Very Low Calorie Ketogenic Diet (VLCKD) Becomes Further Advantageous on Addition of Medium -Chain Fatty Acids Prior to VLCKD Initiation for Obesity Treatment-A Short Communication
Having reviewed the role of different antiobesity agents, bariatric surgery, role of GM in obesity, type 1 diabetes mellitus (T1DM), role of Probiotics in non-alcoholic fatty liver disease(NAFLD)along with other co-morbidities of obesity along with type 2 diabetes mellitus( T2DM ) for obesity therapy recent again shift has come towards dietary perspectives like use of Mediterranean diet (MD) diet, very low calorie ketogenic diet (VLCKD) in therapy of obesity as well as alterations in gut microbiota (GM) subsequent to VLCKD. Here we further add how VLCKD might be made more efficacious strategy for attaining weight reduction. With recent emerging insight on how VLCKD‘s are efficacious in obesity is by emphasizing the part of medium -chain FA’s (MCT’s). Here further emphasis is laid on how utilization of MCT’s prior to initiating VLCKD active phase was much more efficacious (equivalent to 7-8kg weight reduction) in contrast to MCT’s supplementation at the time of VLCKD beginning (with practically negligible body weight reduction (-0.5 to-0.7kg) as well as Waist Circumference (WC)-1.5-1.8cm). Two times reduction in fat mass as well as escalated muscle mass was found in the VLCKD + early MCT’s group in contrast to control group is. Therefore, as much as 8kg can be lost by using this therapy holding lot of promise.
Abbreviations
T2DM: Type2 Diabetes Mellitus; CAD: Coronary Artery Disease; CVD: Cardiovascular Disease; QOL: Quality of Life; NCD: Non-Communicable Diseases; QOL: Quality of Life; IR: Insulin Resistance; VLCKD: Very Low-Calorie Ketogenic Diet; IR: Insulin Resistance; FA: Fatty Acid; AP: Adipose Tissue; GIT: Gastrointestinal Tract; IMM: Inner Mitochondrial Membrane; GPR 84: G- Protein Coupled Receptor; CRP: C Reactive Protein; GM: Gut Microbiota.
Introduction
Obesity has been acknowledged to be a chronic disease which gets correlated with plethora of comorbidities for instance Type 2 Diabetes mellitus (T2DM), hypertension, dyslipidemia), cardiovascular disease (CVD) inclusive of coronary artery disease (CAD) as well as stroke)ii)sleep abnormalities along with cancer [1]. Such comorbidities alias non-communicable diseases (NCD)-diminish the quality of life (QOL) in addition to longevity with escalated public health expenditure [1, 2].
Despite numerous approaches have been generated for achieving weight reduction, obesity tendencies are drastically escalating specifically in young adults in addition are middle income countries [3]. Apart from lifestyle factors, physical exercise, cigarette smoking, alcohol consumption, diet has further been believed to be a risk factor for Obesity in addition to NCD [4], whose modification is substantially plausible.
Out of the dietary strategies very low-calorie ketogenic diet (VLCKD) has been observed to be the maximum efficacious strategy for attaining weight reduction [5]. Additionally, it has been illustrated to diminish inflammation along with insulin resistance (IR), that portray 2 of the major initiating factors for NCD generation [6].
VLCKD gets comprised of a multistep protocol that has three major stages: i) active phase ii) dietary re-education in addition to its iii) sustenance [7]. The active stage represents the maximum significant stage of VLCKD in view of it aids in attaining of 80% of the target weight reduction with a time period of 30 of 45 days based on personalized reactions. pacey weight reduction subsequent to considerable limitation of energy ingestion (600-800kcal/day as well as a sustenance of nutritional ketosis [7].
Nutritional ketosis takes place subsequent to full consumption of carbohydrate restricted (mostly <50gdaily) due to which escalation of fatty acid (FA’s) oxidation takes place in the adipose tissue (AP) with the idea of energy generation [8]. Actually, acetylcoenzyme A CoA, the precursor of the ketone bodies inclusive of acetoacetate, ii) βhydroxy butyrate iii) acetone get utilized in the form of alternate resource of energy for a variety of tissues. Intriguingly, just FA’s that possess the carbon chain length ≤8 possess the capacity of crossing the inner mitochondrial membrane (IMM), sovereign of carnitine palmoyl acetyltransferase I enzymes [9]. In reference to this FA’s C8 (caprilic acid) might possess greater robust ketogenic actions in comparison to C10 (capric acid) in addition to C12 (lauric acid) [10]. Clinical proof illustrated that 20g of C8 generates a significantly greater robust ketogenic reactions actions in comparison to 10g of C8 [9]. Nevertheless, Norgren, et al. [11], displayed that for guaranteeing practically negligible inimical sequelae, C8 dosage has to be restricted to 15- 20g/ consumption [11]. Triglycerides (TG) which possess medium -chain FA’s (MCT’s) - possess FA’s with carbon back bone long-chain with 6-12carbon atoms associated with glycerol [12, 13]. Subsequent to consumption of diet MCT’s digestion take place by the intestinal lipases followed by absorption in the gut in the form of TG which possess long chain CoA fatty acids (LCTs>12 carbon atoms) [13]. Separate from LCTs, the FA’s possessed by MCT’s possess the capacity of binding albumin with the avoidance of generation of chylomicron. Thereby MCT’s avoid the hydrolysis brought about by plasma lipoprotein lipases in addition to in the form of sequelae getting accumulated in the AT. This gets followed by MCT’s directly gaining entry into the liver, where they might undergo metabolism by mitochondrial oxidation [14, 15]. Nevertheless, separate from LCTs, there is no requirement of carnitine modulated transportation to mitochondria. Additionally, MCT’s specifically C8 along with C10 possess the capacity of undergoing oxidation in the peroxisomes, thereby portraying a greater accessible energy resource in contrast to LCTs [15]. Different studies have illustrated that supplementation of MCT’s escalate β hydroxy butyrate quantities in a dose-based association [8, 16, 17]. Sequentially, MCT’s might support nutritional ketosis at the time of ketogenic diets [17]. Oxidation with a greater rapid metabolism in addition to lesser accrual in adipocytes MCT’s might possess the capacity of significantly affecting energy equilibrium, facilitating weight reduction which is autonomous of dietary energy ingestion [18, 19]. The mechanistic modes behind this continue to be uncharted in view of greater heterogeneity of studies accessible thus far. Certain studies have illustrated that MCT’s might escalate thermogenesis as well as sequentially affecting energy expenditure. Additionally, substituting LCTs with MCT’s was correlated with greater decreased AT in animal models in addition to humans [20, 21]. Such actions might be modulated by the particular actions of G- protein coupled receptor (GPR 84) in the AT [20]. Furthermore, MCT’s might escalate the sensation of satiety thereby restricting ingestion of food whereas facilitating regulation of body weight [21, 22, 23, 24]. Actually, ketonemia possess the capacity of anorexia generating actions at the level of the hypothalamus [22, 23]. Moreover, certain studies have pointed that MCT’s possess the capacity of the liberation of certain hormones of the gastrointestinal Tract (GIT) implicated in the sensation of hunger/ (Ghrelin as well as peptide YY respectively) [22, 24].
Clarification was not there if utilization of MCT’s might escalate the acute ketogenic reactions. However, a 30day clinical trial displayed that ingestion of caprilic acid (C8-6g twice daily) escalated βhydroxy butyrate plasma quantities from 0.1mmol/L to 0.2mmol/L [25].
Recently Vertrani, et al. [26], from the group of Muscogiuri G performed a retrospective study for evaluation of actions of MCT’s supplementation in overweight /obese subjects going through VLCKD diet or lone VLCKD diet. At the time of weight reduction using VLCKD diet. They assessed 263 overweight / obese females (with body mass index (BMI)-35.7± 5.3kg/m) with age 37.5±14.2yrs with subsequent utilization of one of such three protocols; i) control group 83 enrolled (31.6%) VLCKD without MCT’s supplementation ii) VLCKD + MCT’s group 86 enrolled (32.7%) (MCT’s supplementation 20g daily at the time of VLCKD beginning from the first day prior to initiating VLCKD active phase iii) VLCKD + early MCT’s, 94 enrolled (35.7%) (MCT’s supplementation beginning from the 5days prior to initiating VLCKD active phase. Anthropometric estimates, body constitution as well as C Reactive Protein (CRP) were determined at the initiation in addition to the termination (45 days) of VLCKD.
Thus subsequent to MCT’s supplementation associated with significant reduction in body weight , BMI in addition to WC in contrast to control group, with greater actions in the VLCKD + early MCT’s group. Two times reduction in fat mass as well as escalated muscle mass was found in the VLCKD + early MCT’s group in contrast to control group. In reference to inflammation hs CRP quantities (evaluated in the form of absolute proportion alteration) were significantly lesser in the VLCKD + MCT’s group (p=0.009) in addition to VLCKD + early MCT’s group (p=0.011) in contrast to control group. A logistic regression model illustrated that VLCKD + early MCT’s group escalated the probability of enhancement of BMI classes (OR: 1.85, 95%CI 1.02-3.36) further subsequent to adjustment for the plausible influencing factors (Figures 1 & 2).
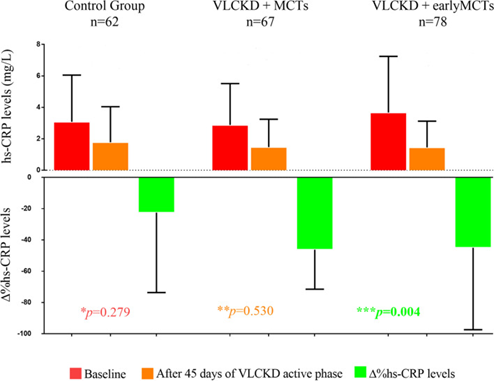
Figure1: Courtesy ref no -26-Changes in hs-CRP concentrations in the three study groups. One-way ANOVA and post hoc test for multiple comparisons (Bonferroni). A p-value in bold type denotes a significant difference (p < 0.05). * hs-CRP concentrations in the three groups at baseline. hs-CRP concentrations in the three groups after 45 days of VLCKD active phase. * The absolute percent change of hs-CRP concentrations in the three groups.
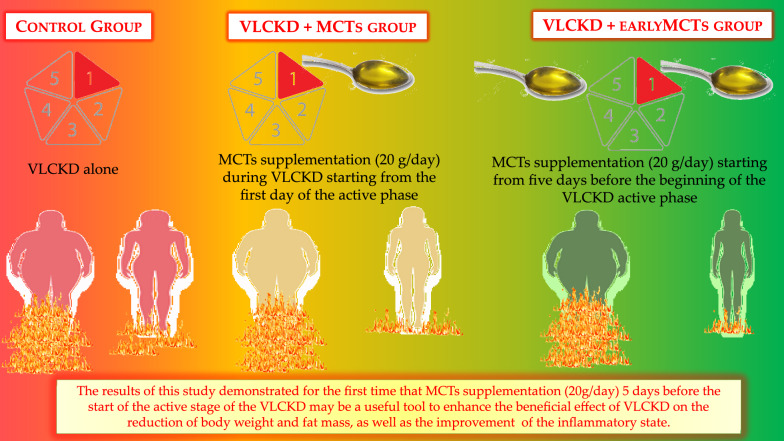
Figure2: Courtesy ref no -26-MCTs supplementation during the active stage of the VLCKD. The MCTs supplementation (20 g/day) 5 days before the beginning of the VLCKD active phase might facilitate the transition into ketosis thus contributing to the effectiveness of the nutritional intervention enhancing its beneficial effects on weight loss, body composition modulation and inflammatory status.
Thus the outcomes obtained by Vertrani, et al. [26], were in agreement with earlier studies which concentrated on MCT’s supplementation at the time of energy restricted diets [18, 19]. Actually, 2 meta-analysis [18, 19], illustrated that isoenergetic substituting LCTs with MCT’s at the time of energy restricted dietary intervention led to small decrease in body weight (-0.5 to-0.7kg) as well as WC(-1.5-1.8cm) in middle aged overweight /obese subjects. Nevertheless, once studies took into account which implicated VLCKD (<800kcal daily) with MCT’s supplementation the average weight decrease was akin to that found in Vertrani, et al. [26], study (average -8kg).
The way detailed previously metabolism of MCT’s is different from that of LCTs, in view of MCT’s possess the capacity of directly gaining entry into the liver, subsequent to intestinal absorption where they might undergo metabolism by mitochondrial oxidation as well as do not get stored [16]. Further, as detailed earlier, MCT’s possessed the capacity of escalating thermogenesis in addition to diminished fat accumulation, thereby aiding in reduction in body weight [20].
Actually, Hill, et al. [27], illustrated that MCT’s escalated thermogenesis by 50% subsequent to 6days MCT’s supplementation. Thereby such mechanistic modes might offer the reasoning of greater efficacy of reduction in body weight, which they found subsequent to initiating MCT’s supplementation prior to VLCKD. Despite reduction in fat mass was found in both VLCKD as well as MCT’s supplementation groups escalated muscle mass was found just in the VLCKD + early MCT’s group in contrast to control group.
Conclusion
In reference to mechanistic modes by which VLCKD utilization is done for the avoidance of comorbidities correlated with obesity, is reduction of systemic inflammation, in view of its antioxidant along with anti-inflammatory actions [28]. This is obtained by separate mechanistic modes for instance by hampering activation of nuclear factor-κappa light chain enhancer of activated B cells (NFκB), nucleotide- binding domain, leucine-rich-repeat containing family, pyrin domain-containing (NLRP3) inflammasome in addition to hampering histone deacetylases. Noticeably, maximum weight reduction was found in the VLCKD + early MCT’s group in contrast to rest of groups, plausibly in view of over flow of KB’s [29].
Having reviewed the role of different antiobesity agents, bariatric surgery, role of GM in obesity, T1D, role of Probiotics in non-alcoholic fatty liver disease (NAFLD along with other co-morbidities of obesity along with T2DM recent again shift has come towards dietary perspectives like use of MD diet, VLCKD in therapy of obesity as well as alterations in gut microbiota (GM) subsequent to VLCKD) [30, 31, 32, 33, 34]. Here it is displayed that MCT’s supplementation prior to VLCKD is further helpful in attaining the goal.
References
-
Dai H, Alsalhe TA, Chalghal N, Ricco M, Bragazzi NL, et al. (2020) The Global burden of Disease attributable to high body mass index in 195 countries and territories, 1990- 2017: analysis of the Global burden of Disease study. PLoS Med 17(17): e10003198.
-
Afshin H, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. (2017) Health effects of overweight and obesity in 195 countries over 25years. N Engl J Med 377(1): 13-27.
-
Lozhano R, Naghavi M, Foreman K, Lim S, Shibuya K, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in1990 and 2017:a systematic analysis for the Global burden of Disease study 10. Lancet 380(9859): 2095-128.
-
GBD 2017 Diet Collaborators (2019) Diet collaborators Health effects of dietary risks in 195 countries, 1990- 2017: a systematic analysis for the Global burden of Disease study 17. Lancet 393(10184): 1958-1972.
-
Muscogiuri G, El Ghoch M, Colao A, Hassapidou M, Yumuk V, et al. (2021) Obesity Management Task Force (OMTF)of the European Association for the study of Obesity(EASO) European Guidelines for Obesity Management in with a very low calorie ketogenic diet (VLCKD)in patients with obesity and over weight: a systematic review and meta- analysis. Obes Facts 14(2): 222-245.
-
Mohammadifard N, Haghhighatdoost F, Rahmlou M, Rodriques APS, Gaskarei MK, et al. (2022) The effects of ketogenic diet on shared risk factors of cardiovascular disease (CVD), and cancer. Nutrients 14(17): 3499.
-
Muscogiuri G, Barrea L, Laudisio D, Pugliese G, Salzano C, et al. (2019) The management of very low calorie ketogenic diet in obesity out-patient clinic. A Practice Guide. J Transl Med 17(1): 356.
-
Harvey CDC, Schoffield GM, Williden M (2018) The use of nutritional supplement to induce ketosis and symptoms associated with keto induction: a narrative review. Peer J 6: e4488.
-
Khabbush A, Orford M, Tsai YC, Rutherford T, Donnell OM, et al. (2017) Neuronal decanoic acid oxidation is markedly lower than that of octanoic acid: a mechanistic insight into the medium-chain triglyceride ketogenic diet. Epilepsia 58(8): 1423-1429.
-
Lin TY, Liu HW, Hung TM (2021) The ketogenic effects of medium-chain triglycerides. Front Nutr 7: 74728440.
-
Norgren J, Sindi S, Sandebring Matton A, Kareholt I, Danillidou M, et al. (2020) Ketosis after intake of coconut oil and caprilic acid with and without glucose: a cross over study in healthy older adult. Front Nutr 7: 40.
-
Clegg ME, Golsorkhi M, Henry CJ (2013) Combined medium-chain triglycerides and chill feeding increase diet induced thermogenesis in normal weight humans. Eur J Nutr 52(6): 1579-1585.
-
Lee YY, Tang TK, Lai OM (2012) Health benefits, enzymatic production, and application of medium-and long-chain triacylglycerol (MLCT) in food industries: a review. J Food Sci 77(8): 137-144.
-
Rego Costa AC, Rosado EL, Soares Mota L (2012) Influence of dietary intake of medium -chain triglycerides on body composition, energy expenditure and satiety: a systematic review. Nutr Hosp 27(1): 103-108.
-
Wanten GJ, Naber AH (2004) Cellular and physiological effects of medium -chain triglycerides. Mini Rev Med Chem 4(8): 847-857.
-
Krotkiewski M (2001) Value of VLCKD supplementation with medium-chain triglycerides. Int J Obes Relat Metab Disord 25(9): 1393-1400.
-
Harvey CJ, Schoffield GM, Williden M, McQuillan JA (2018) Effect of medium -chain triglycerides on nutritional ketosis and symptoms of ketoinduction in healthy adults: A randomized controlled Clinical trials. J Nutr Metab 2018: 2630565.
-
Bueno NB, de Melo IV, Florêncio TT, Sawaya AL (2015) Dietary medium-chain triacylglycerols versus long- chain triacylglycerols for body composition in adults: systematic review and meta-analysis of randomized controlled trials. J Am Coll Nutr 34(2): 175-183.
-
Mumme K, Stonehouse W (2015) Effects of medium -chain triglycerides on weight loss and body composition:a meta-analysis of randomized controlled trial. J Acad Nutr Diet 115(2): 249-263.
-
Hara T, Kashihara D, Ichimura A, Kimura I, Tsujimoto G, et al. (2014) Role of free fatty acid receptors in the regulation of energy metabolism. Biochim Biophys Acta 1841(9): 1292-1300.
-
Swarnamali H, Ranasinghe P, Hills AP, Jayawardena R (2021) Coconut oil consumption and bodyweight reduction: a systematic review and meta-analysis. Minerva Endocrinol.
-
St Onge MP, Jones PJ (2002) Physiological effects of medium -chain triglycerides: potential in the prevention of obesity. J Nutr 132(3): 329-332.
-
Deemer SE, Plaisance EP, Martins C (2020) Impact of ketosis on appetite regulation-a review. Nutr Res 77: 1-11.
-
Maher T, Clegg ME (2020) Dietary with potential affect satiety mechanisms and evidence. Crit Rev Food Sci Nutr 77: 1-11.
-
Courchesne Loyer A, Fortier M, Tremblay Mercier J, Choinard Watk R, Roy M, et al. (2013) Stimulation of mild sustained ketonemia by medium -chain triglycerides in healthy humans: estimated contribution to potential energy metabolism. Nutrition 29(4): 635-640.
-
Vertrani C, Verde L, Savastano S, Colao A, Muscogiuri G, et al. (2023) Supplementation with medium -chain fatty acidsincreases body weight loss during very low calorie ketogenic diet a real life setting. J Transl Med 21: 29.
-
Hill JO, Peters JC, Yang D, Sharp T, Kaler M, et al. (2019) Thermogenesis in humans during overfeeding with medium -chain triglycerides. Metabolism 38(7): 641- 648.
-
Monda V, Polito R, Lovino A, Finaldi A, Valenzano A, et al. (2020) Short term physiological effects of very low calorie ketogenic diet: effects on adiponectin levels and inflammatory status. Int J Mol Sci 21(9): 3228.
-
Freemantle E, Vandal M, Tremblay Mercier J, Plourde M, Poirier J, et al. (2009) Metabolic response a ketogenic breakfast in the healthy elderly. J Nutr Health Ageing 13(4): 293-298.
-
Kaur KK (2018) Sarcopenia: New perspectives of use of ketogenic diet in endocrine dysfunction: how to use with indications and contraindications. Acta Scientific Nutritional Health 3(1): 1-8.
-
Kaur KK, Allahbadia GN, Singh M (2023) Mediterranean diet still holds a Place in Obesity Treatment Despite the Considerable Effectiveness of the Very Low Calorie Ketogenic Diet (VLCKD): A Short Communication’. Obes Res Open J 10(1): 1-5.
-
Kaur KK, Allahbadia GN, Singh M (2020) The association of dietary fatty acids and gut microbiota alterations in the development of neuropsychiatric diseases: A systematic review. Obes Res Open J 7(1): 19-45.
-
Kaur KK, Allahbadia GN, Singh M (2019) Have Probiotics and Synbiotics passed the test of time to be implemented in management of obesity and related metabolic disorders-a comprehensive review. Adv Obes Weight Manag Control 9(1): 21-28.
-
Kaur KK, Allahbadia GN, Singh M (2023) Very Low Calorie Ketogenic Diet (VLCKD)possesses further advantageous actions over ’Mediterranean diet in terms of better enhancement of Gut Microbiota (GM) in type2 Diabetes mellitus Patients- A Short Communication. J Diab Metab Disorder 10(1): 48-54.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey