Prevention of Pressure Sore Using Silicone Gel Pad in Prolonged Surgery
Pressure ulcers develop primarily from friction and shear and are progressive. It is usually found in bedridden and immobile people. Spinal cord injury patients have loss of sensation which adds to the problem. Patients with stroke, who have undergone long surgery, long bone fracture, not able to move tend to develop a pressure sore. Pressure ulcers are preventable usually and their management depends on their severity. This article discusses the prevention of pressure sore by using silicone gel pad in operation theatre that is undergoing prolonged surgery
Introduction
An intraoperative pressure ulcer is a pressure ulcer that develops from hours to 6 days postoperatively. Pressure sore in operating patients is a well-missed complication in surgical departments. Compared to inpatient pressure ulcers, which occur at a rate of 1-11%, intraoperative pressure ulcers occur at a higher rate of 4.7-66% [1]. Long surgeries that last for hours can cause pressure sores which are preventable but unnoticed by the surgical team. Pressure ulcer formation is highly influenced by risk factors, including all conditions leading to immobility, decreased or lack of sensation, as well as malnutrition. Extrinsic risk factors include being immobilized on a spinal board, table, or bed for prolonged periods, as well as poorly fitted medical devices in contact with patient tissues. Intrinsic risk factors such as diabetes, malnutrition, and smoking also increase the overall risk for pressure ulcers. The spinal cord injury patient population is at the highest risk (25-66%) of developing a pressure ulcer due to the combination of immobility and decreased sensation. These data highlight how critical the need is to understand the physical, environmental, and medical risks of the development of pressure ulcers in the individual patient to prevent them.
Materials and Methods
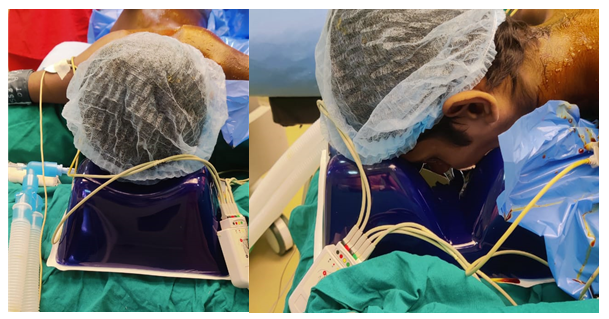
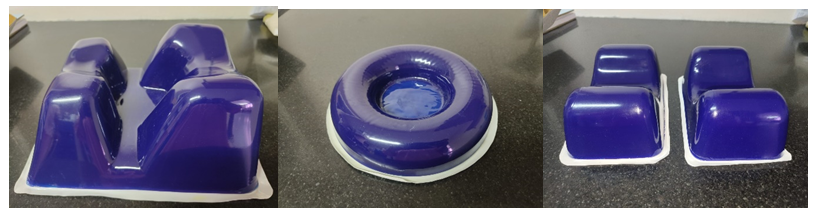
This study was conducted in the Department of Plastic Surgery at a tertiary care center in South India after getting the departmental ethical committee approval. Informed written consent was taken. The study was done on multiple patients who are undergoing prolonged surgeries like free flaps, and craniofacial surgeries. Patients were positioned in a supine or prone position (Figure 1-3). The silicone gel pads (Figure 4) were placed under the pressure points such as the heel, forehead, and occiput. One patient underwent Latissimus dorsi free flap for leg defect which took 270minutes. The second patient underwent Anterolateral Thigh flap cover for foot defect. It was completed in 300minutes. The third patient underwent brachial plexus exploration and nerve transfer which was completed in 240minutes. The silicone gel pad was utilized during the entire duration of the procedure. Patients
were followed up regularly in postoperative period for development of skin changes and pressure sore development.


Results
The studies on using the silicone gel pad for the prevention of pressure sores are showing good outcomes. This study was very promising when it comes to the prevention of pressure sore while patients undergoing prolonged surgeries.
Discussion
Prevention of pressure ulcer formation is directed at alleviating the risk factors for the individual patient, and is primarily focused on minimizing episodes of prolonged pressure either by placing appropriate padding at pressure points or by frequent patient repositioning. Even with adequate padding [2], it is important to make routine positional changes as even relatively low pressures can cause a pressure ulcer with prolonged exposure. Pressure mapping technologies have been developed to measure the amount of pressure placed on different parts of the sitting supine or reclining body. These technologies have been used to develop pressure-relieving wheelchair cushions and to study normal weight-shifting behavior.
Their use in bed-bound patients has been limited but has great potential for determining pressure points at risk for ulceration and in determining the effect of pressure-relieving positions on established wounds [3]. Any patient who has been determined to be at risk for development of a pressure ulcer or who already has a pressure ulcer needs to have a plan for repositioning. The plan needs to be individually tailored for each patient to address his or her specific needs. Frequency of repositioning needs to take many factors into account, including the support surface for the patient, general medical condition, and goals of care. Clinicians need to be cognizant of the fact that repositioning itself, can create shear forces on skin, and so, the fragility and condition of the patient’s skin need to be part of the assessment for how frequently to reposition them [4].
There are a variety of factors to take into account for how to reposition patients depending on whether the patient is supine, prone, or in a wheelchair of special note for patients in the acute hospital setting are medical devices. Care
must be taken in intraoperative positioning of the device between the patient and the support surface can create a high-pressure zone. Documentation of positioning and repositioning and regular skin condition assessment is the key in determining early signs of pressure ulcer formation such as non-blanching erythema [5]. It is necessary in prolonged surgeries to ascertain that the pressure points are adequately padded. However, the limitation is the inability to frequently reposition during a surgical procedure.
A variety of pads are available, which are designed to specifically cover pressure points such as the sacrum and heels as well as foam pads designed to wrap around body parts at risk (especially feet). However, it is important to note that some pads can be detrimental. For example, supports with cutouts can have increased pressure at their edges. There are an equal number of mattress pads (egg crate mattresses, natural sheepskins, etc.) that serve to decrease pressure across a large surface area. Silk-based fabrics are superior in pressure ulcer prevention when compared to cotton-based fabrics due to a decrease in friction forces and subsequent damage to the skin. It is common for patients to develop grade 1 pressure ulcers at pressure sites during the immediate postoperative period, due to their intraoperative position [6].
Normally intracapillary pressure at the arterial end is 30-40mmHg [7]. Microcirculatory occlusion occurs beyond this pressure and this, in turn, initiates a downward spiral toward ischemia, tissue death, and ulceration [8, 9].
The standard operating table mattress is usually made of two-inch (5.08cm) elastic foam and covered with vinyl fabric. However there is evidence that this type of surface contributes to the development of pressure sore. On the other hand, mattresses made with high-specification foam can reduce the formation of pressure sore. The under layer of the mattress allows the patient to sink in and wrap around the body, increasing contact area by up to 60% due to its multi-layer smooth surfaces. Such properties help to distribute pressure over a larger area. Bi-elastic layers also reduce skin creases and shear forces [10].
Identifying pressure injuries as related to surgery can be challenging. They do not manifest in the immediate postoperative period, and their presence must be anticipated. If a patient develops pressure sore, care providers must retrospectively evaluate preoperative period of 24 to 72hours for likely contributing factors. Such a period of confinement may include an acute period of immobility at home due to trauma or unconsciousness, a prolonged period of immobility related to the change in health status, loss of a caregiver, a prolonged emergency department stay, and testing or treatment requiring sedation or immobilization (such as cardiac catheterization, MRI) [11].
The goal of preventing pressure ulcer is to reduce the risk problems of the patient, focusing mainly on reducing the incidence of pressure ulcer by placing appropriate fillings in high points or changing the patient’s position frequently. Even if there is sufficient padding, it is important to change position regularly, even if the pressure is low, it can cause pressure sores due to long-term exposure. Measuring machines are designed to measure the pressure of different parts of the body while lying on your back or sleeping. These ideas were used to create a high chair and study weight- bearing behavior.
Their use in ambulatory patients is limited, but they have great potential in identifying high-risk points for ulceration and determining the effect of pressure-relieving postures [3]. All patients who are at risk of developing pressure ulcer or who already have pressure ulcer need to develop a rehabilitation plan. The plan should be individualized to meet each patient’s unique needs. Many factors must be considered in changing frequency, including the patient’s supportive environment, general medical condition, and goals of care. Physicians should be aware that changes in themselves can create shear forces in the skin, and therefore fragility and pain in the patient’s skin should be part of the process of evaluating the frequency of repositioning [4].
When it comes to how to change, the patient must consider many factors. Depending on whether the patient is asleep, awake, or in a wheelchair. Special warnings for intensive care patients are medical equipment. Care should be taken when placing the device between the patient and the support surface as a pressure point may occur. Information about the location, reoperation, and regular evaluation of skin inflammation is important to identify early signs of inflammation, such as non-blanching erythema. When the surgery is interrupted, it must be determined whether the high points are sufficient. However, its limitation is that it cannot be adjusted frequently during surgery.
In addition to many bandages specifically designed to cover high points such as the ankles and feet, there are also bandages designed to cover the body at risk (especially excluding the feet). However, it is worth noting that some bandages may cause problems. For example, during the cutting process, the pressure on the edges of the support may increase. Normally, intracapillary pressure at the ends of blood vessels is 30 to 40mmHg. Above this pressure, microcirculatory obstruction occurs, causing a vicious cycle of ischemia, tissue death, and ulceration [8, 9].
The bed mattress is usually made of two inches (5.08cm) of elastic foam covered with plastic. But there is evidence that such a site can lead to the development of pressure ulcer. On the other hand, mattresses made of high-measurement sponge can reduce the formation of pressure sores. Due to its multi-layered structure, the lower layer of the bed increases the contact area by up to 60%, allowing the patient to enter and hug the body. This product helps divide the height into a larger area. The bielastic layer also reduces skin wrinkles and cut fat [10]. Surgery related liver damage can be difficult to assess. They do not appear immediately after surgery, so their presence must be taken into account. If the patient develops a mental condition, caregivers should reevaluate the effectiveness of the medication 24 to 72hours before surgery. Incarceration periods, short term absences due to injury or illness, long-term absences due to changes in health, loss of caregivers, extended stays in the emergency room, and tests or treatments requiring sedation or immobilization (e.g., cardiac arrest, Catheterization, MRI) [17].
Silicone gel pads are a novel technique that helps in maintaining the capillary blood flow and does not cause ischemia of the pressure points. Silicone gel will maintain the capillary pressure (16mmHg to 32mmHg) which is well below the threshold pressure to cause pressure ulceration. Silicone Gel is covered with Ctu film to prevent damage to the silicone gel inside. It is comparatively easy to clean wipe with a solvent like sanitizer [12, 13, 14, 15, 16, 17].
Conclusion
It’s important to note that prevention is the key in managing pressure sores. Intraoperative pressure relieving devices are essential in prolonged surgeries. The silicone gel material is known for its flexibility, durability, and hypoallergenic properties and is a part of early intervention towards successful pressure sore prevention. However, larger randomized control studies are needed to evaluate the efficiency of the technique.
References
-
Hoshowsky VM, Schramm CA (1994) Intraoperative pressure sore prevention: an analysis of bedding materials. Res Nurs Health 17(5): 333-339.
-
Odden MC, Coxson PG, Moran A, Lightwood JM, Goldman L, et al. (2011) The impact of the aging population on coronary heart disease in the United States. Am J Med 124(9): 827-833.
-
Murphy RA, Patel KV, Kritchevsky SB, Denise KH, Anne BN, et al. (2014) Weight change, body composition, and risk of mobility disability and mortality in older adults: a population-based cohort study. J Am Geriatr Soc 62(8): 1476-1483.
-
Sen CK, Gordillo GM, Roy S, Robert K, Lynn CHT, et al. (2009) Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen 17(6): 763-771.
-
Coleman S, Nixon J, Keen J, Lyn W, McGinnis E, et al. (2014) A new pressure ulcer conceptual framework. J Adv Nurs 70(13): 2222-2234.
-
Kim JM, Lee H, Ha T, Na S (2018) Perioperative factors associated with pressure ulcer development after major surgery. Korean J Anesthesiol Feb 71(1): 48-56.
-
Guyton AC (1991) Human physiology and mechanism of disease. 5th (Edn.), WB Saunders Company, pp: 124-135.
-
Gefen AR (2009) pressure-time curve for pressure ulcer risk. Part 1. Nurs Stand 23(45): 64-68.
-
Gefen AR (2009) pressure-time curve for pressure ulcer risk. Part 2. Nurs Stand 23(46): 40-44.
-
Scott SM (2016) Perioperative pressure injuries: protocols and evidence-based programs for reducing risk. Analyses.
-
Joseph J, McLaughlin D, Darian V, Hayes L, Siddiqui A (2019) Alternating Pressure Overlay for Prevention of Intraoperative Pressure Injury. Journal of Wound, Ostomy and Continence Nursing 46(1): 13-17.
-
Gould L, Abadir P, Brem H, Marissa C, Teresa CK, et al. (2015) Chronic wound repair and healing in older adults: current status and future research. Wound Repair Regen 23(1): 1-13.
-
Groeneveld A, Anderson M, Allen S, Bressmer S, Golberg M, et al. (2004) The prevalence of pressure ulcers in a tertiary care pediatric and adult hospital. J Wound Ostomy Continence Nurs 31(3): 108-116.
-
Bluestein D, Javaheri A (2008) Pressure ulcers: prevention, evaluation, and management. Am Fam Physician 78(10): 1186-1194.
-
Kosiak M (1959) Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil 40(2): 62-69.
-
Kosiak M (1991) Prevention and rehabilitation of pressure ulcers. Decubitus 4(2): 60-62.
-
Walton GPS (2009) Prevention of pressure ulcers in the surgical patient. AORN J 89(3): 538-548.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey