Cardiovascular Outcomes with Liraglutide: An Update following LEADER
Diabetes Mellitus is one of the most important causes of cardiovascular disease in the United States and worldwide. Few antidiabetic drugs (e.g. Rosiglitazone) have faced cardiovascular (CV) safety related controversies in the recent past. The FDA mandatory advisory states that the CV safety concerns of any new antidiabetic drug should be thoroughly addressed in a dedicated longitudinal outcome trial. Liraglutide, a long-acting GLP-1 agonist, approved as a 2nd line agent in the treatment of type 2 diabetes mellitus (DM), has shown some promising effects on the cardiovascular system in various preclinical and early clinical studies. In accordance with the FDA recommendation, a large, multicenter trial (LEADER) was undertaken in 2010 to look for long-term CV outcome data on liraglutide. Primary outcome (Death due to CV causes, nonfatal MI or, nonfatal stroke) occurred in significantly fewer patients in the liraglutide group, with a lower incidence of cardiovascular and all-cause mortality. Besides, a better glycemic control, fewer hypoglycemic events, significant weight loss, and beneficial effects on nephropathy were observed in patients on Liraglutide. ELIXA trial on Lixisenatide did not reveal any significant CV benefit. So, Results from the ongoing CV outcome trials on other GLP-1 agonists (EXSCEL for Exenatide, HARMONY for Albiglutide, and REWIND study for Dulaglutide) will guide us better to determine whether the observed benefit is indeed a class effect or a molecule effect. Here we have summarized all the cardiovascular outcome data so far available on liraglutide, with special reference to the recently published LEADER trial results.
Introduction
Diabetes Mellitus (DM) is the most important non- communicable disease of the modern era, currently affecting approximately 29.1 million people in the United States. Every year, on an average, a whopping 1.7 million new cases of diabetes are found in individuals of 20 years of age or, older. It was the seventh leading cause of mortality in US population in the year 2010, with the cardiovascular mortality being 1.7 times higher in adults with diabetes, compared to those without it [1]. Hospitalization rate due to CV events (myocardial infarction or, stroke) is also found to be higher among patients with diabetes [2]. Diabetes mellitus, with its various micro and macro vascular complications, is considered as one of the most weighed cardiovascular risk factors, and labeled as CHD-equivalent as per NCEP (National Cholesterol Education Program) expert panel report [3]. Among the available therapeutic options for the treatment of type 2 diabetes mellitus, several newer classes of drugs have come up in recent years, like molecules targeting the incretin system (e.g. GLP-1 receptor agonists, DPP-IV inhibitors) or, drugs acting on the renal glucose excretion (SGLT-2 inhibitors), alongside the trusted ones, insulins and metformin. After all the cardiovascular safety related controversies regarding rosiglitazone, USFDA recommended that CV risk concerns should be addressed more thoroughly during the development of a new antidiabetic drug [4]. GLP-1 agonists (e.g. exenatide, liraglutide, lixisenatide, etc.) are drugs acting on the incretin system of our body, with several established beneficial effects like weight loss and blood pressure reduction, along with a better glycemic control in diabetics. The DURATION-6 trial reported a better glycemic control with liraglutide, compared to exenatide [5]. Several preclinical and early clinical studies have shown a spectrum of cardioprotective effects of liraglutide. Few meta-analysis performed in the recent past confirmed the cardiovascular safety of GLP-1 receptor agonists as well [6]. But, following the FDA advisory for the longitudinal outcome data in all newer antidiabetics, a large multicenter, international trial was undertaken in 2010, namely LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results- NCT01179048) trial (Table 1). Very recently the results of this trial have been published, showing a significant cardiovascular benefit in patients on liraglutide [7]. Hence, our review aims to summarize all the cardiovascular outcome data so far available on liraglutide, with special reference to the recently published LEADER trial results (Table 2).
Importance of CV outcome data on newer Anti diabetics
Diabetes itself is the most important cause of cardiovascular morbidity and mortality in the United States and worldwide. Few antidiabetic drugs have been found to be associated with adverse CV outcomes. There was one such huge controversy regarding rosiglitazone, when a meta-analysis of 42 RCTs was published in 2007, showing a statistically significant increased risk of myocardial infarction (OR 1.43) in patients on rosiglitazone. In the same study, the odds ratio for cardiovascular mortality in rosiglitazone group (compared to control group) was 1.64 (95% CI, 0.98 to 2.74; p =0.06) [8]. Following this study, the American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD), and subsequently the FDA put a restriction on using rosiglitazone in diabetic individuals. However, later in 2013 FDA finally removed the restrictions, following the analysis of the RECORD trial data, which failed to show any significant increase in CV risk with rosiglitazone, when compared to other standard antidiabetic medications [9, 10]. After this controversy FDA came up with a guideline to address the CV safety concerns of antidiabetic drugs more thoroughly, and since then, there has been a profound change in the way a new antidiabetic drug is evaluated and brought to the market [4]. So, in accordance with the mandatory advisory, the endpoints like cardiovascular mortality, the incidence of myocardial infarction, stroke, and hospitalization for heart failure, were included in the most recent clinical studies on novel antidiabetic drugs. Among studies with DPP-4 inhibitors, the SAVOR-TIMI 53 trial (saxagliptin) and EXAMINE trial (alogliptin) satisfied the required CV endpoint criteria, with no increased risk for CV events compared to placebo. There was a concern over an increased risk of hospitalization for heart failure in patients getting DPP-4 inhibitors, as noted in both these trials [11, 12]. However, the recently published TECOS (sitagliptin) trial data did not reveal any similar concerns [13]. Regarding the other newer drug class SGLT-2 inhibitors, the recently published results of EMPA-REG study (with empagliflozin) showed a significantly lower incidence rate of MACE (major adverse cardiovascular event), hospitalization for heart failure, and CV mortality in patients on empagliflozin, as compared to placebo [14]. In the drug class of GLP-1 agonists, ELIXA study (ClinicalTrials.gov id. NCT01147250) looked into the effects of lixisenatide on CV outcome in patients with type 2 diabetes and a recent ACS, and no significant difference was observed between lixisenatide group and place bo group with regard to the primary CV endpoints [15]. LEADER trial (NCT01179048) for liraglutide, initiated in the year 2010, has recently come up with the CV outcome data [7]. Among the other large, multicenter studies involving GLP-1 receptor agonists, the HARMONY study (NCT02465515) for albiglutide, REWIND study (NCT01394952) for dulaglutide, and EXSCEL study (NCT01144338) for the once-weekly formulation of exenatide are ongoing, and results are expected in the next few years [16, 17, 18]. The key characteristics of all the completed and ongoing CV outcome trials on GLP-1 agonists are summarized in Table 3.
GLP and GLP-1 Agonists
Incretin-based therapy is one of the major emerging second-line agents for the treatment of type 2 diabetes mellitus. In the year 1960, it was first shown that the oral administration of glucose causes more insulin secretion than parenteral glucose. The incretin hormones are responsible for nearly 50-70% of postprandial insulin secretion [19]. Primarily two incretin hormones, namely glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1), are responsible for the excess secretion of insulin after an oral glucose load. GIP consists of 42 amino acids and was first isolated from the porcine gut mucosa. It is synthesized and secreted from the intestinal K-cells. Besides augmenting the postprandial insulin secretion, it also inhibits gastric emptying and acid secretion [20]. GLP-1 is secreted by ileal L-cells in response to the presence of carbohydrate, protein or fat inside the intestinal lumen. After release, it is rapidly metabolized by the enzyme dipeptidyl peptidase IV (DPP-4), and its half-life is near about 2 minutes. In DPP-4 deficient mice model, circulating GLP-1 and GIP have found to be elevated [21, 22]. Two different strategies for treating diabetes have been devised, based on the incretin physiology. These includes using a GLP-1 receptor agonist or inhibiting DPP-4 enzyme to prevent the breakdown of GLP-1. Synthetic GLP-1 agonists are resistant to degradation by the enzyme DPP-4. GLP-1 increases glucose-dependent insulin secretion and insulin sensitivity, inhibits glucagon release, delays gastric emptying, and increases the beta cell mass [23]. It also acts centrally to enhance early satiety, decrease the pleasure associated with food, and reduce the food intake [24]. Exenatide was the first GLP-1 agonist approved by FDA in the year 2005. Subsequently, liraglutide, dulaglutide, and lixisenatide were approved. These agents are commonly used in addition to 1st line antidiabetic agent like metformin. The advantage of these agents is once daily or, even once weekly dosing of some GLP-1 agonist preparation, the only limitation being the high cost of therapy. The use of GLP-1 agonist and insulin simultaneously has been approved recently by ADA and EASD [25]. Recently an FDA advisory panel voted for the use of long-acting insulin degludec with liraglutide [26]. Liraglutide (NN2211, Victoza; Novo Nordisk of Bagsvaerd, Denmark) was approved on January 25, 2010, by USFDA for the treatment of type 2 diabetes mellitus and on December 23, 2014, for the treatment of obesity [27, 28]. It is a long- acting GLP-1 receptor agonist, which is administered as subcutaneous once daily. DURATION-6 trial (n= 911 patients) showed that there was a greater reduction in HbA1c level with liraglutide (-1.48 %) with liraglutide, in comparison to once weekly exenatide (-1.28 %) over 26 weeks [5].
- Liraglutide – a long-acting GLP-1 agonist
- An acylated GLP-1 agonist with 97% amino acid sequence homology to endogenous GLP-1.
- Resistant to degradation by DPP-IV and NEP enzymes.
- Potentiates the action of endogenous GLP-1–increases glucose-dependent insulin secretion.
- Plasma half-life is 13 hours - Once daily subcutaneous dosing.
- Approved for use in Type 2 Diabetes Mellitus and Obesity.
- Causes a greater reduction in HBA1c level, compared to Exenatide.
- Beneficial effects on Blood pressure and Body weight/ BMI.
Table 1: Liraglutide – a long-acting GLP-1 agonist.
Non-cardiovascular adverse effects of GLP-1 agonists
Adverse effects of GLP-1 agonists are very minor, rarely requiring a discontinuation of therapy. Most common is gastrointestinal adverse effects, which are seen more with liraglutide (10.5-45% people in trials reported nausea), as compared to exenatide. Nausea was short-lasting, occurring following treatment initiation or, dose escalation, usually resolving by four weeks for liraglutide (as opposed to 8 weeks for exenatide) [29, 30, 31, 32]. Rate of hypoglycemic attacks was relatively lower (3-12%) in diabetic patients treated with GLP-1 agonists alone, though more in the presence of concurrent sulfonylurea therapy [31, 32, 33, 34]. Use of the long-acting preparation of exenatide was associated with various upper respiratory tract infections (e.g. sinusitis, nasopharyngitis, etc.) in some trials [35]. Few reports of pancreatitis following therapy with GLP-1 agonists triggered a black-box warning for both exenatide and liraglutide [30, 36]. Animal studies with liraglutide observed the occurrence of few cases of thyroid C-cell tumors, leading to a warning for this too. Though clinical trials did not reproduce this finding, caution must be taken while using liraglutide in patients with personal or, family history of medullary carcinoma thyroid [36].
Extraglycemic effects of GLP-1 agonists
Cardiovascular effects: GlP-1 receptors have been identified in various sites of our cardiovascular system, like in vascular smooth muscle cells, endothelial cells, and the autonomic nuclei [37, 38, 39]. Stimulation of the GLP-1 receptors in these autonomic nuclei has been shown to result in an increase in heart rate and blood pressure [40]. However, clinical studies using GLP-1 agonists usually have shown BP lowering effects, with no significant change in heart rate as such [41]. A recent animal study with liraglutide observed the potential role of GLP-1 receptor-dependent secretion of ANP (atrial natriuretic peptide) in the reduction of blood pressure [42]. Various cardiac abnormalities (e.g. diastolic impairment, change in cardiac structure, etc.) have been noted in rodents lacking functional GLP-1 receptors [37]. Cardioprotective and vasodilatory effects of GLP-1 are known to be mediated through two distinct pathways – one dependent on GLP-1 receptor itself, and the other involving the 9-36 peptide (a metabolite of GLP-1) [37]. GLP-1 has been shown to increase the glucose uptake in cardiac myocytes, thus helping in the optimization of the myocardial oxygen efficiency [43]. Preclinical studies have shown that GLP-1 can activate the pro-survival kinase pathways (PI3K and ERK1/2) in cardiomyocytes in the setting of ischemic injury, thereby preventing the activation of apoptosis in these cells [44].Recent studies have also found a role of GLP-1 receptor-mediated cAMP-ePAC2 signaling in the cardio protection [42]. In the porcine model of ischemia, exenatide reduced the infarct size and caused an improvement in cardiac function [45]. In mice with induced diabetes and myocardial infarction, pre-treatment with Liraglutide led to a reduction in the incidence of cardiac rupture, improvement in cardiac output, and an improved overall survival [46]. GLP-1 has also been found to be beneficial to the heart, when administered as a 72-hour infusion following angioplasty in patients with acute MI and left ventricular dysfunction [47]. In patients undergoing coronary artery bypass grafting (CABG), a continuous GLP-1 infusion beginning 12 hours before the procedure and continuing for 48 hours, was associated with less requirement of inotropes and reduced incidence of arrhythmias, along with a better glycemic control [48]. A recent study has shown that in patients with coronary artery disease, the intravenous GLP-1 infusion is protective against ischemic dysfunction following dobutamine stress [49]. Few studies, however, have found a neutral effect of liraglutide on the infarct size and coronary reperfusion [50]. GLP-1 infusion has been shown to improve left ventricular ejection fraction, functional status, and quality of life in patients with NYHA class III/IV heart failure [51]. Both exenatide and liraglutide have been found to have a protective role in animal models of atherogenesis, through various mechanisms like reduction of intimal hyperplasia and attenuation of expression of cell adhesion molecules [52, 53, 54]. GLP-1 agonists have been shown to cause a reduction in the level of several cardiovascular risk markers like hs- CRP, PAI-1, and BNP as well [55, 56]. GLP-1 receptor agonists also exert beneficial effects on the endothelial function through their action on receptors present in the endothelial cells. Studies have shown that GLP-1 reduces the TNF-alpha mediated expression of PAI- 1 (plasminogen activator inhibitor-1) in vascular endothelial cells [57]. PAI-1 produced in the setting of myocardial infarction is found to be associated with endothelial dysfunction in the coronary arteries, and thereby it further aggravates the left ventricular dysfunction [58]. Liraglutide has been shown to increase the endothelial nitric oxide synthase (e-NOS) activity and nitric oxide (NO) production in rats with streptozocin- induced diabetes [59]. Flow-mediated vasodilation (FMD) is an important measure of endothelial function, and GLP- 1 infusion has been shown to significantly increase the FMD in brachial arteries of healthy subjects. It also reduced the hyperglycemia-induced oxidative stress and incident endothelial dysfunction in diabetic patients [60]. However, in another recent study, liraglutide didn’t significantly alter the endothelial-dependent vasodilation, measured by forearm blood flow (FBF) [61]. The summary of all the cardiovascular effects of GLP-1, along with the possible mechanisms have been depicted in Figure 1.
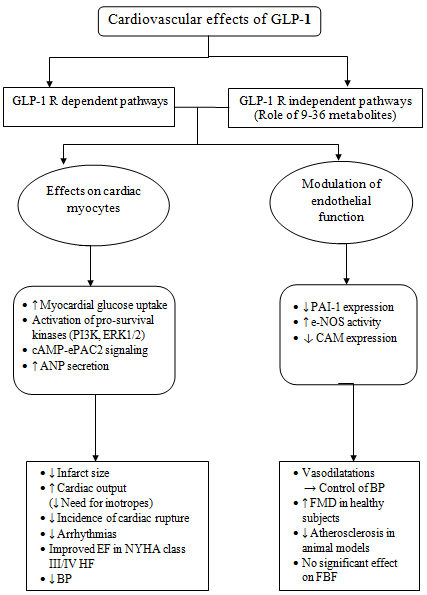
[ANP= Atrial Natriuretic Peptide, PAI= Plasminogen Activator Inhibitor, e-NOS= Endothelial Nitric Oxide Synthase, CAM= Cell Adhesion Molecule, EF= Ejection Fraction, NYHA= New York Heart association, HF= Heart Failure, FMD= Flow Mediated Vasodilatation, FBF= Forearm Blood Flow] CNS and GI effects: GLP-1 receptors are present in areas of CNS that regulate gastric motility, satiety, and feeding in individuals [62, 63, 64]. By delaying gastric motility and promoting satiety, GLP-1 leads to weight loss in obese subjects as well as in patients with Diabetes [65]. Animal studies with liraglutide showed that it reduces food intake, mainly the fats and simple carbohydrates [66]. This anorexigenic effect of this GLP-1 agonist is thought to be mediated by paraventricular nucleus of hypothalamus and area postrema of the brainstem, as noted in brain MRI of fasting mice [67]. Among other CNS effects, stimulation of GLP-1 receptors has been associated with several neuroprotective effects as well. GLP-1 analog is shown to increase the cholinergic activity in areas of the brain, thereby preventing glutamate-induced cytotoxicity [68]. Metabolic profile: GLP-1 agonists tend to have an indirect beneficial cardiovascular effect through their action on various components of the metabolic profile of patients. Studies have found a crucial role of GLP-1 receptor signaling in the biosynthesis and secretion of lipoproteins in the intestine [69]. Significant reduction in the triglyceride level was observed in diabetic patients on daily liraglutide or twice daily exenatide [32, 70]. Moreover, a significant reduction in LDL-C level and non- significant changes in HDL-C were found with the liraglutide use (1.2 or, 1.8 mg/day) [32, 71]. Studies in diabetic patients showed that GLP-1 infusion led to a reduction in serum concentration of free fatty acid (FFA) level, which improves the insulin sensitivity in patients [32, 72]. All these above mentioned metabolic effects, as well as the effect on food intake and satiety, finally lead to a significant weight loss observed in patients treated with a GLP-1 agonist. Treatment with liraglutide produced a dose-dependent weight loss (1.0 kg to 3.68 kg) in patients, which sustained up to 104 weeks. It had a significant beneficial effect on waist circumference and visceral adiposity, which is considered as important cardiovascular risk factors [73, 74, 75, 76]. In a study using a large clinical database, diabetic patients treated with exenatide had a mean weight loss of 3 kg, compared to a 1.1kg loss in sitagliptin-treated patients and 0.6kg loss in individuals getting insulin [77]. Reno protective effects: Studies have shown that GLP-1 infusion leads to a dose-dependent increase in salt excretion by kidneys and a reduction in glomerular hyper filtration. These effects play a role in the control of hypertension and end-organ damage [78, 79]. GLP-1 helps in attenuation of the progression of diabetic nephropathy, by down regulating the expression of RAGE (receptor for advanced glycation end products) in endothelial and mesangial cells of the kidney, and also by decreasing the generation of the reactive oxygen species (ROS) [80, 81].
Cardiovascular Outcome Data on Liraglutide
Meta-analysis of RCTs
In 2013, a meta-analysis was performed including 37 randomized controlled trials of at least six months duration, comparing GLP-1 agonist with a non-GLP-1 agonist drug in patients with T2DM. Out of the 37 trials, 33 provided information on major cardiovascular events (MACE), and at least one event was reported by 25 of them. GLP-1 agonist was found to be associated with a significantly reduced incidence of MACE (Major Adverse Cardiovascular Event), in comparison to placebo or pioglitazone. A non-significant trend towards similar reduction was observed in DPP-4 inhibitor-controlled studies as well. No significant effect on all-cause and cardiovascular mortality was noted. GLP-1 agonist use was also associated with a significant reduction in BMI and the systolic blood pressure of patients when compared to placebo, insulin, pioglitazone, and sulfonyl ureas. Reports from six trials in this meta-analysis showed GLP-1 causes 1-2 bpm elevation in heart rate. Though increased heart rate is associated with cardiac morbidity and mortality, [82] overall cardiovascular safety of GLP-1 agonist was established in this analysis of short-term studies involving low-risk individuals [83].
Data from LEADER trial
Though several studies had hinted on the possible beneficial cardiovascular effects of liraglutide, the need of the hour was a long duration randomized controlled trial. LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results- NCT01179048), a phase 3, randomized, multicenter, double-blind, placebo-controlled clinical trial, was undertaken in 2010. Here long-term follow-up (median follow-up period was 3.8 years) of 9340 patients with type II diabetes mellitus was done, to address the CV safety concerns on the drug liraglutide [7]. The primary endpoint in LEADER trial was a composite of death from cardiovascular causes, nonfatal myocardial infarction (MI), or nonfatal stroke, and the hypothesis was to prove the non-inferiority of liraglutide to placebo. Patients included in this study were aged 50 years or, more, and had at least one pre-existing cardiovascular condition in the form of coronary artery disease, cerebrovascular disease, peripheral vascular disease, chronic kidney disease (stage 3 or greater), or NYHA class II/III heart failure. Individuals who were 60 years of age or, older and possessed at least one of the cardiovascular risk factors (microalbuminuria, hypertension and left ventricular hypertrophy, left ventricular dysfunction, or an ankle– brachial index < 0.9) were also considered eligible for the study. Patients with type 1 diabetes, those with prior use of GLP-1–receptor agonists, dipeptidyl peptidase 4 (DPP- 4) inhibitors, pramlintide, or rapid-acting insulin, were excluded from the study. Individuals with a personal or family history of multiple endocrine neoplasia (MEN) type 2 or medullary carcinoma thyroid and those who had a recent (<14 days of screening) acute coronary or cerebrovascular event, were not considered for the study. Regarding the results, the primary outcome was seen in fewer patients in the liraglutide group (608 of 4668 patients i.e.13.0%), as compared to the placebo group (694 of 4672 i.e.14.9%) (HR 0.87; 95% CI, 0.78 to 0.97; p<0.001 for non-inferiority; p= 0.01 for superiority). A significantly fewer cardiovascular mortality was noted in patients who were on liraglutide (219 patients), in comparison to the placebo group (278 patients) [p value=0.007]. The incidence of death from all causes was also lower in the liraglutide group, and a non-significant lesser incidence of non-fatal MI and stroke was observed in the liraglutide group. Looking at the glycemic control, a mean difference of glycated hemoglobin between the liraglutide group and the placebo group was −0.40% (95% CI, −0.45 to −0.34). Interestingly, severe hypoglycemia occurred in fewer patients in the liraglutide group (114 vs. 153 patients in the placebo group). There was a 31% less incidence of severe hypoglycemia and 20% less incidence of the combination of severe and confirmed hypoglycemia with liraglutide. Regarding the effects on other CV risk factors, a 2.3 kg higher weight loss and 1.2 mm Hg lower systolic blood pressure were noted in patients getting liraglutide. However, there was a mild increase in the diastolic blood pressure (0.6 mm Hg) and heart rate (3 bpm) in the liraglutide group, compared to placebo. The events related to nephropathy were less frequent in the patients getting liraglutide, though there was a non-significant higher incidence of retinopathy. Regarding the non-cardiovascular safety concerns, a non-significant higher rate of pancreatic cancer was found in the liraglutide group (13 patients vs. five patients on placebo). Acute pancreatitis occurred in less number of patients in the liraglutide group (18 vs. 23 in the placebo group), whereas acute gallstone disease was commoner with liraglutide. Gastrointestinal adverse events, causing a permanent discontinuation of the drug were more common with liraglutide in comparison to placebo. Looking at the limitations of this trial, patients were followed for only 3.5 to 5.0 years. A long-term follow-up is still needed for better addressing all the safety concerns associated with the drug. Patients recruited in this study
- had already a high baseline risk for cardiovascular disease. So, it is not clear whether the study outcome can also be applied to the patients with a lower risk profile.
- Conclusion
- Principal findings in the LEADER trial
- Significant reduction in death due to cardiovascular events, incidence of nonfatal MI and nonfatal stroke in the Liraglutide group.
- A reduction in the all-cause mortality with
- Liraglutide use.
- Better glycemic control along with lesser incidence of hypoglycemic attacks.
- Significant weight loss and SBP reduction.
- Beneficial effect on Diabetic Nephropathy.
- No increased risk of pancreatitis.
Table 2: Principal findings in the LEADER trial.
Ever since the big controversy regarding rosiglitazone, long-term prospective trial showing the cardiovascular outcome data on all the newer anti diabetic drugs are considered very crucial. Liraglutide has been found to have several beneficial cardiovascular effects in different preclinical and early clinical studies. The results of the LEADER trial affirmed that the use of liraglutide in diabetic patients is associated with a significant reduction in the cardiovascular events and mortality. Moreover, the promising results in patients with diabetic nephropathy, a decreased incidence of hypoglycemic events and the observed reduction in body weight and blood pressure makes it a desirable therapeutic option for diabetic patients. With the lixisenatide not showing the cardiovascular benefit in ELIXA trial, and the data from the ongoing EXSCEL trial for exenatide still not being available, liraglutide will be considered as the go-to GLP-1 agonist in the coming years, as a second line option in the treatment of type 2 DM.
| ClinicalTrials | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Drug name | Trial | Official Title | Current | Primary | |||||||||||||||||||
| .gov | Phase | Key results | |||||||||||||||||||||
| name | of the trial | status | outcome | ||||||||||||||||||||
| identifier | |||||||||||||||||||||||
| Lixisenatide | ELIXA | NCT 1147250 | A Randomized, Double-blind, Placebo- controlled, Parallel-group, Multicenter Study to Evaluate Cardiovascular Outcomes During Treatment with Lixisenatide in Type 2 Diabetic Patients After an Acute Coronary Syndrome. | Phase III | Completed | Time to first occurrence of any of the following: death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for unstable angina. | A primary end-point event occurred in 406 patients (13.4%) in the lixisenatide group and in 399 (13.2%) in the placebo group (hazard ratio, 1.02; 95% confidence interval [CI], 0.89 to 1.17), which showed the non- inferiority of lixisenatide to placebo |
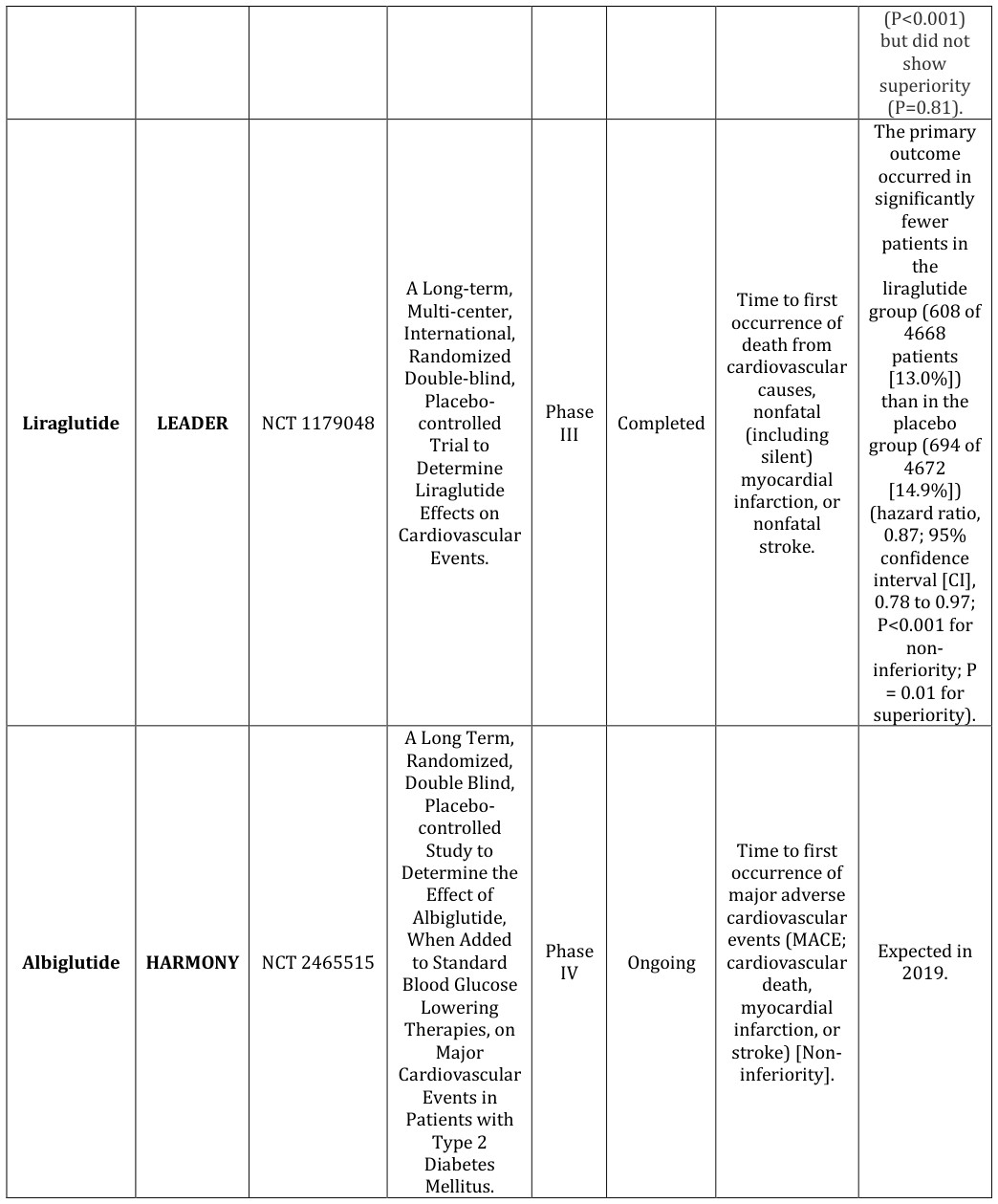
| Dulaglutide | REWIND | NCT 1394952 | The Effect of Dulaglutide on Major Cardiovascular Events in Patients with Type 2 Diabetes: Researching Cardiovascular Events with a Weekly Incretin in Diabetes. | Phase III | Ongoing | Time from randomization to first occurrence of cardiovascular death, non- fatal myocardial infarction, or non-fatal stroke (a composite cardiovascular outcome). | Expected in 2018. |
|---|---|---|---|---|---|---|---|
| Exenatide | EXSCEL | NCT 1144338 | Exenatide Study of Cardiovascular Event Lowering Trial (EXSCEL). A Randomized, Placebo Controlled Clinical Trial to Evaluate Cardiovascular Outcomes After Treatment with Exenatide Once Weekly in Patients with Type 2 Diabetes Mellitus. | Phase III | Ongoing | The primary efficacy outcome variable is defined as the composite endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke. | Expected in 2018. |
Table 4: Characteristics of completed and ongoing cardiovascular outcome trials on GLP-1 agonists.
References
-
National Centre for Chronic Disease Prevention and Health Promotion, National Diabetes Statistics Report, 2014-report estimates of diabetes and its burden in the united states.pdf.National Health and Nutrition Examination Survey estimates applied to 2012 U.S. Census data. (2012).
-
MillerBR, NguyenH,Jia-Haur Hu C, LinC, Nguyen QT(2014) New and emerging drugs and targets for type 2 diabetes: reviewing the evidence. Am Health Drug Benefits 7(8): 452-463.
-
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (Ed.), Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report, Circulation 106. (2002) 106(25): 3143-421.
-
Center for Drug Evaluation and Research. (2008) Guidance for Industry Diabetes Mellitus: Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes.
-
Buse JB, Nauck M, Forst T, Sheu WH, Shenouda SK, et al. (2013) Exenatide once weekly versus liraglutide once daily in patients with type 2 diabetes (DURATION-6): Arandomised, open-label study. Lancet 381(9861): 117-124.
-
Monami M, Dicembrini I, Nardini C, Fiordelli I, Mannucci E(2014) Effects of glucagon-like peptide-1 receptor agonists on cardiovascular risk: a meta- analysis of randomized clinical trials. Diabetes ObesMetab 16(1): 38-47.
-
Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, et al. (2016) LEADER Steering Committee on behalf of the LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 13375(4): 311-322.
-
NissenSE,Wolski K (2007) Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes, N Engl J Med 14 356(24): 2457-2471.
-
US Department of Health andHuman Services, FDA drug safety communication: FDA eliminates the risk evaluation and mitigation strategy (REMS) for rosiglitazone containing diabetes medicines 2013.
-
Mahaffey KW, Hafley G, Dickerson S, Burns S, Tourt- UhligvS, et al. (2013) Results of a reevaluation of cardiovascular outcomes in the RECORD trial. Am Heart J 166(2): 240-249.
-
Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, et al. (2013) SAVOR TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 369(14): 1317-1326.
-
Zannad F, Cannon CP, Cushman WC, Bakris GL, Menon V, et al. (2015) EXAMINE investigators. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial. Lancet23 385(9982): 2067-2076.
-
Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, et al. (2015) Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. The New England Journal of MedicineJ 16 373(3): 232-242.
-
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, et al. (2015) Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 373(22): 2117-2128.
-
Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, et al. (2015) Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 373(23): 2247-2257.
-
Bush MA, Matthews JE, De Boever EH, Dobbins RL, Hodge RJ, et al. (2009) Safety, tolerability, pharmacodynamics and pharmacokinetics of albiglutide, a long-acting glucagon-like peptide-1 mimetic, in healthy subjects. Diabetes ObesMetab 11(5): 498-505.
-
Jimenez-Solem E, Rasmussen MH, Christensen M, Knop FK. (2010) Dulaglutide, a long-acting GLP-1 analog fused with an Fc antibody fragment for the potential treatment of type 2 diabetes. CurrOpinMolTher 12(6): 790-797.
-
Holman RR, Bethel MA, George J, Sourij H, Doran Z, et al. (2016) Rationale and design of the EXenatide Study of Cardiovascular Event Lowering (EXSCEL) trial. Am Heart J 174: 103-110.
-
Gautier JF, Choukem SP, Girard J (2008) Physiology of incretins (GIP and GLP-1) and abnormalities in type 2 diabetes. Diabetes & amp Metabolism 34(S2): 65-72
-
Kim W, Egan JM (2008) The role of incretins in glucose homeostasis and diabetes treatment. Pharmacological Reviews 60 (4): 470-512.
-
Shigeta T, Aoyama M, Bando YK, Monji A, Mitsui T, et al. (2012) Dipeptidyl peptidase-4 modulates left ventricular dysfunction in chronic heart failure via angiogenesis-dependent and -independent actions. Circulation 126: 1838-1851.
-
Kieffer TJ, McIntosh CH, Pederson RA (1995)Degradation of glucose-dependent insulinotropic polypeptide and truncated glucagon- like peptide 1 in vitro and in vivo by dipeptidyl peptidase IV. Endocrinology 136(8): 3585-3596.
-
Asmar M (2011) New physiological effects of the incretin hormones GLP-1 and GIP. Dan Med Bull 58(2): B4248.
-
Skibicka KP (2013) The central GLP-1: implications for food and drug reward. Front Neurosci 7: 181.
-
Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, et al. (2015) Management of hyperglycemia in type 2 diabetes, 2015: a patient- centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 38(1): 140-149.
-
Advisory Committee Briefing Materials: Available for Public Release. Insulin degludec/liraglutide (IDegLira) Treatment to Improve Glycemic Control in Adults with Type 2 Diabetes Mellitus. NDA 208583.
-
Elaine GanszBobo (2010) "FDA Approves New Treatment for Type 2 Diabetes"
-
US Food and Drug Administration (2014) FDA approves weight-management drug Saxenda.
-
Zinman B, Gerich J, Buse J, Lewin A, Schwartz S, et al. (2009) Efficacy and safety of the human glucagon-like peptide-1 analog liraglutide in combination with metformin and thiazolidinedione in patients with type 2 diabetes (LEAD-4 Met+TZD). Diabetes Care 32(7): 1224-1230.
-
Garber A, Henry R, Ratner R, Garcia-Hernandez P, Rodriquez-Pattzi H, et al. (2009) Liraglutide versus glimepiride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomized, 52-week, phase III, double- blind, parallel-treatment trial. Lancet 373(9662): 473-481.
-
Yuan G, Song W, Huang Y, Guo X, Gao Y (2012) Efficacy and tolerability of exenatidemonotherapy in obese patients with newly diagnosed type 2 diabetes: a randomized, 26-week metformin controlled, parallel-group study. Chin Med J 125(15): 2677-2681.
-
Buse JB, Rosenstock J, Sesti G, Schmidt WE, Montanya E, et al. (2009) Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel group, multinational, open-label trial (LEAD-6). Lancet 374(9683): 39-47.
-
Ratner R, Maggs D, Nielsen L, Stonehouse H, Poon T, et al. (2006) Long-term effects of exenatide therapy over 82 weeks on glycemic control and weight in over-weight metformin-treated patients with type 2 diabetes mellitus. Diabetes ObesMetab 8(4): 419-428.
-
Buse J, Henry R, Han J, Kim D, Fineman M, et al. (2004) Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea treated patients with type 2 diabetes. Diabetes Care 27(11): 2628-2635.
-
Buse J, Drucker D, Taylor K, Kim T, Walsh B, et al. (2010) DURATION-1: exenatide once weekly produces sustained glycemic control and weight loss over 52 weeks. Diabetes Care 33(6): 1255-1261.
-
Novo Nordisk A/S (2013) Victoza (liraglutide) package insert.
-
Ban K, Noyan-Ashraf MH, Hoefer J, Bolz SS, Drucker DJ, et al. (2008) Cardioprotective and vasodilatory actions of glucagon-like peptide 1 receptor are mediated through both glucagon-like peptide 1 receptor-dependent and independent pathways. Circulation 117(18): 2340-2350.
-
Nakagawa A, Satake H, Nakabayashi H, Nishizawa M, Furuya K, et al. (2004) Receptor gene expression of glucagon-like peptide-1, but not glucose-dependent insulinotropic polypeptide, in rat nodose ganglion cells. AutonNeurosci 110(1): 36-43.
-
Nystrom T, Gutniak MK, Zhang Q, Zhang F, Holst JJ, et al. (2004) Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am J PhysiolEndocrinolMetab 287(6): 1209-1215.
-
Yamamoto H, Lee CE, Marcus JN, Williams TD, Overton JM, et al. (2002) Glucagon like peptide-1 receptor stimulation increases blood pressure and heart rate and activates autonomic regulatory neurons. J Clin Invest 110(1): 43-52.
-
Gill A, Hoogwerf BJ, Burger J, Bruce S, Macconell L, et al. (2010) Effect of exenatide on heart rate and blood pressure in subjects with type 2 diabetes mellitus: a double-blind, placebo-controlled, randomized pilot study. CardiovascDiabetol 9: 6.
-
Kim M, Platt MJ, Shibasaki T, Quaggin SE, Backx PH, et al. (2013) GLP-1 receptor activation and Epac2 link atrial natriuretic peptide secretion to control of blood pressure. Nat Med 19(5): 567-575.
-
Nikolaidis LA, Elahi D, Hentosz T, Doverspike A, Huerbin R, et al. (2004) Recombinant glucagon-like peptide-1 increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy. Circulation 110(8): 955-961.
-
Ravassa S, Zudaire A, Carr RD, Diez J (2011) Antiapoptotic effects of GLP-1 in murine HL-1 cardiomyocytes. Am J Physiol Heart CircPhysiol 300(4): 1361-1372.
-
Timmers L, Henriques JP, de Kleijn DP, Devries JH, Kemperman H, et al. (2009) Exenatide reduces infarct size and improves cardiac function in a porcine model of ischemia and reperfusion injury. J Am CollCardiol 53(6): 501-510.
-
Noyan-Ashraf MH, Momen MA, Ban K, Sadi AM, Zhou YQ, et al. (2009) GLP-1R agonist liraglutide activates cytoprotective pathways and improves outcomes after experimental myocardial infarction in mice. Diabetes 58(4): 975-983.
-
Nikolaidis LA, Mankad S, Sokos GG, Miske G, Shah A, et al. (2004) Effects of glucagon-like peptide-1 in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion. Circulation 109(8): 962-965.
-
Sokos GG, Bolukoglu H, German J, Hentosz T, Magovern GJ, et al. (2007) Effect of glucagon-like peptide-1 (GLP-1) on glycemic control and left ventricular function in patients undergoing coronary artery bypass grafting. Am J Cardiol 100(5): 824-829.
-
Read PA, Khan FZ, Dutka DP (2012) Cardioprotection against ischaemia induced by dobutamine stress using glucagon like peptide-1 in patients with coronary artery disease. Heart 98(5): 408-413.
-
Kristensen J, Mortensen UM, Schmidt M, Nielsen PH, Nielsen TT, et al. (2009) Lack of cardioprotection from subcutaneously and pre-ischemic administered Liraglutide in a closed chest porcine ischemia reperfusion model. BMC Cardiovasc Dis 9: 31.
-
Sokos GG, Nikolaidis LA, Mankad S, Elahi D, Shannon RP (2006) Glucagon-like peptide-1 infusion improves left ventricular ejection fraction and functional status in patients with chronic heart failure. J Card Fail 12(9): 694-699.
-
Arakawa M, Mita T, Azuma K, Ebato C, Goto H, et al. (2010) Inhibition of monocyte adhesion to endothelial cells and attenuation of atherosclerotic lesion by a glucagon-like peptide-1 receptor agonist, exendin-4. Diabetes 59(4): 1030-1037.
-
Goto H, Nomiyama T, Mita T, Yasunari E, Azuma K, et al. (2011) Exendin-4, a glucagon-like peptide-1 receptor agonist, reduces intimal thickening after vascular injury. BiochemBiophys Res Commun 405(1): 79-84.
-
Gaspari T, Liu H, Welungoda I, Hu Y, Widdop RE, et al. (2011) A GLP-1 receptor agonist liraglutide inhibits endothelial cell dysfunction and vascular adhesion molecule expression in an ApoE-/- mouse model. DiabVasc Dis Res 8(2): 117-124.
-
Bergenstal RM, Wysham C, Macconell L, Malloy J, Walsh B, et al. (2010) Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet 376(9739): 431-439.
-
Courreges JP, Vilsboll T, Zdravkovic M, Le-Thi T, Krarup T, et al. (2008) Beneficial effects of once-daily liraglutide, a human glucagon-like peptide-1 analogue, on cardiovascular risk biomarkers in patients with Type 2 diabetes. Diabet Med 25(9): 1129-1131.
-
Liu H, Hu Y, Simpson RW, Dear AE (2008) Glucagon- like peptide-1 attenuates tumor necrosis factor- alpha-mediated induction of plasminogen [corrected] activator inhibitor-1 expression. J Endocrinol 196(1): 57-65.
-
Shimizu T, Uematsu M, Yoshizaki T, Obata JE, Nakamura T, et al. (2016) Myocardial Production of Plasminogen Activator Inhibitor-1 is Associated with Coronary Endothelial and Ventricular Dysfunction after Acute Myocardial Infarction. J AtherosclerThromb 23(5): 557-566.
-
Zhou SJ, Bai L, Lv L, Chen R, Li CJ, et al. (2014) Liraglutide ameliorates renal injury in streptozotocin-induced diabetic rats by activating endothelial nitric oxide synthase activity via the downregulation of the nuclear factor-κB pathway. Mol Med Rep 10(5): 2587-2594.
-
Ceriello A, Esposito K, Testa R, Bonfigli AR, Marra M,et al. (2011) The possible protective role of glucagon- like Peptide 1 on endothelium during the meal and evidence for an ‘‘endothelial resistance’’ to glucagon- like Peptide 1 in diabetes. Diabetes Care 34(3): 697- 702.
-
Nandy D, Johnson C, Basu R, Joyner M, Brett J, et al. (2014) The effect of liraglutide on endothelial function in patients with type 2 diabetes. DiabVasc Dis Res 11(6): 419-430.
-
Hellstrom PM (2009) GLP-1:broadening the incretin concept to involve gut motility. RegulPept 156(1-3): 9-12.
-
Schirra J, Nicolaus M, Woerle HJ, Struckmeier C, Katschinski M, et al. (2009) GLP-regulates gastroduodenal motility involving cholinergic pathways. NeurogastroenterolMotil 21(6): 609-612.
-
Williams DL (2009) Minireview: finding the sweet spot: peripheral versus central glucagon-like peptide 1 action in feeding and glucose homeostasis. Endocrinology 150(7): 2997-3001.
-
Flint A, Raben A, Astrup A, Holst JJ (1998) Glucagon- like peptide 1 promotes satiety and suppresses energy intake in humans. J Clin Invest 101(3): 515- 520.
-
Raun K, von VP, Gotfredsen CF, Golozoubova V, Rolin B, et al. (2007) Liraglutide, a long-acting glucagon-like peptide-1 analog, reduces body weight and food intake in obese candy-fed rats, whereas a dipeptidyl peptidase-IV inhibitor, vildagliptin, does not. Diabetes 56(1): 8-15.
-
Parkinson JR, Chaudhri OB, Kuo YT, Field BC, Herlihy AH, et al. (2009) Differential patterns of neuronal activation in the brainstem and hypothalamus following peripheral injection of GLP-1, oxyntomodulin and lithium chloride in mice detected by manganese-enhanced magnetic resonance imaging (MEMRI). Neuroimage 44(3): 1022-1031.
-
Perry T, Haughey NJ, Mattson MP, Egan JM, Greig NH (2002) Protection and reversal of excitotoxic neuronal damage by glucagon-like peptide-1 and exendin-4. J PharmacolExpTher302(3): 881-888.
-
Hsieh J, Longuet C, Baker CL, Qin B, Federico LM, et al. (2010) The glucagon-like peptide 1 receptor is essential for postprandial lipoprotein synthesis and secretion in hamsters and mice. Diabetologia 53(3): 552-561.
-
Davies MJ, Donnelly R, Barnett AH, Jones S, Nicolay C, et al. (2009) Exenatide compared with long-acting insulin to achieve glycemic control with minimal weight gain in patients with type 2 diabetes: results of the helping evaluate exenatide in patients with diabetes compared with long-acting insulin (HEELA) study. Diabetes ObesMetab 11(12): 1153-1162.
-
Fonseca V, DeVries JH, Bain SC, Pratley R, Jensen T, et al. (2011) Poster presented at the 21st World Diabetes Congress of the International Diabetes Federation, Dubai, United Arab Emirates.
-
Zander M, Madsbad S, Madsen JL, Holst JJ (2002) Effect of 6-week course of glucagon-like peptide 1 on glycemic control, insulin sensitivity, and b-cell function in type 2 diabetes: a parallel-group study. Lancet 359(9309): 824-830.
-
Pratley R, Nauck M, Bailey T, Montanya E, Cuddihy R, et al. (2011) One year of liraglutide treatment offers sustained and more effective glycaemic control and weight reduction compared with sitagliptin, both in combination with metformin, in patients with type 2 diabetes: a randomised, parallel-group, open-label trial. Int J ClinPract 65(4): 397-407.
-
Pratley RE, Nauck M, Bailey T, Montanya E, Cuddihy R, et al. (2010) Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: a 26- week, randomised, parallel group, open-label trial. Lancet 375(9724): 1447-1456.
-
Garber A, Henry RR, Ratner R, Hale P, Chang C, et al. (2010) Liraglutide, a once-daily human GLP-1 analogue, provides sustained improvements in glycemic control and weight for two years as monotherapy compared with glimepiride in patients with type 2 diabetes. Diabetes ObesMetab 13(4): 348- 356.
-
Jendle J, Nauck MA, Matthews D, Frid A, Hermansen K, et al. (2008) Liraglutide, a once-daily human GLP-1 analog, reduces fat percentage, visceral and subcutaneous adipose tissue and hepatic steatosis compared with glimepiride when added to metformin in subjects with type 2 diabetes. Diabetes; 57(1): A32- 33.
-
Horton ES, Silberman C, Davis KL, Berria R (2010) Weight loss, glycemic control, and changes in cardiovascular biomarkers in patients with type 2 diabetes receiving incretin therapies or insulin in a large cohort database. Diabetes Care 33(8): 1759- 1765.
-
Gutzwiller JP, Tschopp S, Bock A, Zehnder CE, Huber AR, et al. (2004) Glucagon like peptide 1 induces natriuresis in healthy subjects and in insulin-resistant obese men. J ClinEndocrinolMetab 89(6): 3055-3061.
-
Yu M, Moreno C, Hoagland KM, Dahly A, Ditter K, et al. (2003) Antihypertensive effect of glucagon-like peptide 1 in Dahl salt-sensitive rats. J Hypertens 21(6): 1125-35.
-
Ishibashi Y, Matsui T, Takeuchi M, Yamagishi S (2010) Glucagon like peptide-1 (GLP-1) inhibits advanced glycation end product (AGE)-induced up-regulation of VCAM-1 mRNA levels in endothelial cells by suppressing AGE receptor (RAGE) expression. BiochemBiophys Res Commun 391(3): 1405-1408.
-
Ishibashi Y, Nishino Y, Matsui T, Takeuchi M, Yamagishi S (2011) Glucagon-like peptide-1 suppresses advanced glycation end product-induced monocyte chemoattractant protein-1 expression in mesangial cells by reducing advanced glycation end product receptor level. Metabolism 60(9): 1271- 1277.
-
Kannel WB, Kannel C, Paffenbarger RS, Cupples LA (1987) Heart rate and cardiovascular mortality: The Framingham Study. Am Heart J 113(6): 1489-1494.
-
M Monami, DicembriniI, NardiniC, FiordelliI, MannucciE(2014) Effects of glucagon-like peptide-1 receptor agonists on cardiovascular risk: a meta- analysis of randomized clinical trials. Diabetes, Obesity and Metabolism 16(1): 38-47.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study