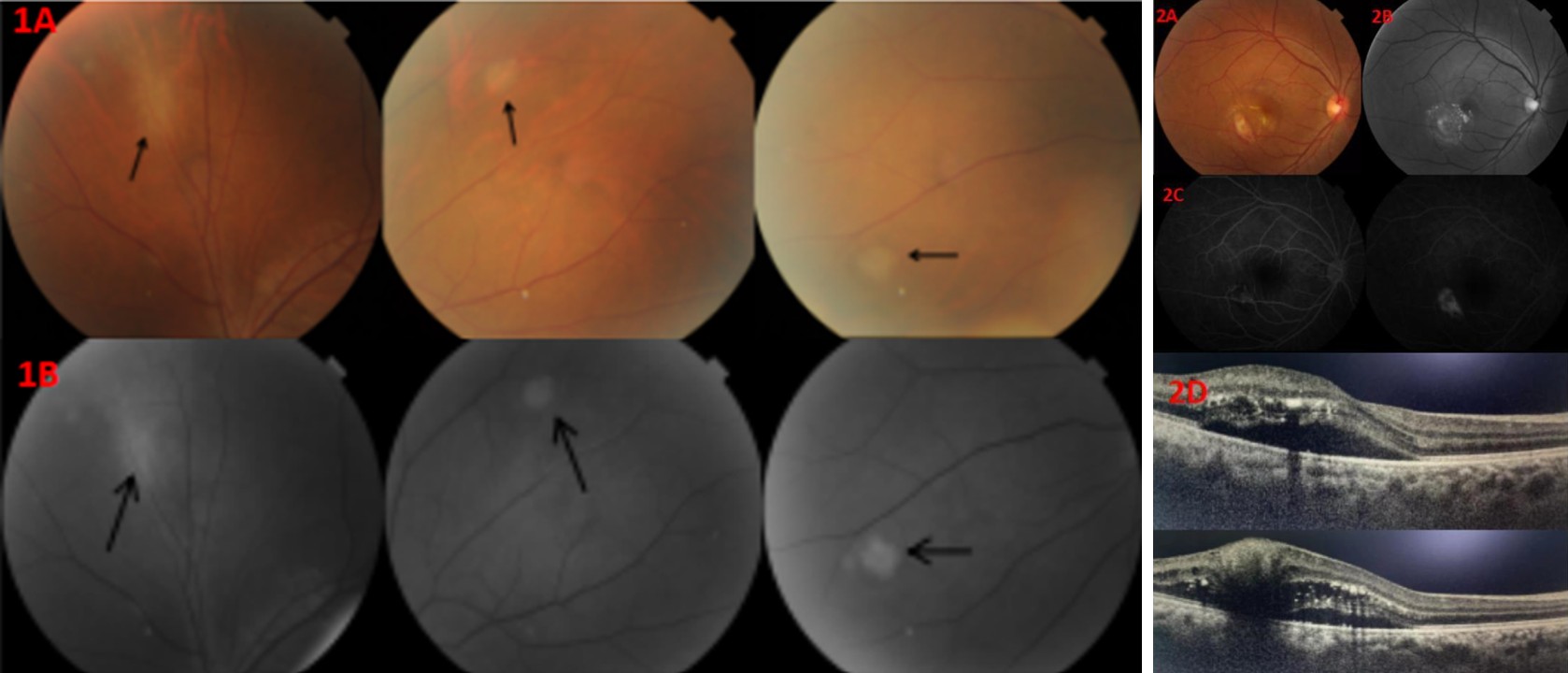
Figure 1A: Fundus images of the left eye, revealing flat, circular, semitransparent, light gray lesions with poorly defined margins(arrow). B. Fundus autofluorescence imaging revealing hyperautofluorescence.
While in the right eye, an elevated lesion was evidennt in the subtemporal of the fovea of the macula together with pronounced surface, neovascularization, macular edema, and exudate formation (Figure 2A). Fluorescein angiography(FFA) revealed pronounced leakage from these neovascular vessels (Figure 2C), while on optical coherence tomography(OCT) revealed that the lesion in the right eye was a hyper reflective mass associated with a disorganized retinal nerve fiber layer, posterior shadowing, sub retinal fluid, spaces with a ”moth-eaten” appearance, and multiple calcifications (Figure 2D). Based on these clinical and imaging findings the patient was diagnosed with bilateral RAH, and an Intravitral injection of Conbercept (0.5mg) was administered in the right eye.
Figure 2: Fundus images of the right eye prior to intravitreal conbercept injection. A: Fundus images revealed a prominent nodular lesion with some calcifications. B: Fundus autofluorescence imaging revealing hyperautofluorescence. C: FFA revealed hypofluorescencent occlusion during the early phase (left) and marked neovascular vessel leakage in the late phase. D: Horizontal OCT images through the fovea revealing macular edema (upper) with a dome-shaped hyperreflective mass associated with retinal disorganization, posterior shadowing, and “moth-eaten: spaces.
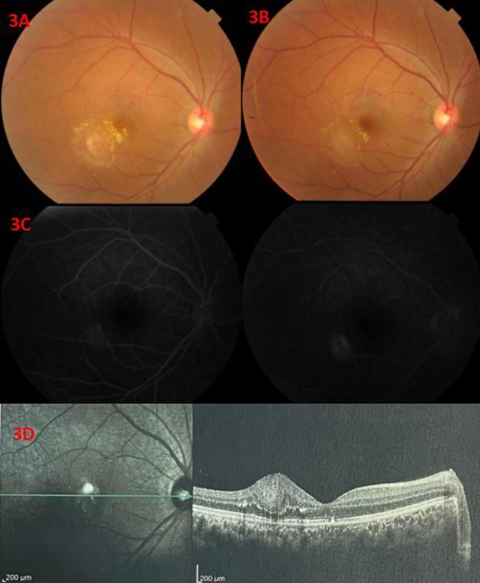
Figure 3: A-B. Fundus images of the right eye at 2 weeks (A) and 6 months (B) following the intravitreal administration of conbercept. Marked neovascular vessel regression was evident, together with the alleviation of macular edema and reductions in lesion size and exudate formation. C. FFA revealed a decrease in neovascular vessel leakage. D. OCT imaging revealed the absence of serous retinal detachment.
At 2 months post-conbercept treatment, the patient’s BCVA for his right eye had improved to 0.8, his metamorphopsia was alleviated, and clear neovascular regression, reduced macular edema, and a reduction in lesion size were all detected upon right fundus examination (Figure 3A-B). Consistently, FFA revealed a reduction in leakage from established neovascular vessels (Figure 3C), while OCT imaging indicated that serous retinal detachment was no longer evident (Figure 3D). Over the following 6-month follow-up period, the patient did not experience any macular edema recurrence and his BCVA remained at 0.8, while no significant changes in the lesions evident in the left eye were detected.
Discussion
RAH are a class of benign tumors frequently observed in patients diagnosed with TSC, as this genetic disease results in the formation of benign lesions in the eyes, skin, lungs, kidneys, and other tissue compartments. TSC results from mutations in the TSC1 or TSC2 genes, both of which are tumor suppressor proteins that encode hamartin and tuberin [10], which control the ability of cells to grow, proliferate, migrate, adhere, and differentiate [11]. TSC2 mutations account for 75-80% of all TSC cases [10], and the patient in the present case was found to harbor a pathogenic TSC2 mutation (NM_000548.5).
Three subtypes of RAH lesions have been described to date, and in the present case, the patient exhibited type I and type II RAH lesions in his left and right eyes, respectively. RAHs generally remain stable over time and have no significant impact on vision, although rare cases of aggressive lesions that resist treatment have been reported, potentially necessitating enucleation in cases of ocular pain and vision loss. In multiple reports, TSC-associated RAH lesions have been shown to be highly angiogenic and to express VEGF, with a reduction in lesion burden in response to anti-VEGF treatment [8]. Other approaches to treating these cases include PDT [9], conventional lasers [12], and sirolimus [7, 13]. The proximity of the target lesion to the macula in the present case resulted in the risks associated with PDT or conventional laser treatment being too severe. While oral mTOR inhibitor treatment has also been reported to reduce RAH size and exudate formation, this treatment approach was not recommended by our oncologists, and we therefore elected to employ a localized treatment approach in an effort to minimize the potential for systemic toxicity.
In the present case, following intravitreal conbercept injection (0.5 mg), pronounced improvements in BCVA, macular edema, symptomatic visual distortions, OCT, and FFA findings were rapidly observed with a concomitant reduction in the size of the lesion and associated neovascularization. These results were consistent with the expression of VEGF and its functional importance in retinal hamartomas, supporting a hypothesis through which the hypoxia-inducible factor-1α(HIF-1α)-VEGF axis is central to the TSC-associated development of this tumor type [14]. RAH-derived VEGF thus appears to play a key role in the pathogenesis of macular edema and exudative retinal detachment, in line with prior results [15].
Conclusion
The present case highlights the importance of timely and appropriate treatment in cases of RAH exhibiting pronounced FFA leakage and detachment detected via OCT. In this patient, the final BCVA achieved was 0.8, suggesting that the symptoms of macular edema largely resolved. The intravitreal administration of anti-VEGF can thus provide an effective means of treating macular edema and exudative retinal detachment that are secondary to RAH. It is therefore essential that TSC patients undergo routine annual ophthalmic examinations.
References
-
Pfirmann P, Combe C, Rigothier C (2021) Sclerose tubereuse de Bourneville: miseau point [Tuberous sclerosis complex: A review]. Rev Med Interne 42(10): 714-721.
-
Wan MJ, Chan KL, Jastrzembski BG, Ali A (2019) Neuro- ophthalmological manifestations of tuberous sclerosis: current perspectives. Eye Brain 11: 13-23.
-
Hodgson N, Kinori M, Goldbaum MH, Robbins SL (2017) Ophthalmic manifestations of tuberous sclerosis: a review. Clin Exp Ophthalmol 45(1): 81-86.
-
Northrup H, Aronow ME, Bebin EM, Bissler J, Darling TN, et al. (2021) Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations. Pediatr Neurol 123: 50-66.
-
Mishra C, Kannan NB, Ramasamy K, Balasubramanian DA (2019) Retinal Astrocytic Hamartoma in Tuberous Sclerosis. Indian Dermatol Online J 10(6): 753-754.
-
Yan S, Chen Y, Chen R, Tian B, Li Z (2018) Subthreshold micropulse laser photocoagulation therapy in a case of bilateral retinal astrocytic hamartomas with tuberous sclerosis complex: A case report. Medicine (Baltimore) 97(50): e13265.
-
Wu F, McGarrey MP, Geenen KR, Skalet AH, Guillot FH, et al. (2022) Treatment of Aggressive Retinal Astrocytic Hamartoma with Oral Mechanistic Target of Rapamycin Inhibition. Ophthalmol Retina 6(5): 411-420.
-
Allan KC, Hua HU, Singh AD, Yuan A (2022) Rapid symptomatic and structural improvement of a retinal astrocytic hamartoma in response to anti-VEGF therapy: A case report. Am J Ophthalmol Case Rep 27: 101606.
-
Eskelin S, Tommila P, Palosaari T, Kivela T (2008) Photodynamic therapy with verteporfin to induce regression of aggressive retinal astrocytomas. Acta Ophthalmol 86(7): 794-799.
-
Wang X, Wang W, Zhao Y, Wang Z, Zhang Y (2022) Analysis of Clinical Features and Next-Generation Sequencing of 12 Tuberous Sclerosis Families in China. Front Med (Lausanne) 9: 840709.
-
Rosset C, Netto CBO, Ashton PP (2017) TSC1 and TSC2 gene mutations and their implications for treatment in Tuberous Sclerosis Complex: a review. Genet Mol Biol 40(1): 69-79.
-
Vrabec TR, Augsburger JJ (2003) Exudative retinal detachment due to small noncalcified retinal astrocytic hamartoma. Am J Ophthalmol 136(5): 952-954.
-
Zhang ZQ, Shen C, Long Q, Yang ZK, Dai RP, et al. (2015) Sirolimus for Retinal Astrocytic Hamartoma Associated with Tuberous Sclerosis Complex. Ophthalmology 122(9): 1947-1949.
-
Brugarolas JB, Vazquez F, Reddy A, Sellers WR, Kaelin WG Jr (2003) TSC2 regulates VEGF through mTOR- dependent and -independent pathways. Cancer Cell 4(2): 147-158.
-
Ahmad KT, Mansour HA, Rollins BT, Oviedo SP, Phillips PH, et al. (2021) Long Term Outcome and Histologic Findings of a Retinal Astrocytic Hamartoma Treated with Intravitreal Injection of Anti-VEGF: A Case Report. Case Rep Ophthalmol Med 2021: 7500791.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey