Comparative Analytic Epidemiology of Plasmodium Parasitized Pregnant and Non-Pregnant Women Attending Tertiary Health Care Facility in Port Harcourt, Niger Delta
Malaria remains a public health burden in Nigeria. This study compared and determined the prevalence of malaria parasites and other possible risk factors among pregnant and non-pregnant women in Port Harcourt. A total of 200 blood samples (capillary) were collected from 100 pregnant and 100 non-pregnant women as a control through convenience sampling technique research design. The subjects for the study were drawn from women attending antenatal clinic in Braithwaite Memorial Hospital Port Harcourt, Rivers State, Nigeria. Thick and thin films were made on clean grease free glass slide and stained after drying with 3% solution of Giemsa stain to detect and identify the species of malaria parasites. SPSS version 21 was used to estimate frequency and percentage outcome. The results showed that out of 100 slides examined for pregnant women, 68% had malaria infection while 32% were negative. There were high prevalence rate of malaria infection among pregnant women of 20-23 years and 32-35 years age group while those ≥ 40 years showed least rate of 33%. The control samples showed infection rate of 71% with 29% negative. Showing that, non-pregnant women have a high prevalence rate when compared to pregnant women. It was discovered that illiterate pregnant women showed high prevalence rate than their educated counterparts. The use of indigenous (drug) herbs by some pregnant women proved 100% sensitive to P. falciparum as none were positive for malaria infection as captured through the administration of well-structured questionnaire. Intermittent treatment is therefore, recommended and further robust research should be channelled towards indigenous (drug) herbs for malaria treatment, especially in the developing communities. There is also urgent need for more inclusive malaria public health education in the region, especially among the vulnerable groups.
Introduction
Malaria is a life-threatening parasitic disease which constitutes major problem to pregnant women in tropical countries like Nigeria. Changes during pregnancy and the presence of placenta organ-malaria parasites affinity alter the immune status in women. These phenomenal changes further diminish the immunity of pregnant women thereby making them more vulnerable to malaria infection. It has been earlier reported that annually, 25 to 30 million women become pregnant in malarious areas of Africa [1]. Malaria infection during pregnancy can have adverse effects on mother and foetus, including maternal anaemia, foetal loss, premature delivery, intrauterine growth retardation, and delivery of low birth-weight infants, a risk factor for death [2, 3]. The burden of malaria infection during pregnancy is caused mainly by P. falcjparum malaria parasites, the most common malaria species in Africa.
Research has shown that adverse effects of malaria in pregnancy vary by areas of high and low transmission levels. Pregnant women living in low transmission settings infected with malaria may experience severe malaria disease, maternal anaemia, premature delivery, or foetal loss [3]. In high transmission areas, there is significant development of group immunity that prevents severe disease, however, Plasmodium parasites specifically target the placenta, leading in increased risk during pregnancy. Pregnant women infected with malaria parasites in such settings are more likely to experience maternal anaemia, and delivery of low birth-weight infants, particularly for categories such as the immunocompromised, younger women, and those in their first and second pregnancies [3]. Therefore, pregnant women like other critically vulnerable groups such as infants and children under 5 years of age, naive adults, are more prone to malaria infection in endemic settings than non- pregnant women [4, 5, 6]. It was earlier reported that about 10,000 maternal deaths are attributed to malaria annually [7]. In Nigeria, 11% of maternal deaths are attributed to malaria [8].
Many researchers have reported different prevalence rates of malaria in pregnancy in different parts of Nigeria, ranging from 19.7% to 72.0% [9]. In Anambra, Southeastern Nigeria, Ukibe SN, et al. [10] reported a prevalence of 73.1% of Plasmodium falciparum infection among pregnant women. In another related recent study conducted on pregnant women in Rivers State, an overall prevalence of 31.3% was reported Wokem GN, et al. [11]. While there are reports of up to 50% reduction in malaria episodes and deaths in some African countries between 2000 and 2006, report from Nigeria has not shown significant reduction, especially with regards to malaria in pregnancy.
Malaria in pregnancy is a obstetric, social and medical problem requiring multidisciplinary and multidimensional clinical approach to handle. Preventing malaria in pregnancy relies on insecticide treated bed nets, intermittent preventive treatment with antimalarials such as sulphadoxine- pyrimethamine, and potentially relies on the development of effective vaccines. Pregnant women are routinely given folic acid supplementation to prevent neural tube defects in their infants. However, high doses of folic acid counteract the effect of sulfadoxine-pyrimethamine [3].
With all the above complications associated with malaria parasites infections in human, the occurrence of malaria infection in pregnant women of various age groups was studied to know the current distribution of malaria parasites among this vulnerable group, pregnant women. Also, this study related peoples’ ways of life as regards to age, educational status, and social behaviour as these affect exposure to malaria parasitic infection. This study, therefore, was aimed to compare and determine the prevalence of malaria parasites in pregnant and non-pregnant women in relation to certain epidemiological factors such as age, educational status, and social behaviour.
Materials and Methods
This was hospital-based cross-sectional research on the distribution of malaria parasites among pregnant women attending antennal care in Braithwaite Memorial Hospital Port Harcourt, Rivers State, Nigeria. Braithwaite Memorial Hospital Port Harcourt is a tertiary hospital that serves as referral centre. It is the second largest tertiary hospital in Rivers State, Nigeria. It is locate in the heart of Port Harcourt city. It is a government owned health care facility with different department and team of specialists and consultants with very large bed capacity. The city where it is situated – Port Harcourt, is a metropolitan city with lots of oil and gas activities with influx of human in bid to make a living. The seasons common are the rainy and dry seasons however, the rainy is more. This study was conducted during the rainy season. The geographical situation of the study area actually favours the breeding of vectors including female Anopheles mosquitoes. A total of 200 participants were randomly selected and recruited into the study, 100 each per group of pregnant women and a non-pregnant comparing group. The groups were matched with respect to sex, age, occupation and drug used. Laboratory diagnosis involved microscopic examination of both thick and thin blood films for the diagnosis of malaria parasites according to Cheesbrough M [12]. Quality control measures were applied as the study utilized both negative and positive controls in the study. Consent and approval were not taken for granted in course of the study as well as other ethical issues.
Data was presented using descriptive statistics in frequencies and percentages, and analysis was done using excel and SPSS version 21 software.
Results
The study recruited two hundred (200) women classified based on gravid status as pregnant and non-pregnant in an equal proportion each of one hundred per stratum. The malaria parasite species detected and identified in this study was Plasmodium falciparum only.
Overall Prevalence of Plasmodium Parasitaemia
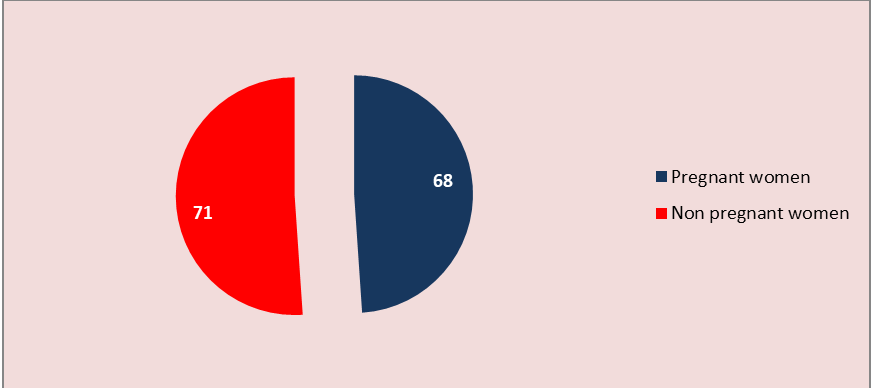
Figure 1 shows the distribution of malaria parasites among pregnant and non-pregnant women. Of the 100 samples of the pregnant women examined, the prevalence of malaria parasites in percentage was 68.0% while the non-pregnant women had a prevalence rate of 71.0%. The observed difference in prevalence rates showed that more of non-pregnant women were infected than pregnant women.
Age-Related Distribution of Plasmodium Parasitized Pregnant Women
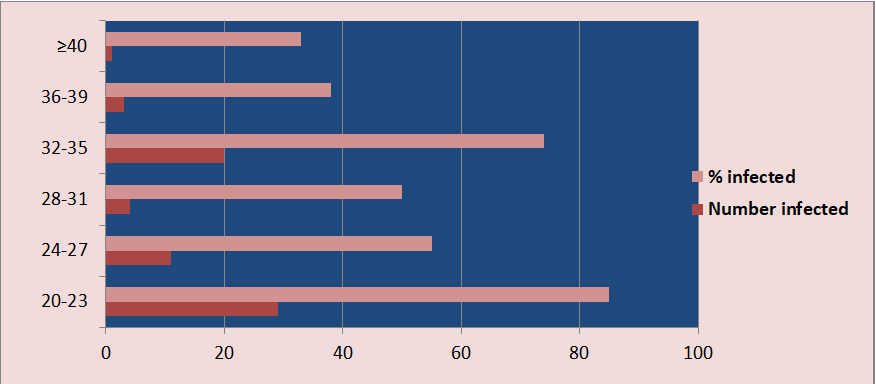
Figure 2 shows the distribution of malaria parasites in pregnant women according to age group. Pregnant women within the age range of 20 to 23 years recorded the highest percentage of malaria infection, followed with those within the age range of 32 to 35 years, while those who were 40 years or above had the lowest percentage prevalence of malaria infection, followed with those within the age range of 36 to 39 years respectively.
Distribution of Plasmodium Parasitized Subjects by Educational Status
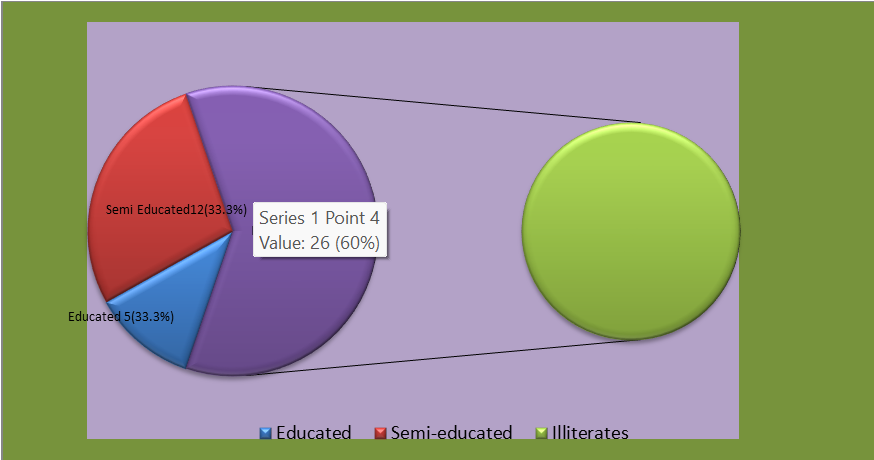
Figure 3 shows that, illiterate pregnant women had the highest percentage of prevalence, 26 (53.1%) while educated and semi educated pregnant women had similar prevalence rate of 33.3% at varying frequencies of 5 and 12 respectively.
Distribution of Plasmodium Parasitized Subjects Based on Drug used Status
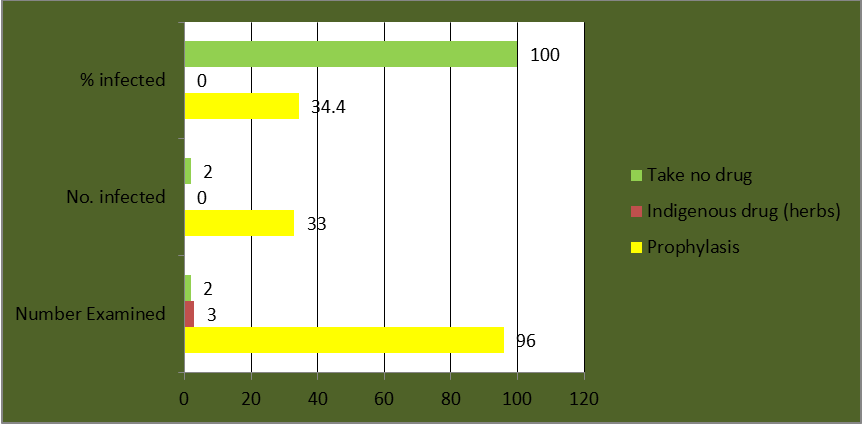
Figure 4 shows percentages of infected pregnant women based on drug used. Three (3) pregnant women that used indigenous drugs (herbs) showed 0% infection rate while 96 pregnant women that used prophylaxis had 33 of them infected with a prevalence of 34.4%. And those who used no drugs had all of them infected with a prevalence of 100%.
Discussion
Pregnant women are more susceptible to infection with malaria parasites, Plasmodium falciparum which is more threatening during pregnancy. Pregnancy appears to interfere with immune processes in malaria a disease which alters immune reactivity. In higher malaria endemic area where semi-immune adults usually have substantially acquired resistance to local strains of plasmodia, prevalence of clinical malaria is higher and it’s severity greater in pregnant women than non-pregnant women [13]. This is not consistent with the finding from this study in which the prevalence rate of 68% of malaria parasite infection was recorded in pregnant women while non-pregnant women had higher prevalence of 71%. Reasons for this result, perhaps the pregnant women were usually given prophylactic antimalarial drugs which protect them from malaria. This may also be due to the fact that, the study was carried out during rainy season, April to June.
Researchers in similar studies on malaria in pregnancy had reported variations in Plasmodium parasites infection rates in different geographical locations in Nigeria. In 2011 and 2017, a low prevalence rate of 26% and 31.3% respectively of malaria parasites were reported among pregnant women in Rivers State [11, 14]. While in another related study conducted among pregnant women in Calabar, Southern Nigeria, a prevalence of 68% of Plasmodium falciparum infection was reported Monjol BE, et al. [15], which strongly corroborates the findings of this study. However, a higher prevalence rate of 73.1% [10] and 99% Gunn JKL, et al. [16] were reported among pregnant women in Anambra and Enugu, South eastern Nigeria respectively. These changes in rates of prevalence may be attributed to differences in level of transmission or endemicity of malaria parasites at the various study locations, differences in sample size, gravidae status of pregnancy of participants, responsiveness of participants to malaria prophylactic measures, and malaria microscopic skills of researchers.
Age distribution of malaria parasitaemia in this study showed that infected pregnant women within the age limits of 20-23 years and 32-35 years had the highest rates of prevalence. This is consistent with the reports of similar studies conducted in Rivers State by Barikuura FB, et al. [5], and in Gabon Republic by Bouyou-Akotet Mk, et al. [17] who found that pregnant women within the age group less than 21years and greater than 32 years were at high risk. These age limits could depict younger women, primigravidaes, which are highly susceptible to infection and most affected with malaria parasites infection outcomes than their older counterparts. Therefore, to stem this, awareness on malaria preventive measures during their pregnancy should target young women even before they get married preferably at schools, religious, and social gatherings.
It was further observed in this study that illiterate pregnant women had the highest prevalence of 53.1% of malaria parasites compared with their educated counterparts. This is probably attributed to frequent exposure to vectors of malaria parasites due to low knowledge of malaria pathogen transmission and breeding pathways. This further validates the fact that a relationship exist between poverty, illiteracy and malaria infection. Notably according to Schantz-Dunn J [18], World Health Organization previously defined malaria as a disease of poverty caused by poverty.
On the contrary from this study, educated pregnant women recorded low infection rate of 33.3%. This could be due to their high living standard, awareness, and high knowledge on preventive measures against both malaria infectious agents and arthropod vectors of transmission.
Furthermore it was also found in this study that pregnant women who refused to take drugs due to their religious belief or inability to adhere to the Doctor’s instructions on malaria chemoprophylaxis had the highest prevalence rate of 100%, followed by those on prophylaxis 34.4%, while those who took herbs (indigenous drug) had no malaria attack.
The rate of malaria infection obtained in this study is high for both the pregnant and non-pregnant women and the underlying clinical state of these study participants may not have been considered especially the pregnant women. The pregnant women and the foetus in-utero are at higher risk to the adverse effects of malaria infection. Malaria and pregnancy are mutually aggravating conditions. The physiological changes of pregnancy and the pathological changes due to malaria have synergistic outcome on the course of each other, thus making the life difficult for the mother, the child and the treating physician. P. falciparum malaria can run a turbulent and dramatic course in pregnant women.
Moreover, in pregnancy malaria tend to be more atypical in presentation. This could be due to the hormonal, immunological and haematological changes of pregnancy. Malaria in pregnancy is more severe due to the hormonal and immunological changes, the parasitaemia tends to be 10 times more severe and as a result, all the complications of falciparum malaria are more common in pregnancy compared to the non-pregnant population. Plasmodium falciparum is more fatal in pregnancy because its mortality doubles compared to the non-pregnant population.
The challenge of malaria is an increasing concern for public health professionals especially the high incidence plus wide spread among the vulnerable groups. Despite efforts to reduce transmission and increase treatment, there has been little change in which areas are at risk of this disease since 1992. Indeed, if the prevalence of malaria stays on its present upwards course, the death rate could double in the next twenty years. Precise statistics are unknown because many cases occur in rural areas where people do not have access to hospitals or the means to afford health care. As a consequence, the majority of cases are undocumented.
In Africa malaria is present in both rural and urban areas, though the risk is lower in the larger cities [19].
Conclusion
This study found a higher prevalence of malaria parasites in non-pregnant women than pregnant women. The rate of clinical malaria is higher and its severity greater in pregnant women than non-pregnant women. Thus P. falciparum infection during pregnancy increases the likelihood of maternal anaemia, stillbirth, low birth weight, decrease haemoglobin concentration to mention but a few. Hence, the urgent need to intensify vector and parasites control through health education campaign among the populace, use of chemo- and prophylactic drugs, along with the use of long lasting insecticide treated nets against the vectors.
Recommendation
Intermittent treatment with curative anti-malaria drug should be administered at least twice during pregnancy (second and third trimesters) in order to reduce the incidence of low birth weight and anaemia following Kindhauser MK [20] guideline.
The use of herbs by some pregnant women proved effective. Hence government should encourage ministry of health and NAFDAC and local herbs producers to go into more research in local herb just to develop new and more effective drugs for preventing and control, particularly in view of the rapid spread of drug resistance.
Young women between the ages of 20 and 23 of years recorded the highest prevalence hence awareness on malaria prevention should target young women even before they get married preferably at schools, religious and social gathering. This is done by raising high living standard, awareness, and preventive measures towards material infection and their vectors. These measures when taken would dramatically reduce the burden of infection of parasitaemia and definitely reduced the malaria parasite count in the blood.
The most ultimate goal of malaria control is to prevent mortality and reduce socio-economic loss by reducing morbidity through progressive improvement, regular chemoprophylaxis where necessary, combination with standard treatment should be recommended for travellers.
The use of insecticide treated nets decreased both the number of malaria cases and malaria death rates in pregnant women (World Health Organization). It is also essential to avoid stagnant pools and poor environmental condition, which encourages the breeding of mosquito. Nevertheless, much work need to be done to educate the pregnant women and the producer of indigenous drug (herbs) to strictly adhere to environmental hygiene since no single women took herb had malaria parasites in the blood.
- Acknowledgement: We are sincerely grateful to the pregnant and non-pregnant women who willingly participated in this study, even as we are also thankful to the Medical Microbiology of Braithwaite Memorial Hospital Port for their technical support during laboratory practical assay of the samples of this study
- Ethical Approval: Ethical approval was gotten from the ethical approval committee of the facility where the study was conducted.
References
-
Steketee RW, Nahlen BL, Parise ME, Menendez C (2001) the burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg, 64(2): 28-35.
-
Azuonwu O, Amadi EC, Wokem GN, Kalu NE (2011) Health risk of malaria infection during pregnancy: A review. Journal of Pharmacy Research 4(1): 30-32.
-
Centers for Disease Control and Prevention (2023) Intermittent Preventive Treatment of Malaria for pregnant women (IPTp).
-
Azuonwu O, Wokem GN, Dimkpa FB (2019) Differential molecular investigation assay of tumor necrosis factor- alpha (TNF-α), interleukin-1 beta (IL-1β), Interleukin-6 (IL-6), and interleukin 10 (IL-10) among children potentially diagnosed of falciparum-malaria of Niger Delta extract. LOJMS 4(2): 358-363.
-
Barikuura FB, Ngozika WG, Obioma A (2019) Immune- based investigation of tumour necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), interleukin-6 (IL- 6), interleukin-10 (IL-10) among pregnant women infested with Plasmodium falciparum in Port Harcourt. J Medical Microbio Immunol Res 3(1): 1-9.
-
Doolan DL, Dobano C, Baird JK (2009) Acquired immunity to malaria. Clin Microbiol Rev 22(1): 13-36.
-
Okpere EE, Enabudoso EJ, Osemwenkha AP (2010) Malaria in pregnancy. NMJ 51(3): 109-113.
-
Federal Ministry of Health (2000) Malaria Situation Analysis Document Federal Ministry of Health Report.
-
Okwa OO (2003) The Status of malaria among pregnant women: A study in Lagos, Nigeria. Afr J Reprod Health 7(3): 77-83.
-
Ukibe SN, Ukibe NR, Mbanugo JI, Ikeakor LC (2016) Prevalence of malaria among pregnant women attending antenatal clinics in hospitals in Anambra State, South east, Nigeria. AJOL 37(2): 240-244.
-
Wokem GN, Amala SE (2017) Prevalence of malaria in pregnant women attending antenatal clinic in a rural and an urban hospital in Port Harcourt, Nigeria. JAMMR 24(12): 1-9.
-
Cheesbrough M (2005) District laboratory practice in tropical countries, Part 1 2nd (Edn.), Cambridge University Press.
-
Uko EK, Emeribe AO, Ejezie GC (1998) Malaria infection of the placenta and Neonatal low birth weight in Calabar. Journal of Medical Laboratory Science 7: 7-10.
-
Wogu MN, Nduka FO, Wogu MD (2011) Prevalence of malaria parasite infection among pregnant women attending antenatal clinics in Port Harcourt, Rivers State, Nigeria. IJTDH 3(2): 126-132.
-
Monjol BE Useh MF (2017) Detection of Plasmodium falciparum chloroquine resistance transporter (pfCRT) mutant gene amongst malaria-infected pregnant women in Calabar, Nigeria. Ann Parasitol 63 (4): 323-330.
-
Gunn JKL, Ehiri JE, Jacobs ET, Ernst KC, Pettygrove S, et al. (2015) Population-based prevalence of malaria among pregnant in Enugu State, Nigeria; the healthy beginning initiative. Malaria Journal 14(1): 438.
-
Bouyou-Akotet MK, Ionete-Collard DE, Mabika- Manfoumbi M, Kendjo E, Matsiegui P, et al. (2003) Prevalence of Plasmodium falciparum infection in pregnant women in Gabon. Malaria Journal (2): 18.
-
Schantz-Dunn J, Nour NM (2009) Malaria and pregnancy: A global health perspective. Rev Obstet Gynaecol 2(3): 186-192.
-
Keiser J, Utzinger J, Caldas De Castro M, Smith T, Tanner M, et al. (2004). Urbanization in Sub-Saharan Africa and Implication for Malaria Control. Am J Trop Med Hyg 71(2): 118-127.
-
Kindhauser MK (2003) Communicable diseases 2002: Global defence against the infectious disease threat / edited by Mary Kay Kindhauser. WHO.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey